
Translate this page into:
Prevalence of concomitant injuries with Hill–Sachs lesion in traumatic shoulder dislocations
Address for correspondence: Dr. Reddy Ravikanth, Department of Radiology, St. John's Medical College, Bengaluru - 560 034, Karnataka, India. E-mail: ravikanthreddy06@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Ravikanth R, David M, Sandeep S, Abraham MJ, Sarkar P, Alapati A, et al. Prevalence of concomitant injuries with Hill–Sachs lesion in traumatic shoulder dislocations. J Orthop Allied Sci 2017;5:58-62.
Abstract
INTRODUCTION:
The shoulder joint (comprising the glenohumeral and scapulothoracic joints) displays the greatest range of motion of all joints in the human body, and preservation of its stability is essential to its function. The Hill–Sachs defect is a compression fracture of the humeral head associated with instability. The Hill–Sachs lesion may be limited to the articular cartilage or may extend to the subchondral bone.
PURPOSE:
To identify and characterize the magnetic resonance imaging (MRI) findings in patients with Hill–Sachs lesion and to look for concomitant injuries.
MATERIALS AND METHODS:
This retrospective case series included 35 patients identified by search through the senior authors' databases, with cross-reference to our institutional radiologic communication system for MRI review. Baseline patient demographic data were collected, including age and sex. We retrospectively assessed all patients who were diagnosed with shoulder dislocation at our institution between 2012 and 2016.
RESULTS:
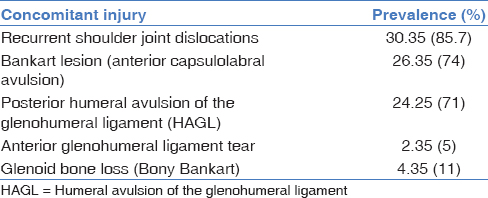
We identified 35 patients with a posterior Hill–Sachs lesion. The average age was 33.6 years (range, 22–70 years) and 31 patients were male (89%). There were 18 right shoulders and 17 left shoulders. Eleven patients (31.4%) had evidence of engaging Hill–Sachs lesion and 24 did not. Posterior humeral avulsion of the glenohumeral ligament (HAGL) injuries were found to be partial tears (30%) and complete tears (70%). Additional shoulder injury with the lesion occurred in 96% of identified cases. The most common concomitant injuries were recurrent shoulder joint dislocations (85.7%), posterior HAGL (71%), anterior Bankart lesions (74%), glenoid bone loss (11%), and anterior glenohumeral ligament injuries (5%).
CONCLUSION:
Engaging Hill–Sachs lesion on physical examination shows a trend toward more medially oriented lesion measured using modified biceps angle on MRI, and the size of engaging Hill–Sachs lesion appears significantly larger than that of nonengaging lesions on both axial and coronal images.
Keywords
Engaging lesions
Hill–Sachs
joint instability/complications
modified biceps angle
magnetic resonance imaging
shoulder dislocations/complications
trauma

Introduction
The shoulder joint (comprising the glenohumeral and scapulothoracic joints) displays the greatest range of motion of all joints in the human body, and preservation of its stability is essential to its function. The glenohumeral joint is an inherently unstable ball-and-socket joint, and it is susceptible to a variety of injuries, especially dislocation. The term shoulder instability refers to a variety of mechanisms and clinical presentations including symptomatic and asymptomatic laxity, subluxation, and dislocation.[1] Acute and chronic anterior shoulder instability is accompanied by secondary injuries of the humeral head, articular cartilage, anterior and posterior capsule, glenohumeral ligaments, and glenoid and biceps tendon. Significant injuries occur during the initial shoulder dislocation event, and additional soft tissue, cartilage, and bony injury may occur with every subsequent dislocation episode. The severity of associated injuries may increase with time as a result of repeated dislocation or subluxation episodes. The severity of labrum lesions in posttraumatic shoulder instability increases with time. Associated injuries may influence long-term outcome. The goal of all reconstructive procedures in the unstable shoulder is to reduce the amount of pathologic translation and avoid secondary morbidity to intra- and extra-articular structures.[2]
The incidence of Hill–Sachs lesion is generally higher than previously thought. This lesion occurs on the articular surface posterior to the humeral greater tuberosity and must be distinguished from the denuded articular cartilage, the nonarticulating bare area of the humeral head. The Hill–Sachs lesion may be limited to the articular cartilage or may extend to the subchondral bone.
The Hill–Sachs defect is a compression fracture of the humeral head associated with instability. At the time of shoulder dislocation, the soft cancellous bone of the humeral head is impressed against the hard cortical bone of the anterior glenoid rim, creating a compression fracture in the humeral head. This can be visualized on an internal rotation radiograph of the shoulder, as first described by Hill and Sachs in 1940.[3] The incidence of the defect approaches 100% in patients with recurrent anterior shoulder instability. Larger lesions with advanced bone loss are more likely to engage, resulting in shoulder instability at lower arm abduction angles. In patients with moderate bone loss, arthroscopic management of the defects includes transfer of the infraspinatus and posterior capsule into the defect, known as the remplissage procedure. Bone grafting of the defect with allograft humeral or femoral head replacement. is done for larger lesions with severe bone loss. The true incidence of Hill–Sachs lesions is unknown. While reported to occur in 40%–90% of patients with an initial dislocation event, the incidence may be as high as 100% with recurrent instability.[4] The size of the defect is often related to the amount of time the shoulder remains dislocated, thus quite small with the first dislocation. With each subsequent dislocation, the compression fracture enlarges, becoming more evident on follow-up radiographs.
A growing body of evidence in the orthopedic literature supports the notion that recurrent instability of the shoulder leads to progressive bone loss, both on the glenoid and the humeral head. Bone loss on either side of the joint may lead to recurrent instability at lower arm abduction angles, as well as feelings of instability with activities of daily living. Shoulder dislocations can occur with less force, such as while sleeping at night or with the arm adducted at the side. A substantial amount of literature describes the well-established relationship between anterior glenoid bone loss and recurrent instability. However, there are little published data on management of bone defects on the humeral side. Reverse Hill–Sachs lesions are located on the anterior-superior humeral head, and they are associated with posterior shoulder dislocations. The incidence of this type of lesion is difficult to quantify, as posterior dislocations are much less common, although the reverse lesion may occur in up to 86% of posterior instability cases.[5]
Purpose
To identify and characterize the magnetic resonance imaging (MRI) findings in patients with Hill–Sachs lesion and to look for concomitant injuries.
Materials and Methods
This retrospective case series included 35 patients identified by search through the senior authors' databases, with cross-reference to our institutional radiologic communication system for MRI review. Baseline patient demographic data were collected, including age and sex. We retrospectively assessed all patients who were diagnosed with shoulder dislocation at our institution between 2012 and 2016. Inclusion criteria were anterior shoulder dislocation, availability of preoperative MRI, the absence of acute or former concomitant injuries to the investigated shoulder joint, and no previous shoulder surgery. All demographic data and injury mechanisms were drawn from patients' charts and the hospital's electronic database. First, traumatic and recurrent shoulder dislocations were reported. Radiographs and MR images were analyzed by radiologists and trauma surgeons in regard to Hill–Sachs lesions and the absence of concomitant injuries (i.e., fractures, rotator cuff injuries, superior labrum anteroposterior, and anterior labral periosteal sleeve avulsion). The MRI studies were conducted with coronal fast short-tau inversion recovery and coronal, sagittal, and axial fast spin-echo techniques. MRI was performed with a 1.5-T system and a 3-channel, receive-only, phased-array shoulder coil (GE Healthcare). The imaging protocol involved proton-density fast spin-echo sequences (repetition time/echo time [TR/TE], 4000–6000/28–38 ms) and inversion recovery sequences (TR/TE, 3200–6800/15–18 ms). A senior musculoskeletal radiologist assessed the identified patients' MRIs to confirm the presence of abnormalities.
Results
We identified 35 patients with a posterior Hill–Sachs lesion. The average age was 33.6 years (range, 22–70 years) and 31 patients were male (89%). There were 18 right shoulders and 17 left shoulders. Eleven patients (31.4%) had evidence of engaging Hill–Sachs lesion and 24 did not. Posterior humeral avulsion of the glenohumeral ligament (HAGL) injuries were found to be partial tears (30%) and complete tears (70%). Additional shoulder injury with the lesion occurred in 96% of identified cases. The most common concomitant injuries were recurrent shoulder joint dislocations (85.7%), posterior HAGL (71%), anterior Bankart lesions (74%), glenoid bone loss (11%), and anterior glenohumeral ligament injuries (5%) [Table 1].
We quantified Hill–Sachs lesions using MRI and measured the depth of the lesion but were not able to show a significant difference between stable and unstable shoulders that were treated nonoperatively. In cases of engaging lesions, the mean width was 48% and the mean depth was 16% of the humeral head diameter on axial images. The corresponding width and depth measurements on coronal images were 40% and 15%, respectively. In cases of nonengaging lesions, the corresponding width and depth measurements were 42% and 12% on axial images and 34% and 14% on coronal images, respectively. The size of engaging Hill–Sachs lesions was significantly larger than that of nonengaging lesions on both axial and coronal images. The location of the Hill–Sachs lesion was assessed using a modified biceps angle on MRI. As opposed to the biceps angle that used the biceps groove as a reference point for location of the Hill–Sachs lesion or an angle between the groove and the central aspect of the Hill–Sachs lesion to assess location, modified biceps angle on MRI accounted for the medial extent of the lesion because this portion would be the first portion to engage the anterior glenoid with the shoulder in abduction and external rotation (ABER).
Discussion
Hill–Sachs lesion results from impaction of the stronger anterior glenoid margin on the less compact posterosuperior margin of the humeral head. The location of the Hill–Sachs lesion depends on the degree of ABER of the humerus during injury: the more abducted and externally rotated the shoulder during the injury, the more superior and posterior is the position on the humeral head. The location, size, and orientation of the Hill–Sachs lesion have all been postulated to decrease stability of the glenohumeral joint. As the size of a Hill–Sachs lesion increases, less contact area becomes available for the humeral head to articulate with the glenoid during ABER.[6] The orientation of a Hill–Sachs lesion is thought to result in shoulder instability because of the risk of engagement when the shoulder is in the ABER position. Engagement is a descriptive term for abnormal contact between the humeral head and glenoid; it predisposes the shoulder to instability or the symptoms of instability. With the shoulder abducted and externally rotated, an intact posterosuperior humeral head maintains contact with the glenoid throughout the range of motion. If a Hill–Sachs lesion is present and parallel to the anterior margin of the glenoid in the ABER position, the defect loses contact with the glenoid and becomes lodged onto or engages the anterior margin of the glenoid. When the patient attempts internal rotation, the humeral head becomes stuck on the glenoid, predisposing the joint to instability.[7] Alternatively, when a Hill–Sachs lesion is oriented diagonally in relation to the anterior glenoid in the ABER position, continuous contact between the two articular surfaces during range of motion decreases the likelihood of engagement, instability, and signs of instability. The importance of the location of the Hill–Sachs lesion in predisposing to shoulder instability has been described in the form of the glenoid track theory. The glenoid track is the contact area between the humeral head and glenoid during ABER.[5]
Pathoanatomy
Hill–Sachs lesions most commonly occur during anterior glenohumeral instability episodes. The shoulder typically is in an abducted, externally rotated position. As the humeral head is forced anteriorly, the capsule, glenohumeral ligaments, and glenoid labrum are stretched and likely torn. As the humeral head translates farther anteriorly, a compression fracture occurs along the posterior-superior-lateral aspect of the humeral head as it comes into contact with the anterior glenoid rim. In cases of recurrent anterior shoulder instability, the static restraints to glenohumeral translation (capsuloligamentous structures and labrum) become increasingly attenuated. This makes it easier for the relatively softer cancellous bone of the humeral head to sustain continued damage as it makes repeated contact with the harder cortical bone of the anterior glenoid rim.[8]
Hill–Sachs lesions are typically described as engaging or nonengaging: an engaging Hill–Sachs lesion, as described by Palmer and Widen[9] and Burkhart and De Beer,[10] occurs when the humeral head defect engages the rim of the glenoid while the shoulder is in a position of athletic function, with 90° of abduction and 0°–135° external rotation. In an engaging lesion, the long axis of the humeral head defect is oriented parallel to the anterior glenoid rim and thus engages with it when the shoulder is in ABER. When the humeral defect is not parallel with the rim of the glenoid and thus does not engage with it in a position of function, the lesion is referred to as a nonengaging Hill–Sachs lesion. Hill–Sachs lesions rarely occur in isolation. They most commonly occur in conjunction with an anterior capsulolabral avulsion, the Bankart lesion.[11] Other common coexisting injuries include HAGL and mid capsular tears, floating anterior capsule, anterior glenohumeral ligamentous pathology, and glenoid bone loss (i.e., bony Bankart lesion).
History
The patient with a Hill–Sachs defect will uniformly have a history of shoulder instability, whether a single dislocation or recurrent instability events. It is important for the examiner to inquire about the initial dislocation event, the mechanism of injury, the position of the arm (i.e., ABER), the length of time the shoulder remained dislocated before reduction, whether the shoulder self-reduced or required reduction with sedation, the number of subsequent dislocations, the ease with which the shoulder dislocates and reduces, and the ease of shoulder dislocation, number of dislocation events, and arm position all provide information on the stability of the shoulder. Shoulders that dislocate easily with activities of daily living, and those that dislocate in lower arm abduction angles, are more likely to have bone loss, both on the anterior glenoid and humeral head.[12]
Clinical examination
Fullness in the anterior shoulder may represent an anterior dislocation, while an arm fixed in internal rotation may represent a locked posterior dislocation.[13] Both active and passive range of motion should be determined.[14] Apprehension and instability at lower arm abduction angles is indicative of severe glenohumeral instability and raises the suspicion of bone loss.[15] The jerk test and posterior load and shift test evaluate for posterior glenohumeral instability. Instability can further be confirmed clinically by the Jobe's apprehension and relocation tests.[16]
Diagnostic radiology
A number of diagnostic plain film, ultrasound, computed tomography (CT), and MRI techniques have been described for detecting pathology of the humeral head, osseous glenoid, and labrum. The radiographic techniques most advantageous for initial evaluation of glenohumeral instability are the anteroposterior projection AP with internal and external views, axillary, axillary with exaggerated external rotation, apical oblique (Garth view), and West Point views.[17] The combination of these views is an important first step at effectively evaluating both the glenohumeral relationship and osseous pathology on both the humerus and the glenoid. Ultrasound has been suggested as a cost-effective method for screening patients with shoulder instability for Hill–Sachs lesions. This has the advantages of allowing the patient to remain in a position of comfort and minimizing exposure to excessive radiation that accompanies CT and the multiple radiographs specific to detecting a possible Hill–Sachs lesion.[18] However, this practice remains to be validated for determining specific treatment. MRl is advantageous as it allows for detection of soft tissue pathology that may need to be addressed during surgical intervention and can certainly be a tool to help delineate the amount of humeral and glenoid bone loss. A double-blind, prospective study by Denti et al. on 15 patients yielded a sensitivity of 60%, specificity of 100%, and accuracy of 87% compared to arthroscopy, which had a sensitivity of 80%, specificity of 100%, and accuracy of 87%.[19] The gold standard for the evaluation of a Hill–Sachs defect remains a CT scan, with the humeral head digitally subtracted in order to critically quantify the location and size of the humeral defect.[20] In addition, the sagittal oblique view of the glenoid should be visualized in order to look at the amount of glenoid bone loss. The osseous deficits as visualized on CT scan can be precisely defined and are the most important findings for surgical decision making.[21]
Conclusion
In Hill–Sachs injury, a high degree of suspicion should be observed for recurrent shoulder dislocations, associated ligament injuries such as posterior HAGL, anterior Bankart lesions, glenoid bone loss (bony Bankart), and anterior glenohumeral ligament injuries. Engaging Hill–Sachs lesion on physical examination shows a trend toward more medially oriented lesion measured using modified biceps angle on MRI and the size of engaging Hill–Sachs lesion appears significantly larger than that of nonengaging lesions on both axial and coronal images.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Recurrent posterior shoulder instability. J Bone Joint Surg Am. 2005;87:883-92.
- [CrossRef] [PubMed] [Google Scholar]
- Natural history of glenohumeral dislocation – Revisited. Am J Sports Med. 1982;10:135-7.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of the spectrum of intra-articular lesions in acute and chronic anterior shoulder instability. Arthroscopy. 2007;23:985-90.
- [CrossRef] [PubMed] [Google Scholar]
- The incidence of Hill-Sachs lesions in initial anterior shoulder dislocations. Arthroscopy. 1989;5:254-7.
- [CrossRef] [PubMed] [Google Scholar]
- Structural and mechanical properties of the glenohumeral joint posterior capsule. J Shoulder Elbow Surg. 2005;14:201-6.
- [CrossRef] [PubMed] [Google Scholar]
- The pathophysiology of shoulder instability. Am J Sports Med. 2000;28:910-7.
- [CrossRef] [PubMed] [Google Scholar]
- The Hill-Sachs lesion. An experimental study. Am J Sports Med. 1980;8:328-32.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic management of posterior instability: Evolution of technique and results. Arthroscopy. 2008;24:389-96.
- [CrossRef] [PubMed] [Google Scholar]
- The bone block method for recurrent dislocation of the shoulder joint. J Bone Joint Surg. 1948;30B:53-8.
- [CrossRef] [Google Scholar]
- Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy. 2000;16:677-94.
- [CrossRef] [PubMed] [Google Scholar]
- Hill-sachs lesion and normal humeral groove: MR imaging features allowing their differentiation. Radiology. 1994;190:665-8.
- [CrossRef] [PubMed] [Google Scholar]
- Hill-sachs lesion: Comparison of detection with MR imaging, radiography, and arthroscopy. Radiology. 1992;185:847-52.
- [CrossRef] [PubMed] [Google Scholar]
- Intraarticular pathology in acute, first-time anterior shoulder dislocation: An arthroscopic study. Arthroscopy. 1993;9:546-9.
- [CrossRef] [PubMed] [Google Scholar]
- The relationship between Hill-Sachs lesion and recurrent anterior shoulder dislocation. Acta Orthop Belg. 2007;73:175-8.
- [Google Scholar]
- Management of anterior glenohumeral instability associated with large Hill-Sachs defects. Tech Shoulder Elbow Surg. 2004;5:170-5.
- [CrossRef] [Google Scholar]
- Radiologic features of shoulder instability. Clin Orthop Relat Res. 1993;291:29-44.
- [CrossRef] [Google Scholar]
- Classification and evaluation. In: Bigliani LU, ed. AAOS Monograph Series: The Unstable Shoulder. Rosemont, IL: American Academy of Orthopaedic Surgeons; 1996. p. :25-36.
- [Google Scholar]
- Clinical assessment of three common tests for traumatic anterior shoulder instability. J Bone Joint Surg Am. 2006;88:1467-74.
- [CrossRef] [PubMed] [Google Scholar]
- Magnetic resonance imaging versus arthroscopy for the investigation of the osteochondral humeral defect in anterior shoulder instability. A double-blind prospective study. Knee Surg Sports Traumatol Arthrosc. 1995;3:184-6.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis of Hill-Sachs lesion of the shoulder. Comparison between ultrasonography and arthro-CT. Acta Radiol. 1997;38:523-6.
- [CrossRef] [PubMed] [Google Scholar]
- Osteoarticular allograft transplantation for large humeral head defects in glenohumeral instability. Arthroscopy. 2007;23:322.e1-5.
- [CrossRef] [PubMed] [Google Scholar]




