
Translate this page into:
Unusual proximal femur fracture in children treated with PHILOS plate and review of literature
Address for correspondence: Dr. Mukesh Kumar, Department of Orthopaedics, MMIMSR, Ambala, Haryana, India. E-mail: mukeshmedico@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Kumar M, Chandrabau KK, Bhaskaran VK, Jindal RC. Unusual proximal femur fracture in children treated with PHILOS plate and review of literature. J Orthop Allied Sci 2017;5:6-9.
Abstract
Fractures of the hip are uncommon in children with incidence is less than 1% in all paediatrics fracture. It requires careful attention because of the incidence of complications is high. There is no consensus over ideal treatment of each group, but there are different options for each group has been described in literature, we report a case of unusual proximal femur fracture in ten-year-old girl which is not described in literature in best of our knowledge. A 10 years old girl was brought to us with pain in right hip joint and inability to bear weight on right lower limb after road traffic accident (child was hit by a car while walking on the road). Evaluated and found to have fracture of proximal femur. fracture was fixed with long PHILOS plate, which united in eight weeks duration, implant was removed at 10 month. At present after 14 months, she is able to perform her routine activities comfortably. and her Harris hip score is 95. We propose to add this type of fracture as 5th type of Delbet's classification as the fracture pattern in my patient was not fitting in any group of Delbet's classification and it belongs to proximal femur group and anatomically this fracture pattern was next to type IV fracture. Uncommon fracture of hip in children can be expected, this type of fracture can be added as 5th type in Delbet's classification. Long term outcome and ideal treatment yet to be described.
Keywords
Modified Delbet
PHILOS plate
proximal femur fracture

Introduction
Fractures of the hip are uncommon in children but require careful attention because of the high incidence of complications.[1-3] Delbet's classification is most commonly used to classify proximal femur fracture. Type-II is the most common fracture with incidence of 45% and Type-I is least common hip fracture in children with incidence of 8%, in a review study by Canale and Bourland.[2] Delbet's classification was later used by Colonna[4] to determine the treatment and prognosis of hip fracture in children.
There is no consensus over ideal treatment of each group, but there are different options for each group that has been described in literature.[5]
AVN of femoral head is most common and serious complication of hip fracture in children with incidence of up to 59% of all pediatrics hip fracture.[1] Besides displacement of the fracture,[6] other risk factors for AVN include a Type-I or displaced Type-II fracture and age of more than 10 years.[7] Other complications mentioned are malunion, coxa vara, nonunion, premature closure of physis, and chondrolysis.[8]
Case Report
A 10-year-old girl was brought to us with pain in the right hip joint and inability to bear weight on right lower limb after road traffic accident (child was hit by a car while walking on the road). Child was evaluated and found to have proximal femur fracture which was not fitting in any group according to Delbet's classification [Figure 1].
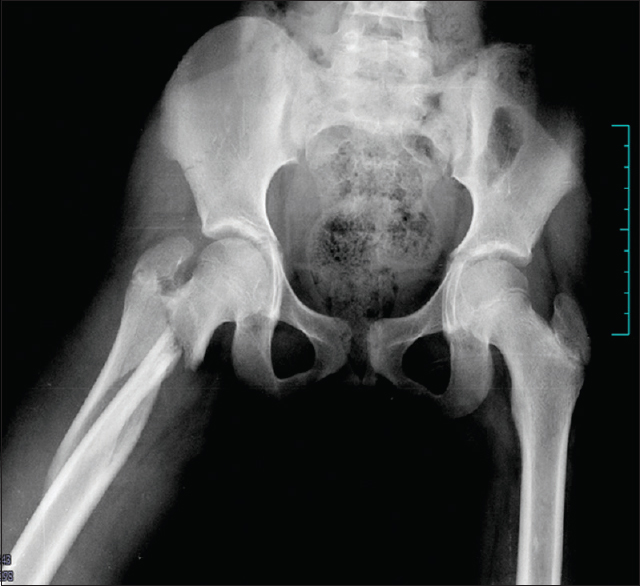
- Radiograph of pelvis with both hips showing fracture of cervicotrochanteric with subtrochanteric extension
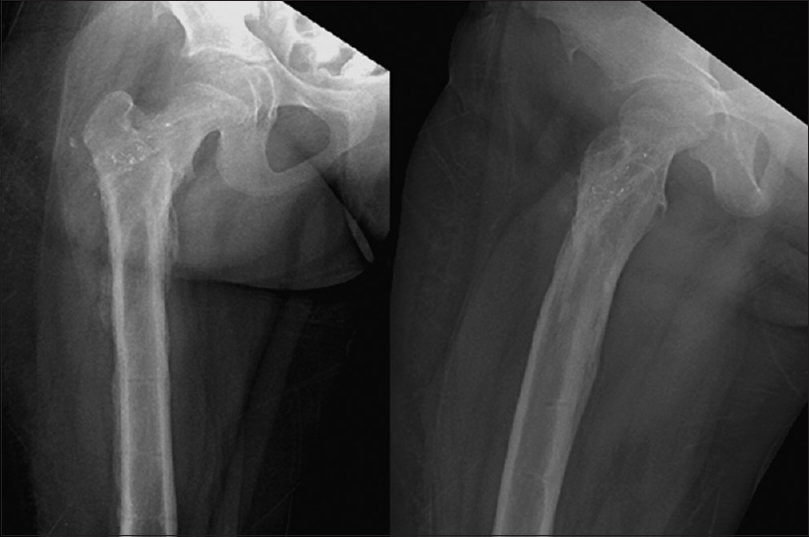
Being a unusual fracture we had difficulty in choosing implants but after discussion with other orthopaedics surgeon we decided to stabilise with long PHILOS (proximal humerus interlocking system) plate and screws. After thorough evaluation and pre anaesthetic clearance, stabilisation with plate and screws was planned. patient was positioned on fracture table, closed reduction was tried but failed. Open reduction was done using hook on medial side and temporarily stabilized with k-wires. Fracture was finally fixed with PHILOS plate and screws through plate. Since gap over cervicotrochanteric region was persisting, we used lag screw above the tip of PHILOS plate to compress the fracture [Figure 2]. Still we were not confident about stability of fracture fixation, so postoperatively rotation stop was given for affected limb and non-weight bearing was advised for 6 weeks followed by partial weight-bearing and full weight-bearing was allowed at 12 weeks [Figure 3]. The patient was on regular follow-up till 10 months post operatively [Figure 4]; by this time, fracture has united well with normal neck shaft angle with Harris hip score of 95 and good functional outcome according to Ratliff. Implant removal was done at ten months. She was allowed to bear weight after one month of implant removal [Figure 5]. At present, after 14 months of follow-up [Figures 6 and 7]. She is able to perform her routine activities comfortably with Harris hip score and functional outcome is comparable to before implant removal.
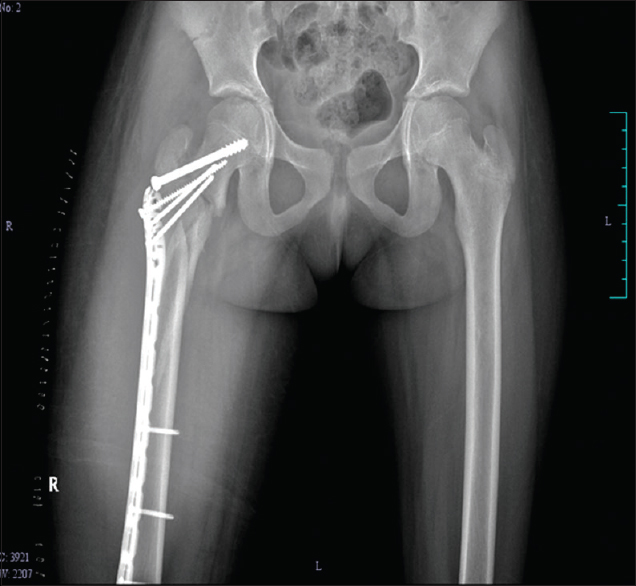
- Radiograph of pelvis with both hips showing fracture fixed with PHILOS plate and partially threaded screw
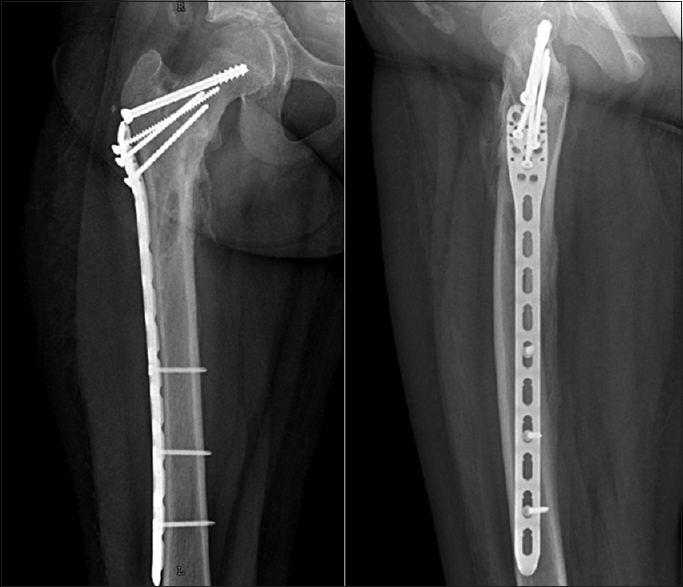
- Radiograph of pelvis with both hips showing implant in situ with uniting fracture at 3 months postoperatively

- Radiograph of pelvis with both hips showing implant in situ with uniting fracture at 10 months postoperative

- Radiograph of pelvis with both hips after implant removal

- Clinical photographs showing range of motion of hip
- Radiograph of pelvis with both hips till last follow.up at 14. months after implant removal
Discussion
Fractures of the head and neck of the femur in children are exceedingly rare, accounting for fewer than 1% of all pediatric fractures,[1] most orthopedic surgeons will treat only a few such fractures in a lifetime.[8] Hip fractures in children can be caused by axial loading, torsion, hyperabduction, or a direct blow to the hip. Almost all hip fractures in children are caused by severe, high-energy trauma. It is usually associated with head injury, pelvic fracture, open femoral shaft fracture, subtrochanteric femoral fracture, facial injury, upper extremity and clavicle injuries, splenic injuries, perineal wounds, and retroperitoneal hematoma.[9] Bagatur and Zorer[10] found five associated injuries in 4 of their 17 patients, including forearm, humeral, pelvic, and tibial fractures. All but 1 of the 17 fractures was caused by high-energy mechanisms. Hip fracture in children may lead to AVN of femoral head, coxa vara, nonunion, or delayed union if not treated properly.[1,11] Therefore, current management is directed at early, anatomic reduction of these fractures with stable internal fixation and supplemental external stabilization (casting), with the goal of minimizing devastating late complications.
The classification in children differs from those in adults, the classification commonly used for hip fracture in children is Delbet's classification, which includes four types of fracture, Type-I, transepiphyseal, with (IB) or without (IA) dislocation from the acetabulum; Type-II, transcervical; Type-III, cervicotrochanteric; and Type-IV, intertrochanteric.
Type-II being the most common type followed by Type-III, IV, and I,[2] AVN of femoral head is most commonly associated with Type-I and II. Type-IV fracture is having more favorable overall outcome.
There is no consensus made for ideal treatment for each type of fracture, but the treatment of these fractures depends on type of fracture, age of the child, displacement, and angle of the fracture line.
For Type-I fracture, closed reduction can be attempted followed by hip Spica and close follow-up, in failed cases, open reduction and stable fixation are better option.[12]
Type-II and III displaced fractures should always be treated with anatomical reduction and stable fixation to avoid devastating complications, for undisplaced fracture closed reduction and hip spica can be tried with close follow-up; if fails, open reduction and internal fixation is preferable.[12]
For Type-IV fracture, good results can be expected after closed treatment of most intertrochanteric fractures, regardless of displacement. Traction and spica cast immobilization are effective.[8] Failure to maintain adequate reduction and polytrauma are indications for internal fixation.
The fracture pattern of my patient was not fitting in any type of Delbet's classification. This fracture pattern belongs to proximal femur group and anatomically this fracture pattern was next to Type-IV fracture. The treatment for this fracture also is based on the principle of proximal femur treatment. On the basis of above facts we suggest a modification of Delbet's classification by adding this type of fracture as a fifth group [Figure 8] – Modified Delbet's classification, Type-I-transepiphyseal with (type IB) or without (type IA) dislocation of the femoral head from the acetabulum.; Type-II-transcervical; Type-III-basicervical (cervicotrochanteric); Type-IV-intertrochanteric (Pertrochanteric); and Type-V-cervicotrochanteric with subtrochanteric extension.
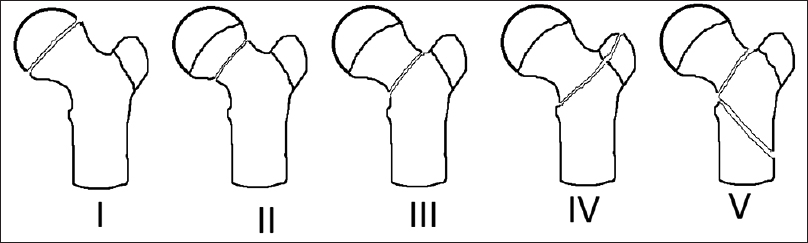
- Modified Delbet's classification: Type-I-transepiphyseal with (type IB) or without (type IA) dislocation of the femoral head from the acetabulum; Type-II-transcervical; Type-III-basicervical (cervicotrochanteric); Type-IV-intertrochanteric (Pertrochanteric); and Type-V-cervicotrochanteric with subtrochanteric extension
Conclusion
Uncommon fracture of hip in children can be expected, the cervicotrochanteric with subtrochanteric extension can be treated with long PHILOS plate with favorable outcome. This type of fracture can be added as 5th type in Delbet's classification. Long-term outcome and ideal treatment are yet to be described.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Fractures of the neck of the femur in children. J Bone Joint Surg Br 1962:44-42.:528-42.
- [CrossRef] [PubMed] [Google Scholar]
- Fracture of the neck and intertrochanteric region of the femur in children. J Bone Joint Surg Am. 1977;59:431-43.
- [CrossRef] [Google Scholar]
- Complications associated with fracture of the neck of the femur in children. J Pediatr Orthop. 1992;12:503-9.
- [CrossRef] [PubMed] [Google Scholar]
- Fractures of the neck of the femur in children. Am J Surg. 1929;6:793-7.
- [CrossRef] [Google Scholar]
- Paediatric hip fractures: A systematic review of incidence, treatment options and complications. Acta Orthop Belg. 2010;76:7-13.
- [Google Scholar]
- Fractures of the hip in children. Orthop Clin North Am. 2006;37:223-32.
- [CrossRef] [PubMed] [Google Scholar]
- Risk factors for avascular necrosis after femoral neck fractures in children: 25 Cincinnati cases and meta-analysis of 360 cases. J Orthop Trauma. 2006;20:323-9.
- [CrossRef] [PubMed] [Google Scholar]
- Fractures of the head and neck of the femur in children. J Bone Joint Surg Am. 1994;76:283-92.
- [CrossRef] [PubMed] [Google Scholar]
- Fractures of the neck of femur in children: An experience at the Aseer Central Hospital, Abha, Saudi Arabia. Injury. 2002;33:823-7.
- [CrossRef] [PubMed] [Google Scholar]
- Complications associated with surgically treated hip fractures in children. J Pediatr Orthop B. 2002;11:219-28.
- [CrossRef] [Google Scholar]
- Fractures of the neck of the femur in children. J Bone Joint Surg Am. 1971;53:1165-79.
- [CrossRef] [Google Scholar]
- Heckman, Charles court-brown, Rockwood and Greens, Fractures in Children. (6th). Philadelphia, USA: Lippincott Williams and Wilkins; 2006. p. :861-77.s. Ch. 21
- [Google Scholar]




