
Translate this page into:
Proposed maximum surgical blood ordering schedule for common orthopedic surgeries in a Tertiary Health - Care Center in Northern India
Address for correspondence: Dr. Sonam Kumari, H. No. 120, Sector 20 A, Chandigarh - 160 020, India. E-mail: sonu4068@yahoo.co.in
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Kumari S, Kansay RK, Kumar S. Proposed maximum surgical blood ordering schedule for common orthopedic surgeries in a Tertiary Health - Care Center in Northern India. J Orthop Allied Sci 2017;5:21-6.
Abstract
BACKGROUND:
Blood transfusion is the cornerstone of therapy for many serious ailments, surgical and trauma patients. Patients undergoing orthopedic surgeries as elective procedure or emergency orthopedic surgery for trauma often experience excessive blood loss- requiring transfusions. However, preoperative placement of blood requests frequently overshoots the actual need resulting in unnecessary crossmatching, which can be reduced by formulating maximum surgical blood ordering schedule (MSBOS). It is a table of elective surgical procedures, which lists the number of units of blood routinely cross-matched pre-operatively.
OBJECTIVE:
The objective of this study is to audit the blood utilization in orthopedic surgeries so that unnecessary cross-matching, wastage of blood bank resources, and financial losses to the patients could be reduced.
MATERIALS AND METHODS:
A retrospective study was carried out in our tertiary care hospital over a period of 6 months to determine the utilization of blood during different orthopedic procedures and to recommend an appropriate blood ordering schedule. The data collected include patient's requests, patient's transfused, type of surgical procedure, number of units crossmatched and transfused, crossmatch to transfusion ratio (CTR) and transfusion indices (TI's); according to them, MSBOS was proposed.
RESULTS:
A total of 478 units of blood were crossmatched for 273 patients and only 243 units were transfused to 183 patients. About 50.8% of the crossmatched units and 67% of the total patients were transfused. Seven out of the thirteen procedures had a CTR higher than 2, low TI ≤0.5 and blood utilization ≤50%. Fracture forearm and unilateral total knee replacement have the transfusion probability of ≤30%, so implementation of type and screen policy was recommended for these two procedures.
CONCLUSIONS:
MSBOS based on the past blood utilization records for different surgeries and keeping patients variables in consideration wherever required would provide an efficient way of blood utilization and appropriate management of blood bank resources.
Keywords
Blood requests
crossmatch
polytrauma
type and screen policy

Introduction
Patients undergoing orthopedic surgeries as an elective procedure or emergency orthopedic surgery for trauma often experience excessive blood loss- requiring transfusions. Orthopedic surgeries alone consume a considerable proportion of blood available to the National Health Services, which has been reported to be in the range of 10% - 15%.[1] However, it has been observed that the preoperative placement of blood requests frequently overshoots the actual need resulting in unnecessary crossmatching.[2] The consequences of unnecessary crossmatching results in outdating of blood, overburdening of blood bank personnel, depletion of blood bank resources, wastage of time and financial loss to the patients.[3,4]
The cross-match to transfusion ratio (CTR), the transfusion index (TI), transfusion probability and blood utilization when considered together are simple and reliable indicators of the accuracy of preoperative assessment of expected transfusions for an individual patient undergoing a particular surgical procedure. These TI's are helpful in formulating the maximum surgical blood ordering schedule (MSBOS). MSBOS is a table of elective surgical procedures, which lists the number of units of blood routinely cross-matched pre-operatively. Another term, surgical blood ordering equation which is an extended MSBOS incorporates patient and surgical variables, such as pre and post- operative hemoglobin levels of the patient and the amount of surgical blood loss during each surgical procedure.[5] They are intended only as a guide to the ordering of blood and blood products and are interpreted according to individual circumstances, including the clinical condition of the patients.[6]
The ratio of the number of units crossmatched to the number of units actually transfused, i.e., CTR should not exceed 2:1.[7] Lower CTR also reduces the overall consumption of blood bank resources, workforce and time. To limit the number of units held out of the circulation and outdating of blood units, MSBOS recommends that for patients likely to be transfused during surgery, the number of cross-matched units should be twice the median requirement for that surgical procedure.[8]
According to the International Red Cross, appropriate use of blood had cut down the number of transfusions by 30%.[9] Implementation of MSBOS by Chawla et al. resulted in about 60% reduction of cost to the patients.[4] Similarly, Hardy et al. found 33% reduction in the number of blood units crossmatched for an elective surgical procedures after introducing MSBOS at their hospital.[10] Keeping in view the previous literature, this study was initiated to improve the efficacy of ordering and utilization of blood by the formulation of MSBOS for common orthopedic procedures. Our primary objective was to audit the blood utilization in orthopedic surgeries both elective and emergency trauma so that unnecessary crossmatching, wastage of blood bank resources, and financial losses to the patients could be reduced.
Materials and Methods
A retrospective analysis of data for 6 months from September 2014 to February 2015 was performed. Required data of patients who underwent orthopedic surgeries were collected from blood bank records (from patient request forms, crossmatching forms and blood issuance register). Revision total hip replacement (THR), revision total knee replacement (TKR), pelvic fractures, bone tumor surgeries, bilateral primary joint replacement, polytrauma (multiple bone fractures) and fracture shaft femur are the various causes for massive transfusion in orthopedics. Patients who underwent massive transfusion were excluded from the study to eliminate bias. In this study, the patients who had only multiple bone fractures were included as polytrauma; although polytrauma patients also have major abdominal and chest injuries, but those patients were excluded from the study as it exclusively involved orthopedic procedures. The total number of patient's requests, number of patient's transfused, number of units crossmatched, and number of units transfused were calculated for each surgical procedure.
The CTR, transfusion probability (%T) and TI were calculated as:
-
The formula for CTR:

CTR is used as a measure of the efficiency of blood ordering practice. A ratio of more than 2.5 indicates excessive crossmatching of blood for a specific procedure even a ratio of ≥2 is considered indicative of significant blood wastage. A realistic objective for CTR is 1 - 2:1.
-
The formula for transfusion probability:
A value of ≤30 was considered indicative of significant blood wastage.
-
The formula for TI:
The TI is defined as the average number of units transfused for a given procedure. TI of more than 0.5 indicates that blood needs to be cross-matched preoperatively for that procedure while a value of ≤0.5 signifies no need for crossmatch.
-
Blood ordering quotient (BOQ) represents a ratio between the average number of units cross-matched per patient for a particular procedure and the average number of units transfused per patient. It is calculated as follows:

Where
 BOQ of <1.5 indicates significant usage of blood for that procedure.
BOQ of <1.5 indicates significant usage of blood for that procedure. MSBOS = 1.5 × TI where

MSBOS was formulated using Mead's criterion. According to this criterion, the number of red blood cells (RBCs) calculated was one and half times the TI for each surgical procedure. Keeping in view, the MSBOS calculated using Mead's criteria, TIs and the clinical experience, MSBOS is recommended for each surgical procedure.
Results
Thirteen common orthopedic surgeries carried out at our teaching hospital were evaluated. For 273 patients, 478 units of blood were crossmatched and only 243 units were transfused to 183 patients [Table 1], that is, 50.8% of the crossmatched units and 67% of the total patients were transfused.
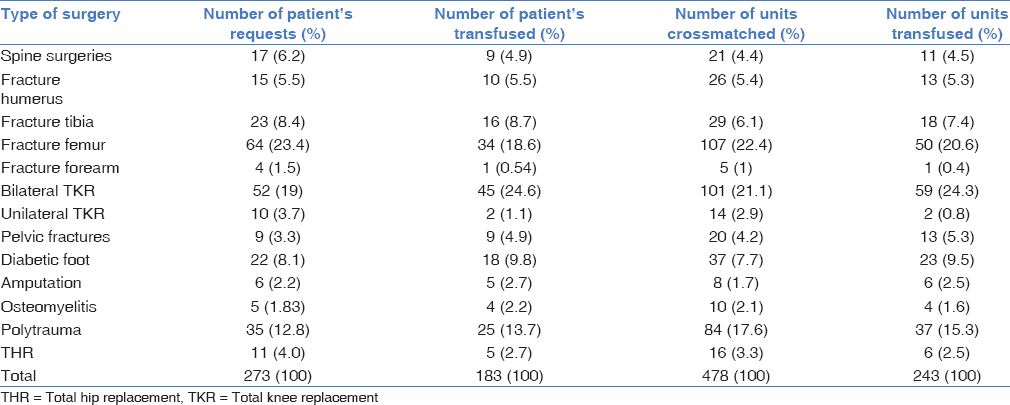
Maximum number of patient requests were received for fracture femur, i.e., 64 (23.4%) followed by bilateral TKR, i.e., 52 (19%). Furthermore, maximum number of blood units were transfused to patients for these two procedures, i.e., 50 (20.6%) and 59 (24.3%), respectively. Fracture femur was the most common procedure, followed by bilateral TKR but maximum number of patients transfused (45) and maximum number of blood units transfused (59) were for bilateral TKR. Blood crossmatch and transfusion patterns for the 13 orthopedic surgeries were shown in Table 1.
The CTR, transfusion probability (%T), as well as TI 1 and TI 2, were formulated for each of the elective procedures and is shown in Table 2.
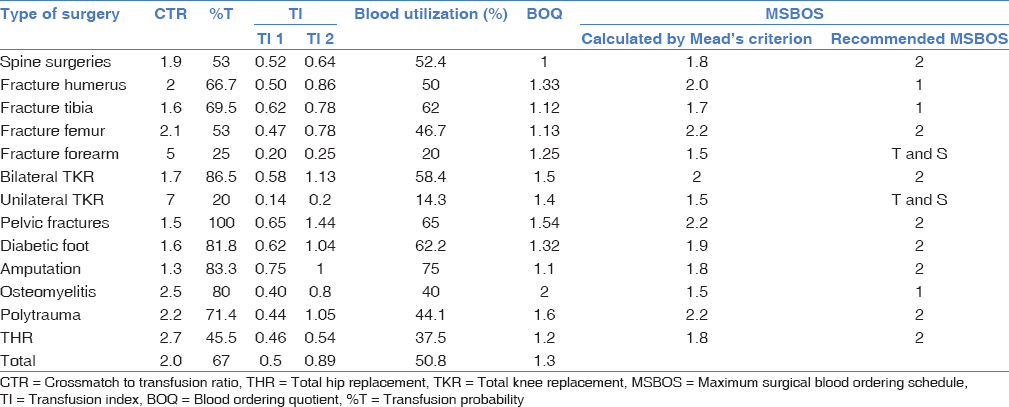
The CTR was ≥2, TI 1 ≤0.5, and blood utilization was ≤50% for seven procedures, i.e., fracture humerus, fracture femur, fracture forearm, unilateral TKR, osteomyelitis, polytrauma, and THR indicating excessive crossmatching of blood for these procedures. Although fracture femur was at number two orthopedic procedure for which maximum number of blood units were transfused, blood utilization for it was <50% (46.7%) indicating excessive crossmatching. The CTR for spine surgeries, fracture tibia, bilateral TKR, pelvic fractures, diabetic foot, and amputation was <2 which was within the MSBOS criteria. Transfusion probability was <30% for fracture forearm (25%) and unilateral TKR (20%) indicating insignificant blood usage for these two procedures. BOQ was higher, i.e., >1.5 for bilateral TKR, pelvic fractures, osteomyelitis, and polytrauma indicating excessive blood ordering for these procedures. MSBOS was calculated using Mead's criteria for all the thirteen procedures and MSBOS for our hospital was recommended keeping in view the TIs and clinical experience of orthopedicians. Type and screen policy (and ensuring the availability of group specific blood) was recommended for fracture forearm and unilateral TKR.
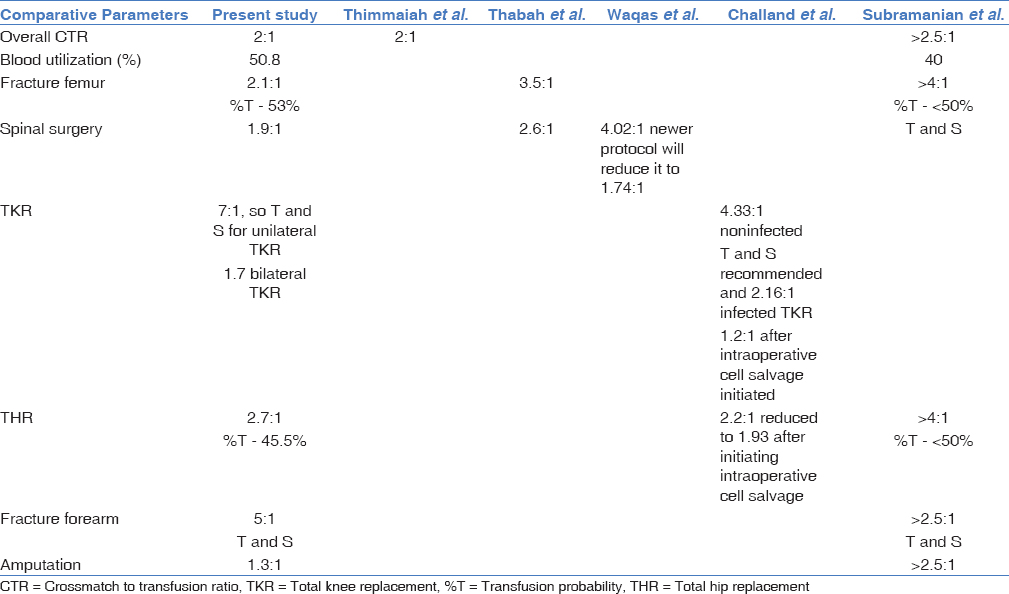
Table 3 shows the comparison of the results of the present study with other studies from the literature.
Discussion
Although the risk of transfusion transmitted infections is declining, zero risk could not be achieved; moreover, the non-infectious serious hazards of transfusion (immune as well as nonimmune) significantly contributes to the morbidity and mortality associated with transfusion which can rarely be fatal. Provision of adequate and safe blood is challenging in developing countries due to the paucity of voluntary blood donors, poor facilities for storage and blood component preparation as well as inappropriate blood ordering and utilization.[11] Limited availability and supply of blood and the associated risks of transfusion necessitates the rational use of blood and avoidance of unnecessary transfusions.[6] Chawla et al. in their study found that both the public and private hospitals were not rational in the use of blood. In the public
Hospitals, appropriate use of blood was only 54.1% (n = 92) compared to the private hospitals where appropriateness was 69.4%.[4] Even in developed countries, inappropriate transfusion is in the range of 18% - 35%, while in India the range varied from 30% to 60%.[12]
One of the best methods of evaluating transfusion practices is to determine the ratio of units crossmatched to units transfused (CTR). The more accurately the clinicians predict patient's blood needs, the closer the CTR will approach 1:1. A CTR ≥2.5, %T ≥50 and TI ≥0.5 are considered indicative of significant blood utilization.[3,7]
In the present study, overall CTR was 2:1 which was same as CTR of Thimmaiah et al., although this was within the recommended guidelines, efforts should be made to reduce it to 1:1.[1]
In the study by Thabah et al., for orthopedic cases, surgeries for fracture femur was the most common procedure followed by spinal surgeries and the CTR was 3.5 and 2.6 respectively, and it was ≤2 for other surgeries.[6] Similarly, in the present study, surgery for fracture femur was the most common procedure with CTR of 2.1 which was quite lower than that of Thabah et al.
CTR for spine surgeries was 1.9 in the present study while in the study of Waqas et al., CTR for spine surgeries was very high, i.e., 4.02 which could be reduced significantly to 1.74 by implementing their new transfusion protocol, considering factors such as age, gender, preoperative hemoglobin and number of spine levels decompressed and fused.[13]
According to Challand et al., cross - matching was necessary for both non - infected and infected revision THR, but the number of units requested could be reduced to 2 units, which was same as the recommended MSBOS for THR in the present study. In revision TKR, transfusions were more likely in infected cases and a “group and save” may be sufficient for noninfected cases same type and screen policy was recommended in the present study for unilateral TKR but not for bilateral TKR. In the present study, CTR for THR (including both infected, non – infected and revision THR) was 2.7 and TI was 0.46 while in Challand et al. study, for revisions of noninfected THR, the CTR = 2.24 and TI = 1.67; in infected cases, CTR = 2.16 and TI = 1.68. In revisions of non-infected TKR, the CTR = 4.33 and TI = 0.48 and in infected cases, the CTR = 2.16 and TI = 1.35. They observed the considerable change in the practice of ordering crossmatched blood following the introduction of intraoperative cell salvage devices (revision THR: CTR = 1.93, TI = 0.84; revision TKR: CTR = 1.20, TI = 0.16).[14] From results of Challand et al., it could be considered that intraoperative cell salvage is a very good option to reduce the overall usage of blood.
Thimmaiah et al. conducted their study on 449 patients, 14.5% of them underwent blood transfusion. Requirements of blood transfusion were 5% in both primary and revision TKR, 38% in primary and revision THR and revision THR alone 74.7% of patients.[1] In the present study, transfusions were required in 45.5% of THR, 86.5% of bilateral TKR and 20% of unilateral TKR, transfusion requirements were little higher in replacement surgeries in the present study than study by Thimmaiah et al. but their CTR was same (2:1) as the present study.
In a study of Subramanian et al., 6 of the 12 elective procedures had a high CTR ≥2.5 with 2 of them, namely, intertrochanteric fracture femur and THR, exceeding 4. However, the probability that a patient would undergo transfusion (%T) was <50% in these procedures while in the present study CTR and transfusion probability was 2.1 and 53% for fracture femur and 2.7 and 45.5% for THR, respectively. Fracture spine and fracture forearm indicates insignificant blood utilization in Subramanian et al. study. The present study also indicated insignificant blood utilization in forearm surgeries (25%) but not for spine surgeries (53%).[2]
The patient's preoperative condition affects the CTR because MSBOS algorithm uses the surgical procedures alone.[8] Elderly patients with comorbid conditions and inoperable diseases; in such cases, it is best to crossmatch blood units only after the surgeon had decided to proceed further.[3] Blood wastage also depends on the surgeons' expertise (resulting in more or less blood loss) for a particular surgery and the anesthesiologists decision (their preset higher transfusion triggers). Despite much studies and evidence - based guidelines for transfusion, inappropriate transfusion still happens. In drawing up the “schedule,” attention must be paid to factors that would affect the speed of provision of compatible blood such as, the distance of the operating rooms from the blood bank and emphasis should be laid on local circumstances, clinical practice and patient's variables.[6] Nuttall et al. determined the predictors of red blood cell transfusion in total hip arthroplasty and developed a theoretically more efficient system which incorporated patient factors in the ordering of RBC's for surgical patients.[15] Low preoperative hemoglobin/hematocrit, short stature, female sex, availability of preoperative autologous blood donation, surgical blood loss, and the type of surgery are the risk factors useful in predicting the blood transfusion.[5]
Transfusion request for each patient should be based on clinical judgment of the patient and appropriate hemodynamic monitoring. The risk of transfusion reactions, infections and metabolic complications associated with massive transfusion should curtail the indiscriminate or routine prophylactic use of allogeneic blood products. Numerous methods have been suggested and used earlier to reduce the use of blood in elective major surgeries such as THR and TKR. These include the intraoperative and perioperative cell salvage, antifibrinolytic agents, treatment of anemia, reviewing antiplatelet drugs and anticoagulation; appropriate use of these would help in reducing the transfusion rate and would reduce the wastage of blood bank resources.[2] However, none of these options were considered in the present study due to the lack of facilities, financial constraints and availability of sufficient blood-stock; moreover most of the orthopedic procedures were emergency procedures and considering options such as preoperative use of erythropoietin and iron therapy were not feasible.
Conclusions
MSBOS implementation helps in logical and appropriate use of blood bank resources by avoiding the unnecessary crossmatching for surgeries where preoperative blood requirement is minimal but the availability of adequate blood supply should be ensured before surgery. Regular auditing to ensure the appropriateness and efficacy of MSBOS and periodic feedbacks are essential to improve the blood utilization practices and patient care. It would have not only an impact in blood bank management but also a change in attitude and practice of surgeons for better.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Blood transfusion in hip and knee joint replacement surgery. Int J Orthop Surg. 2009;17(1)
- [CrossRef] [Google Scholar]
- Reviewing the blood ordering schedule for elective orthopedic surgeries at a level one trauma care center. J Emerg Trauma Shock. 2010;3:225-30.
- [CrossRef] [PubMed] [Google Scholar]
- Blood utilisation in elective general surgery cases: Requirements, ordering and transfusion practices. J Postgrad Med. 2000;46:13-7.
- [Google Scholar]
- An audit of blood cross-match ordering practices at the Aga Khan University Hospital:First step towards a maximum surgical blood ordering schedule. J Pak Med Assoc. 2001;51:251-4.
- [Google Scholar]
- An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am. 1999;81:2-10.
- [CrossRef] [PubMed] [Google Scholar]
- 'Maximum surgical blood order schedule' in a newly set-up tertiary care hospital. Anaesth Pain Intensive Care. 2013;17:28-32.
- [Google Scholar]
- Guidelines for implementation of a maximum surgical blood order schedule. The British Committee for Standards in Haematology Blood Transfusion Task Force. Clin Lab Haematol. 1990;12:321-7.
- [Google Scholar]
- Reducing unnecessary cross-matching: A patient-specific blood ordering system is more accurate in predicting who will receive a blood transfusion than the maximum blood ordering system. Anesth Analg. 2003;96:369-75.
- [CrossRef] [Google Scholar]
- South East Asia faces severe shortage of safe blood. BMJ. 2000;320:1026..
- [CrossRef] [PubMed] [Google Scholar]
- Maximum surgical blood order schedule reduces hospital costs. Am Surg. 1987;53:223-5.
- [Google Scholar]
- Pattern of blood transfusion request and utilization at a Nigerian University Teaching Hospital. Sahel Med J. 2014;17:19-22.
- [CrossRef] [Google Scholar]
- Regional Appropriateness of Blood Transfusion Audit, The Northern Ireland Regional Transfusion Committee. Summary Report 2004:1-30.
- [Google Scholar]
- Prospective validation of a blood ordering protocol for elective spine arthrodesis and its impact on cost reduction. Surg Neurol Int. 2014;5(Suppl 7):S362-4.
- [CrossRef] [PubMed] [Google Scholar]
- Maximum surgical blood ordering schedule for revision hip and knee arthroplasty. J Bone Joint Surg Br. 2011;93:527-32.
- [Google Scholar]
- Use of the surgical blood order equation in spinal instrumentation and fusion surgery. Spine (Phila Pa 1976). 2000;25:602-5.
- [CrossRef] [PubMed] [Google Scholar]




