
Translate this page into:
Surgical outcome of distal end radius fractures by ligamentotaxis
Address for correspondence: Dr. C. Vishwanath, No. 43, Maruthi Nilaya, 1st Main, DB Sandra, Vidyaranyapura (Post), Bengaluru - 560 097, Karnataka, India. E-mail: drvishwanathc24@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Vishwanath C, Harish K, Gunnaiah KG, Ravoof A. Surgical outcome of distal end radius fractures by ligamentotaxis. J Orthop Allied Sci 2017;5:68-73.
Abstract
BACKGROUND AND OBJECTIVES:
Preservation of the articular congruity is the principle prerequisite for successful recovery, following distal radius fractures. The best method of obtaining and maintaining an accurate restoration of articular anatomy, however, remains a topic of considerable controversy. The main aim of this study is to evaluate the results obtained by treatment of distal end radius fractures by external fixation.
MATERIALS AND METHODS:
This is a prospective controlled study; fifty cases of unstable distal end radius fractures with/without intra-articular extension were treated with uniplanar static type of external fixation using the principle of ligamentotaxis and augmentation by K-wires from July 2013 to December 2016 at our tertiary rural hospital. The age group of the patients is 18–60 years, external fixator was applied for a duration of 6–8 weeks, and cases were followed up for an average of 6–10 months postoperatively.
RESULTS:
Assessed as per Demerit Point System of Gartland and Werley (modified by Sarmiento 1975) for functional results and criteria for anatomical results by Sarmiento (1975) at the end of 6–8 months of follow-up. Excellent anatomical result was seen in 11 patients, good result seen in 32 patients, and fair result seen in five patients with two poor result patients.
CONCLUSION:
External fixation and ligamentotaxis provide better functional and anatomical results in comminuted intra-articular and unstable extra-articular wrist injuries. The functional result of treatment of distal radius fractures not only depends on the anatomical restoration of the articular surface but also depends on the associated soft tissue injuries and articular damage.
Keywords
External fixation
extra-articular fracture
intra-articular fracture
radius fracture

Introduction
Fractures of the distal radius continue to be the most common skeletal injuries treated by an orthopedic surgeon. In fact, these injuries are the most common fractures of the upper extremity and account for approximately 1/6th (16%) of all fractures seen and treated in emergency rooms.[1,2] Distal radius fractures disturb the mechanical foundation of the human's most elegant tool, the hand. The same ligaments, retinaculae, tendons, and periosteum that envelop the fracture which are the surgical barriers for open reduction of the fracture fragments, help achieve reduction of the fracture by ligamentotaxis.[3] Many fractures of the distal aspect of the radius are relatively uncomplicated and are effectively treated by closed reduction and immobilization in cast. However, unstable/intra-articular fractures can jeopardize the integrity of the articular congruence and/or kinematics of these articulations.
A consensus prevails that vast majority (nearly 90%) of distal radius fractures are articular injuries resulting in disruption of both the radiocarpal and radioulnar joints.[4] Intra-articular fractures are inherently unstable, difficult to reduce anatomically and to immobilize in closed plaster of Paris (POP) support and are associated with high rate of complications.[3,5] With the changing mode of injury, fracture of the distal end radius occurring in younger patients, increasing functional demands of the patients, better understanding of the fracture pattern, advances in biomechanics of the wrist, and availability of treatment-oriented classification system, it seems we have to look beyond the conventional teaching that they all do well ultimately. Preservation of the articular congruity is the principle prerequisite for successful recovery.[4]
External fixation is generally accepted as superior to plaster immobilization in young patients with intra-articular comminuted displaced distal radius fracture.[6] The successful use of external fixation in the management of unstable intra-articular fractures necessitates careful assessment of the fracture pattern, appropriate patient selection, meticulous surgical technique, appropriate choice of fixation devices, judicious augmentation with internal fixation and bone grafting, careful postoperative monitoring, and aggressive early rehabilitation.[7-9]
The main aim of this study is to evaluate the results obtained by the treatment of distal end radius fractures by external fixation in terms of duration of immobilization in external fixation and restoration of anatomy of distal end radius (radial length, palmar tilt, and radial angulation) and to know the effectiveness in allowing early motion of digits and prevention of deformity and disability due to malunion.
Materials and Methods
All the patients attending the outpatient and inpatient Department of Orthopaedics at a tertiary rural hospital with fracture of distal end radius and fulfilling the inclusion criteria during the study period of July 2013 to December 2016 were included.
Study design
This was a prospective study of cases fulfilling the inclusion and exclusion criteria during the study period of July 2013 to December 2016.
Inclusion criteria for the proposed study were unstable intra-articular distal end radius fractures with increased volar/dorsal communition and >2 mm spread/depression of articular surface with >10° angulation of major fragments; fractures extending into radiocarpal/radioulnar joints or with ulnar fractures (Frykman's III, VIII); unstable extra-articular fractures with significant metaphyseal comminution and failure to maintain reduction after initial attempt at closed reduction and cast application; and open fractures of distal end radius to facilitate wound care and bilateral distal end radius fractures.
Exclusion criteria for the proposed study were the patient presents with malunited fractures; cases with neurovascular deficit; and compound fracture cases with associated neurological deficit and fractures occurred at the metaphysis level and proximally.
In the preoperative period, splint age with POP slab and elevation was carried out which facilitate fracture reduction and precision of pins while applying external fixator.[10] Fractures were classified according to the Frykman classification.
Instability[7] was recognized based on the initial displacement as follows:
>20° dorsal angulation
Marked dorsal metaphyseal comminution
Radial shortening >10 mm.
Secondary instability is said to be present when closed reduction and cast immobilization fails to maintain initial reduction and is found if residual dorsal angulation >10°, residual radial shortening >5 mm, >2 mm step-off or displacement of articular fragments, intra-articular fractures, loss of radial inclination >20°, metaphyseal comminution of >50% diameter of radius, associated ulnar fracture, significant osteoporosis.[11-13]
Criteria for acceptable reduction (Melone[2]) were as follows:
Follow-up and evaluation
The external fixation device is left in place for an average of 5–8 weeks; still both clinical and radiological evidence of healing are seen. The fixator was removed as outpatient procedure under sedation. After removal of external fixator below/elbow POP slab/splint was applied for 2 weeks which was removed intermittently for exercises 8–10 weeks postoperatively, strengthening exercises were begun [Figures 1-3].
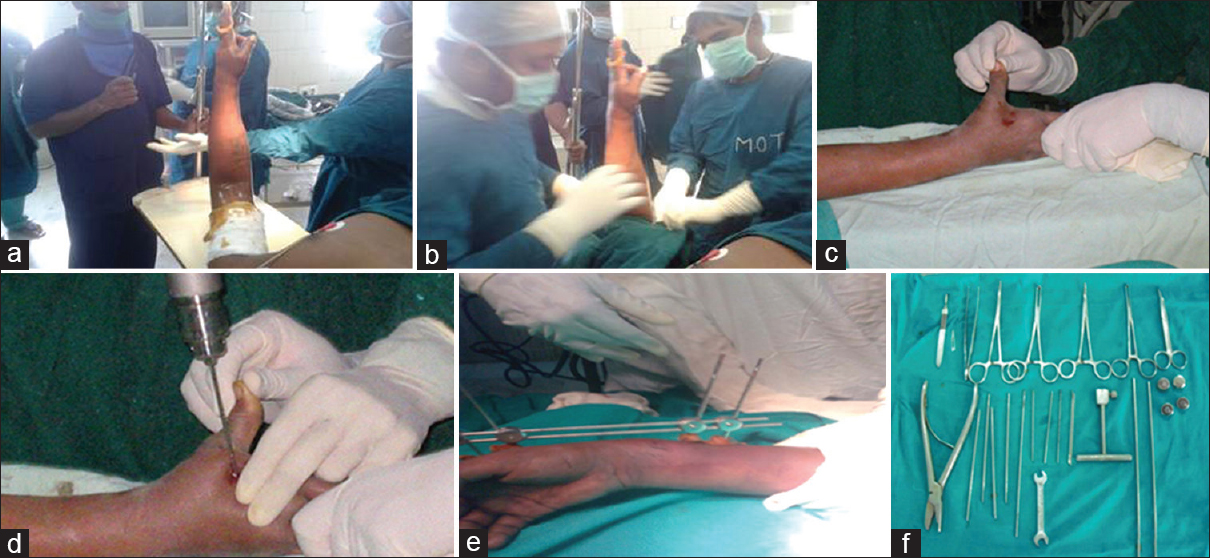
- (a) Surgical technique: Painting of the limb. (b) Surgical technique: Draping of the limb. (c) Surgical technique: Stab incision. (d) Surgical technique: Metacarpal pinning. (e) Surgical technique: External fixation applied. (f) Surgical technique: Instrumentation
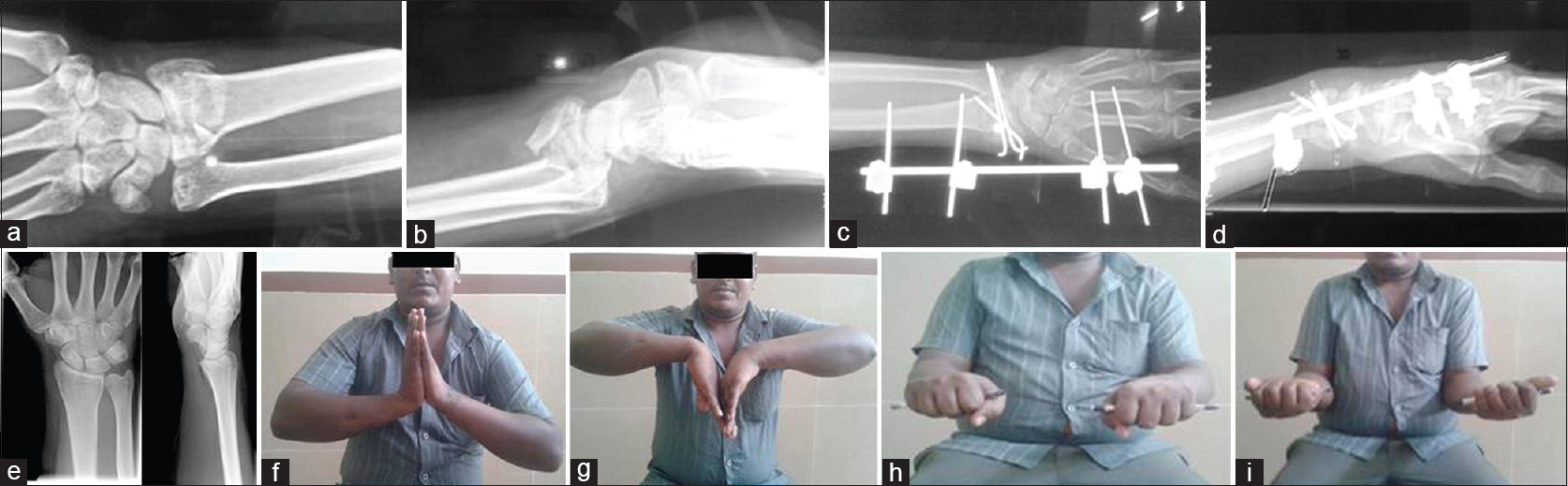
- (a) Case series - 1: Preoperative anteroposterior view. (b) Case series – 1: Preoperative lateral view. (c) Case series – 1: Postoperative anteroposterior view. (d) Case series – 1: Postoperative lateral view. (e) Case series – 1: Union 16 weeks. (f) Case series – 1: Dorsiflexion at 2 months. (g) Case series – 1: Palmar flexion at 2 months. (h) Case series – 1: Pronation at 2 months. (i) Case series – 1: Supination at 2 months
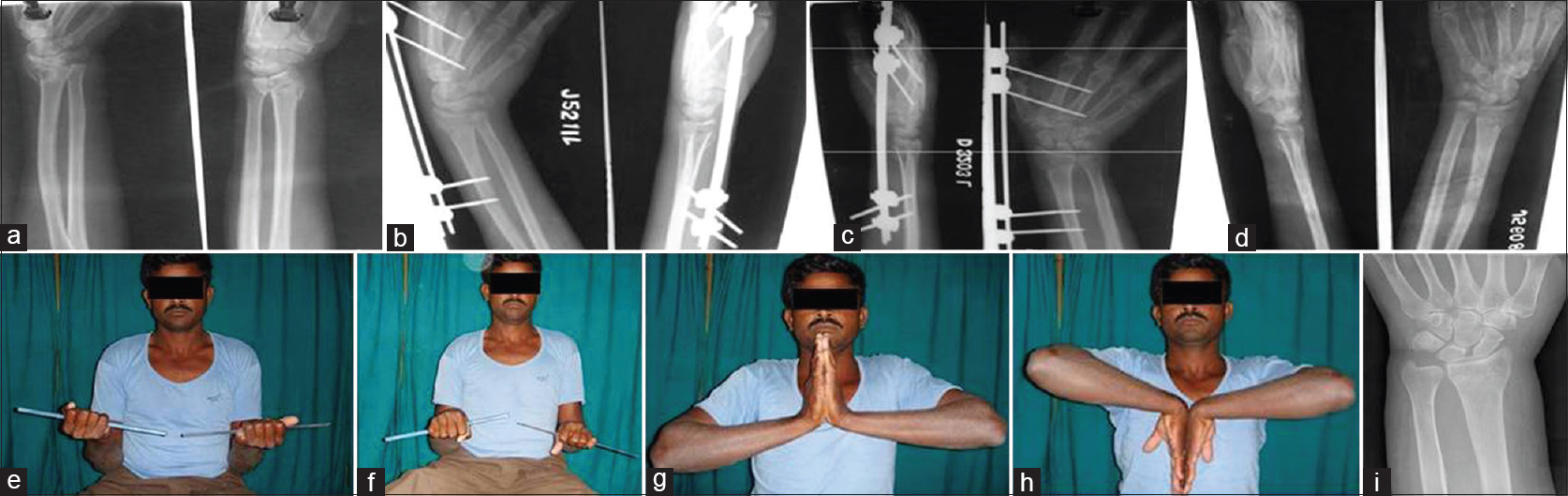
- (a) Case series – 2: Preoperative anteroposterior and lateral views. (b) Case series – 2: Postoperative anteroposterior and lateral views. (c) Case series – 2: Postoperative 6 weeks. (d) Case series – 2: Postoperative 3 months. (e) Case series – 2: Supination at 3 months. (f) Case series – 2: Pronation at 3 months. (g) Case series – 2: Dorsiflexion at 3rd month. (h) Case series – 2: Palmar flexion at 3rd month. (i) Case series – 2: X-ray showing fracture union
Majority of cases were followed up to 6 months. The maximum follow-up in our study was 50 weeks and minimum was up to 11 weeks. The final results of all patients were evaluated as per:
Results
In our study, the maximum patients sustained distal end radius fractures are in the age group of 20–30 (34%) followed by age groups of 41–50 (26%) and 31–40 (24%) years with a mean age of the patients being 54 years with male population predominantly injured in 38 (76%) than the female (12 patients) population (24%). In this study, 35 patients sustained the right-sided injury (70%) and 15 patients with left-sided injury (30%). Thirty-two patients (64%) sustained injury with road traffic accident, whereas 18 patients (36%) were injured in falls. In our study, 14 (28%) patients sustained associated fractures than other 36 (72%) patients, who sustained isolated distal end radius fracture. Eighty percent of the patients underwent surgery within 48 h of the injury.
In this case study of fifty patients, 13 patients (26%) were treated with 6 weeks fixation, whereas 15 patients (30%) were continued with 7 weeks of fixation and 22 patients (44%) were treated with a period of 8 weeks. In this study, under Frykman's classification of distal end radius fractures, there were no patients in Types I and II treated with ligamentotaxis. Eight patients were classified in Type III fractures, four patients in Type IV, three patients in Type V classification, nine patients in Type VI group, 17 patients in Type VII, and seven patients in Type VIII classification [Table 1]. In our series, ten patients were found to be with a loss of radial length of −2 mm, 26 patients were suffered with −1 mm loss of radial length, and 14 patients had no loss of radial length at all. In twenty patients, seven patients were found to with rate of union in 8–10 weeks, 12 patients were found radiological union evident on 11–13 weeks, 23 patients were found radiological union in 14–17 weeks, eight patients were found radiological union in 18–20 weeks, and no case of delayed or nonunion was reported. Fourteen patients (28%) of the total fifty patients have reported having pain on exertion and 36 patients (72%) had no such complaints [Table 2].


According to Gartland and Werley score for the outcome, 11 patients (22%) had excellent result, 32 patients (64%) had good result, 5 (10%) patients had fair result, and 2 (04%) patients had poor result [Table 3].

Discussion
Although Abraham Colles was evidently satisfied with the results of his treatment of distal radial fractures in 1814, more recent authors have drawn attention to the high prevalence of unsatisfactory results.
In 1952, DePalma hypothesized that a residual dorsal tilt of the distal end of the radius of >5° led to a poor result.[11] found that immobilization of a distal radial fracture in a cast resulted in a 60% loss of reduction and an unsatisfactory result with regard to pain and loss of function in nineteen (32%) of sixty patients.[17]
Cole and Obletz documented radial shortening of 3 mm or more in 22 (67%) of 33 patients and radial shortening of 6 mm or more in 11 patients (33%) after fixation with pins and plaster.[10]
Clyburn et al. reported radial shortening of 5 mm or more in 20 (25%) of eighty patients who had been managed with the same technique; a complication led to a reoperation in 13 patients (16%).[18]
Kliena et al. found that loss of volar tilt after a distal radial fracture led to progressive load on the ulnocarpal and radioscaphoid articulations, which caused pain and early degenerative disease.[19] Taleisnik and Watson reported an association between malunion of the distal end of the radius and dynamic midcarpal instability.
Unsatisfied with the available methods of treatment, Cooney et al., in 1979, critically reviewed external fixation for the treatment of distal radial fractures and reported a good result for 51 (85%) of sixty patients, with decreased radial shortening and improved volar tilt. Since then, external fixation has become a popular and reliable method for the treatment of these frequently seen fractures. A common algorithm for unstable distal radial fractures is external fixation, supplemental fixation with Kirschner wires, and frequently, the use of a bone graft or bone substitute.[16]
The external fixator is a versatile tool in the treatment of intra-articular fractures of the distal radius.[1] Our standard reduction procedure is similar to the conservative management of these fractures. Continued traction results in controlled distraction of the fracture and facilitates manipulation. This technique is simpler than other techniques. The procedure is performed during a short hospital stay.[3]
The external fixator is reliable in terms of maintaining reduction of axes as well as of radial length. Simple intra-articular fractures with dorsoulnar fragments can be reduced with ligamentotaxis.[20,21]
In our study, among fifty patients, excellent results were obtained in 11 patients, good results in 32 patients, fair results in five patients, and poor result in two patients. Overall, we had a high rate of favorable results and low rate of complications.
The relatively long period of immobilization (6–8 weeks) had no adverse effects on the long-term functional outcome. The fixator can therefore be left according to the radiologic evidence of fracture healing.
Our prospective study of the results of distal radius fractures treated by external fixation emphasizes that:
External fixation for distal radius fracture is a safe and reliable method in terms of fracture fixation, with good functional results and a low complication rate, in particular when external fixation is the primary treatment
Eight weeks of fixation are well tolerated
External fixation is not an adequate tool to maintain volar tilt.
Conclusion
External fixation of the distal radius has evolved from its early beginnings in pins and plaster fixation. The current designs of fixators are well established and can be used to reliably treat many fractures about the wrist.[19] The external fixator is simple and inexpensive. It effectively stabilizes fractures yet allowing for hand motion and prevents stiffness. When intra-articular fractures are treated by conventional methods, pain and restriction of joint motion are not uncommon, whereas when treated by ligamentotaxis by static external fixator, anatomical reduction is predictably achieved at fracture site. Although some cases have residual joint stiffness, pain and arthritis can be prevented. Limitations of the study include volar and dorsal bartons fractures which were treated with precontured locking plates.
The significance of this study is to conclude that comminuted intra-articular fractures at distal end of radius need external fixator to have achievement of good anatomical reduction and achievement of stable fixation. “Good anatomical restoration always leads to good functional end results.”
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
This study was supported by the Hospital Medical Records.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Current concepts review-fractures of the distal end of the radius. J Bone Joint Surg Am 2009:461-9.:73-9.
- [CrossRef] [Google Scholar]
- Distal radius fractures: Patterns of articular fragmentation. Orthop Clin North Am. 1993;24:239-53.
- [CrossRef] [PubMed] [Google Scholar]
- Fractures of the distal aspect of the radius: Changes in treatment over the past two decades. Instr Course Lect. 2003;52:185-95.
- [Google Scholar]
- Intra-articular fractures of the distal end of the radius in young adults. J Bone Joint Surg Am. 1986;68:647-59.
- [CrossRef] [Google Scholar]
- External fixation and recovery of function following fractures of the distal radius in young adults. Injury. 1988;19:235-8.
- [CrossRef] [PubMed] [Google Scholar]
- External fixation of distal radius fractures. Indications and technical principles. Orthop Clin North Am. 1993;24:255-64.
- [CrossRef] [Google Scholar]
- Gray's Anatomy – The Anatomical Basis of Clinical Practice. (41st). Amsterdam: Elsevier Churchill Livingstone Publication; 2015.
- [Google Scholar]
- Rockwood and Green's Fractures in Adults. Ch. 20. (7th). Walnut Street Philadelphia, PA 19106 USA: Lippincott Williams and Wilkins Publication; 2011. p. :815-67.:830-67.
- [Google Scholar]
- Comminuted fractures of the distal end of the radius treated by skeletal transfixion in plaster cast. An end-result study of thirty-three cases. J Bone Joint Surg Am. 1966;48:931-45.
- [CrossRef] [Google Scholar]
- The history and evolution of percutaneous pinning of displaced distal radius fractures. Orthop Clin North Am. 1993;24:287-300.
- [CrossRef] [PubMed] [Google Scholar]
- Colles' fractures. functional bracing in supination. J Bone Joint Surg Am. 1975;57:311-7.
- [CrossRef] [Google Scholar]
- Fractures of the distal radius. A modern treatment-based classification. Orthop Clin North Am. 1993;24:211-6.
- [CrossRef] [Google Scholar]
- Fractures of the distal radius: Operative treatment. Instr Course Lect. 1993;42:73-88.
- [Google Scholar]
- Imaging techniques for distal radius fractures and related injuries. Orthop Clin North Am. 1993;24:217-28.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of healed Colles' fractures. J Bone Joint Surg Am 1951:33-907.:895-907.
- [CrossRef] [Google Scholar]
- Dynamic external fixation for comminuted intra-articular fractures of the distal end of the radius. J Bone Joint Surg Am. 1987;69:248-54.
- [CrossRef] [Google Scholar]
- Results of transarticular fixator application in distal radius fractures. Injury. 2000;31(Suppl 1):71-7.
- [CrossRef] [PubMed] [Google Scholar]
- Unstable articular fractures of the distal radius. comparative techniques of ligamentotaxis. Orthop Clin North Am. 1993;24:275-86.
- [CrossRef] [Google Scholar]
- Computed tomography scanning with image reconstruction in evaluation of distal radius fractures. J Hand Surg Am. 1994;19:720-7.
- [CrossRef] [PubMed] [Google Scholar]




