
Translate this page into:
Single-stage posterior-only debridement and transpedicular screw fixation for dorsolumbar tuberculosis: A prospective study of twenty cases
Address for correspondence: Dr. Ashish Balkrishna Patidar, 127 Amarnath Avenue, Indore Road, Ujjain - 456 001, Madhya Pradesh, India. E-mail: patidarashish1978@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Patidar AB, Mehta RP, Sharma SK, Vyas GB, Singh V, Ramchandra O. Single-stage posterior-only debridement and transpedicular screw fixation for dorsolumbar tuberculosis: A prospective study of twenty cases. J Orthop Allied Sci 2017;5:74-9.
Abstract
BACKGROUND:
India bears the highest burden of tuberculosis (TB), i.e., about one-fourth of the total burden. Of the musculoskeletal TB, spinal TB affects half of the patients. Pharmacological treatment in the form of AKT is the mainstay of treatment of spinal TB, but surgery has its own role to play as an adjunct to AKT in selected cases. Various surgical methods and approaches are mentioned in literature. We studied the efficacy and safety of posterior only approach for decompression and internal fixation in treating thoracic and lumbar spinal TB in adults.
MATERIALS AND METHODS:
In this prospective randomized control study, we treated twenty patients with thoracic-lumbar TB with single-stage posterior only debridement, decompression, and transpedicular screw fixation. Preoperative and postoperative C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), kyphosis angle, visual analog scale (VAS) score and Frankel neurological grading, intraoperative blood loss, and duration of surgery were compared. Correction in kyphosis angle and loss of kyphosis angle at final follow-up was assessed.
RESULTS:
Sixteen male and four female patients with mean age 37.9 years were treated. Average follow-up was 14.95 months. Thirteen patients had two level involved; seven had single level. The average duration of surgery was 155 min (standard deviation [SD] 23.951). Preoperative average increase in ESR was 39.4 mm/h (SD 9.046) and 24.15 mm/h (SD 3.787) at 3 weeks. Average preoperative CRP was 15.7 mg/L (SD 5.398) and 9.05 mg/L (SD 3.456) at 3 weeks. Average preoperative kyphosis angle was 24.7° (SD 6.822) corrected to an average of 10.1° (SD 3.932) postoperative. At final follow-up, there was a mean loss of 1.4° of kyphosis angle. The average blood loss was 722.75 ml; the average duration of surgery was 228.5 min. The pain VAS dropped significantly from 7.05 (SD 1.468) to 3.9 (SD 1.209). At final follow-up, VAS was 1.7 (SD 0.864). All the patients had good neurological recovery except one.
CONCLUSIONS:
Single-stage posterior-only procedure is safe and effective for management of thoracolumbar spinal TB.
Keywords
Posterior instrumentation
posterior only approach
Pott's spine
thoracolumbar tuberculosis

Introduction
Tuberculosis (TB) of spine is prevalent in developing countries and is considered a disease affecting people from low socioeconomic groups.[1,2] Spinal TB affects around half of all patients with musculoskeletal TB. The intervertebral disc and the end plates of the adjacent superior and inferior vertebral bodies are often involved in TB; severe destruction of these elements often leads to kyphotic deformities.[3,4]
Anterior decompression and fixation have been long considered as the gold standard for treatment of TB of spine.[5-7] More operation time, more blood loss and greater duration of hospitalization are its disadvantages. In addition, anterior debridement may reduce the biomechanical stability of the spine, and it is common to find residual kyphosis at the end of treatment. Thus, anterior debridement combined with posterior fusion, and fixation was developed. However, the combined procedures are also associated with a longer operation time, greater blood loss, more postoperative complications, and longer hospital stay.[8,9]
Recently, the posterior approach has gained popularity based on the principle of adequate debridement and stable fixation with much lower complication rates. However, complications resulting from damage to the posterior spinal column due to the posterior approach reduce the surgical effect and affect the patient's quality of life.
The purpose of our clinical study is to investigate the efficacy and safety of treating thoracic and lumbar spinal TB in adults through a posterior only approach debridement and internal fixation.
Materials and Methods
After obtaining permission from the Ethical Committee of the Institution, from March 2014 to March 2016, we studied twenty patients with thoracic and lumbar TB at a tertiary care hospital. Diagnosis of active TB was made based on clinical symptoms, thorough general and local examination, laboratory findings (complete blood count, erythrocyte sedimentation rate [ESR], C-reactive protein [CRP], and sputum for acid-fast bacilli [AFB]) and radiographic evidence (X-ray dorsolumbar and lumbosacral spine, chest X-ray, and magnetic resonance imaging). Patients who had one of these manifestations were confirmed postoperatively through laboratory tests such as AFB staining, bacterial cultures, polymerase chain reaction, Gene Xperts. On confirmation of diagnosis, all patients were put on antitubercular treatment (4HRZE + 8HRE).
Patient's pain was assessed on the basis of ten-point visual analog scale (VAS) score, and the neurological status was assessed with Frankel grading.
The radiographic assessment included preoperative kyphotic angle which was measured on X-ray by Cobb's method as the angle between the upper end plate and the lower end plate of the infected level.
Inclusions
Patients of all ages, both sexes, presenting with newer onset or with the progressive neurological deficit, with spinal instability, not responding to AKT for at least 6 weeks, with epidural abscess compressing the dural sac or with intractable pain.
Exclusions
Patients with more than two level involvement and those with kyphosis angle more than 60° were excluded as correction of such acute angle may alter the neurological outcome.
Operative technique
Under general anesthesia in prone, extraperiosteal dissection was performed through a midline incision to expose the posterior spinal elements. The dissection exposed an adequate number of vertebrae two above and two below the involved segments. Pedicle screws were then inserted under fluoroscopic guidance into the normal vertebrae. On one side, a temporary rod that had been contoured to accommodate the deformity was applied to maintain spinal stability and avoid cord injury during decompression and debridement. At the thoracic level, we performed costotransversectomy and ligated the segmental vessles carefully. Root was sacrificed only in cases of thoracic spine where cage was inserted. Paravertebral and epidural abscess was drained, and thorough debridement was done until fresh bleeding was seen. The same procedure was carried out on opposite side if required. Tissue from the diseased area was harvested for histopathological confirmation of disease. Cage with graft was inserted where required. Opposite side contoured rod was fixed and carefully gradual correction of kyphosis was done. After wash with normal saline, streptomycin powder 1 g was put locally. Wound was closed in layers over drain.
Postoperative management and follow-up
The drain was removed at 48 h; dressings were done on day 2, day 5, day 8, and day 12. Sutures were removed at day 14. Log rolling was started after drain removal, and bedside sitting was started with Taylors brace applied. Depending on the neurological recovery and patient comfort, patient was ambulated on wheelchair, crutches, or walker. Unassisted ambulation was permitted only after 6 weeks. Postoperative ESR and CRP were done at 3 weeks and 3 months. Patients were followed-up at monthly intervals, and at every follow-up, patient's neurological status, VAS score, and kyphosis angle were calculated.
The efficacy of the treatment was concluded on the basis of following variables: intraoperative blood loss, duration of surgery, complications, postoperative kyphosis correction, neurological recovery as graded by Frankel grading, improvement in VAS scores, and loss of kyphosis at final follow-up.
Results
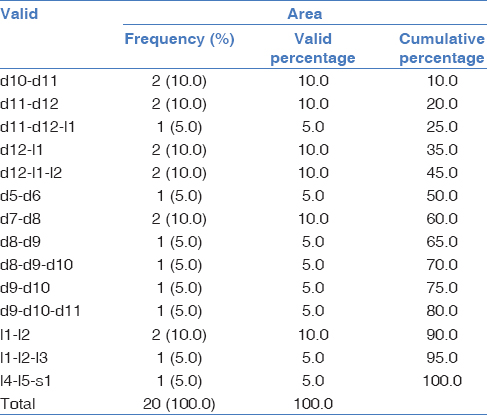
We treated 20 patients of which 16 were male, and 4 were female with minimum age of 16 years and maximum of 57 years (mean 37.9 years). Average follow-up was 14.95 months with maximum 22 months and minimum of 8 months. Seven patients had two level involved while 13 had disease at single level. The average duration of surgery was 155 min (standard deviation [SD] 23.951) [Table 1].
The preoperative average rise in ESR was 39.4 mm/h (SD 9.046) which significantly dropped down to 24.15 mm/h (SD 3.787) at 3 weeks, and in all patients, it returned to normal at 3 months.
The average preoperative rise in CRP was 15.7 mg/L (SD 5.398) which dropped to an average CRP of 9.05 mg/L (SD 3.456) at 3 weeks and was normal at final follow-up.
Average preoperative kyphosis angle was 24.7° (SD 6.822) which could be corrected to an average of 10.1° (SD 3.932) postoperative. At final follow-up, there was a mean loss of 1.4° of kyphosis angle.
The average blood loss was 722.75 ml; the average duration of surgery was 228.5 min.
The pain VAS dropped significantly from 7.05 (SD 1.468) to 3.9 (SD 1.209). At final follow-up, VAS was 1.7 (SD 0.864) [Table 2].

The neurological grading as per Frankel grading was as follows [Table 3].

No neurological deterioration was found in the study postoperatively. Five patients of Frankel grade-C improved to grade-E except one which improved to grade D. All patients with grade-D improved to grade-E except one which did not show any improvement. Patient with grade A improved only to grade C at last follow-up.
Complications
Two patients required observation in the Intensive Care Unit for 24 h postoperatively because of excessive intraoperative blood loss. Two patients presented with wound gaping and were treated with freshening of edges and resuturing under antibiotic coverage. Cage with graft was inserted in three cases where corresponding roots were sacrificed.
No hardware failure was observed in any case till the last follow-up [Figure 1a-d - Case 1 and 2a-e - Case 2].
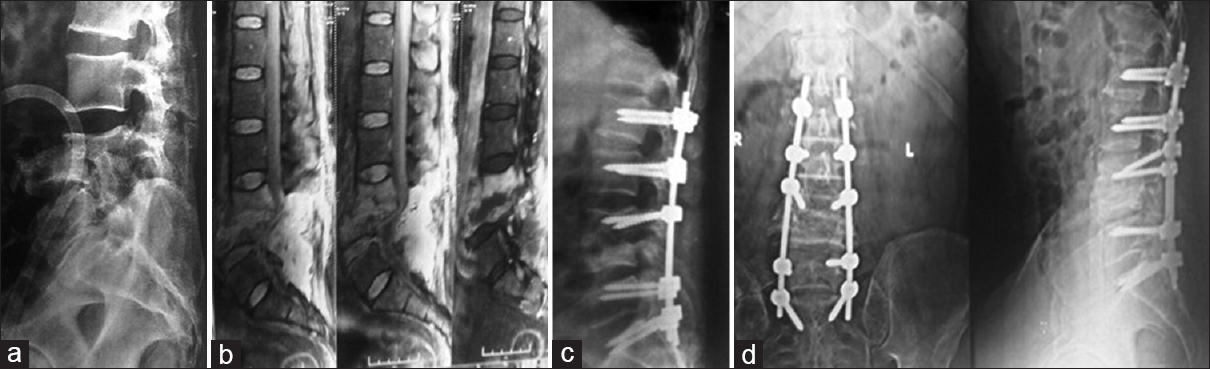
- (a) X-ray of 60-year-old male patient with L3–L4 spondylodiscitis. (b) Magnetic resonance imaging showing pre and paravertebral pus collection. (c) X-ray lateral view showing fixation at the level and two levels above and below. (d) Eight months follow-up X-ray showing consolidation
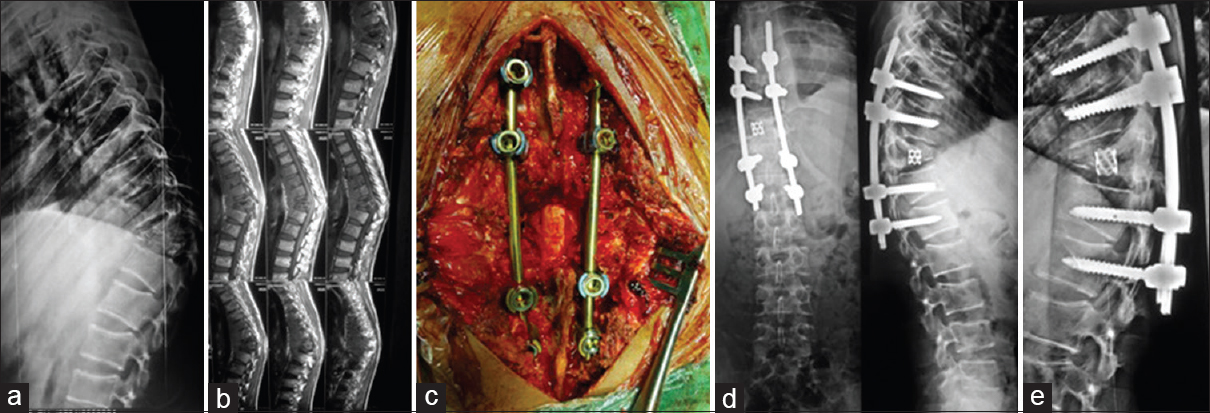
- (a) A 16-year-old male patient, D-10 D-11 tuberculosis. (b) Sagittal section of magnetic resonance imaging. (c) Debridement, decompression, and pedicle screw fixation two levels proximal and distal with cage and bone graft done. (d) Postoperative X-ray. (e) Postoperative X-ray follow-up X-ray at 12 months
Discussion
Chemotherapy is the mainstay in controlling and treating the disease in Pott's spine. Surgical management is an effective choice in the management as it can decrease the disease load thereby making the chemotherapy more effective, relive pain, improve neurological function, and reconstruct the spine stability. The purpose of any surgical procedure is to obtain adequate decompression and visualization for intervention and achieve spinal stability.
TB of spine almost always affects the anterior column of the spine, and hence, anterior approach is considered the gold standard for debridement and decompression in Pott's spine, which was popularized by Hodgson.[6] However, anterior exposure of the abdominal vessels and ureter presents a significant challenge to the surgeon, especially if the vertebral destruction due to disease has led to severe kyphosis. In addition, this approach is contraindicated in patients with concomitant pulmonary TB and compromised pulmonary reserve.[7] There may also be associated lung scarring secondary to old/active pulmonary TB, which may preclude the anterior approach. The posterior approach gives a reasonable access to the lateral and anterior aspects of the cord for an equally good decompression of the cord and thus characterized as simple approach. Combined anterior and posterior approach in one or two stages has been advocated by some researchers, but it is more invasive and has more complications and patient morbidity. Wang et al.[10] in their study compared combined approach with posterior-only approach and concluded that combined approach may not be ideal approach for treating thoracolumbar TB.
Oga et al. evaluated the adherence capacity of Mycobacterium tuberculosis to stainless steel and concluded that adherence was negligible and the use of implants in regions with active TB infection may be safe.[11] In addition, Shen et al. in their study concluded that the presence of the titanium cage anteriorly at the site of tubercular spondylitis has no negative influence on the course of infection healing, and additionally, they stabilize the affected segment maintaining sufficient sagittal profile.[12]
The advent of pedicle screw instrumentation and the development of the extended posterior approaches have allowed the surgeon to perform anterior debridement and reconstruction from behind, and have led many surgeons to opt for posterior only surgery. It further avoids the possible hazards of violating the thoracic or abdominal cavities.[13] Spinal TB is associated with osteopenia or soft vertebral bodies. Posterior instrumentation in these cases is justified by the fact that posterior elements are relatively healthier when compared to the vertebral body.[14]
Lumbar TB usually causes a severe kyphotic deformity which directly correlates with the severity of back pain.[15] While anterior instrumentation may prevent the progression of kyphosis during treatment; it is not so effective in correcting preexisting kyphosis. The addition of posterior instrumentation has shown to improve the correction of sagittal alignment. Transpedicular screw fixation provides sufficient stability, helps in correcting preexisting kyphosis effectively, and obviates the progress of late angular deformity.[16-18]
Ma et al.[19] reported that excellent neurological result was observed after single-stage posterior debridement, bone graft, and internal fixation in patients with neurological impairment due to spinal TB, which was similar to those obtained through anterior decompression. Moreover, the posterior approach may be superior to the anterior instrumentation to correct deformity and maintain that correction. Zhang et al.[20] Reported one stage posterior debridement and instrumentation for treating spinal TB where kyphotic angle was significantly corrected after surgery, and there were no relapses during long-term follow-up. Sahoo et al.[21] reported 18 selected cases of thoracolumbar spinal TB treated by posterior only approach surgery; kyphosis was improved from 17.7° ± 5.8° preoperatively to 9.4° ± 4.6° postoperatively. Xu et al.[22] in their study observed average Cobb angle correction to 5.3° ± 3.0° postoperatively from 22.1° ± 6.1° preoperatively. Meanwhile, average 1.8° ± 1.0° loss was observed at last visit. Zaveri and Mehta 2009[23] first reported on 15 cases of lumbar TB by transforaminal lumbar interbody fusion procedure and posterior fixation and received good clinical outcomes.
In our study, most of the patients had improved VAS scores, neurological deficit (Frankel scores) significantly improved at the final follow-up visit than those before surgery, there was no significant loss of kyphosis at final follow-up, and majority of the patients had achieved significant improvement in their daily activities except in two cases which could not regain any functional strength.
Thus, though anterior approach is a favored method for debridement and decompression as the lesion is situated anteriorly, there is an increased morbidity related to the approach (transthoracic, transpleural). The posterior only approach (extra-pleural) provides reasonable exposure for adequate debridement and decompression along with posterior instrumentation. Better sagittal spinal correction, lesser complications, insignificant loss of kyphosis, and less patient morbidity with good neurological recovery and disease control are the points in favor of posterior only approach.
Conclusions
From our study, we conclude that single-stage posterior-only debridement and transpedicular screw fixation is a safe and effective procedure and can play a significant role in the management of thoracic and lumbar spinal TB.
With this method, we can achieve adequate debridement, correction of kyphosis angle, and neurological recovery with relatively less postoperative complications and patient morbidity.
However, there are still some limitations of the study which include the authors' experience, insufficient sample of size and shorter duration of follow-up.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- TB/HIV Facts. 2011. Available from: http://www.who.int/tb/challenges/hiv/factsheet hivtb 2011.pdf (accessed )
- [Google Scholar]
- 2010/2011 Tuberculosis Global Facts. Available from: http://www.who.int/tb/publications/2010/factsheet_tb_2010.pdf (accessed )
- [Google Scholar]
- Severe kyphotic deformity in tuberculosis of the spine. Int Orthop. 1995;19:327-31.
- [CrossRef] [Google Scholar]
- Operative treatment of progressive deformity in spinal tuberculosis. Int Orthop. 2001;25:322-5.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior instrumentation in tuberculous spondylitis: Is it effective and safe? Clin Orthop Relat Res. 2007;460:108-16.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior spinal fusion. The operative approach and pathological findings in 412 patients with Pott's disease of the spine. Br J Surg. 1960;48:172-8.
- [CrossRef] [PubMed] [Google Scholar]
- Simultaneous anterior decompression and posterior instrumentation of the tuberculous spine using an anterolateral extrapleural approach. J Bone Joint Surg Br. 2008;90:1477-81.
- [CrossRef] [PubMed] [Google Scholar]
- Sagittal alignment after anterior debridement and fusion with or without additional posterior instrumentation in the treatment of pyogenic and tuberculous spondylodiscitis. Spine (Phila Pa 1976). 2003;28:1036-42.
- [CrossRef] [PubMed] [Google Scholar]
- Tuberculous kyphosis: Correction with spinal osteotomy, halo-pelvic distraction, and anterior and posterior fusion. J Bone Joint Surg Am. 1974;56:1419-34.
- [CrossRef] [Google Scholar]
- One-stage anterior debridement, bone grafting and posterior instrumentation vs. single posterior debridement, bone grafting, and instrumentation for the treatment of thoracic and lumbar spinal tuberculosis. Eur Spine J. 2014;23:830-7.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the risk of instrumentation as a foreign body in spinal tuberculosis. Clinical and biologic study. Spine (Phila Pa 1976). 1993;18:1890-4.
- [CrossRef] [PubMed] [Google Scholar]
- The role of single-stage posterior debridement, interbody fusion with titanium mesh cages and short-segment instrumentation in thoracic and lumbar spinal tuberculosis. J Neurosurg Sci. 2015;8(9):11051-59.
- [Google Scholar]
- Kyphotic deformity in spinal tuberculosis and its management. Int Orthop. 2012;36:359-65.
- [CrossRef] [PubMed] [Google Scholar]
- Historical aspects of Pott's disease (spinal tuberculosis) management. Eur Spine J. 2013;22(Suppl 4):529-38.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation of radiographic parameters and clinical symptoms in adult scoliosis. Spine (Phila Pa 1976). 2005;30:682-8.
- [CrossRef] [PubMed] [Google Scholar]
- Combined posterior instrumentation and anterior interbody fusion for active tuberculous kyphosis of the thoraco-lumbar spine. Curr Orthop. 1991;5:177-9.
- [CrossRef] [Google Scholar]
- A single stage posterior approach and rigid fixation for preventing kyphosis in the treatment of spinal tuberculosis. Spine (Phila Pa 1976). 1994;19:1039-43.
- [CrossRef] [PubMed] [Google Scholar]
- Role of posterior stabilisation in the management of tuberculosis of the dorsal and lumbar spine. J Bone Joint Surg Br. 2003;85:100-6.
- [CrossRef] [PubMed] [Google Scholar]
- Outcomes of anterior and posterior instrumentation under different surgical procedures for treating thoracic and lumbar spinal tuberculosis in adults. Int Orthop. 2012;36:299-305.
- [CrossRef] [PubMed] [Google Scholar]
- One-stage posterior debridement, transforaminal lumbar interbody fusion and instrumentation in treatment of lumbar spinal tuberculosis: A retrospective case series. Arch Orthop Trauma Surg. 2013;133:333-41.
- [CrossRef] [PubMed] [Google Scholar]
- Posterior-only approach surgery for fixation and decompression of thoracolumbar spinal tuberculosis: A retrospective study. J Spinal Disord Tech. 2012;25:E217-23.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical treatment for mono-segmental lumbar tuberculosis by single-stage posterior debridement, compact bone grafting and posterior single-segment fixation. Injury. 2015;46:1311-6.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical treatment of lumbar tuberculous spondylodiscitis by transforaminal lumbar interbody fusion (TLIF) and posterior instrumentation. J Spinal Disord Tech. 2009;22:257-62.
- [CrossRef] [PubMed] [Google Scholar]




