
Translate this page into:
New emerging Gore Matrix: Basis of stitchless spine surgery under local anesthesia
Address for correspondence: Dr. Satishchandra Gore, 1128, Shivajinagar, Mission Spine, Pune - 411 016, Maharashtra, India. E-mail: yesgore@yahoo.co.in
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Gore S. New emerging Gore Matrix: Basis of stitchless spine surgery under local anesthesia. J Orthop Allied Sci 2017;5:1-5.
Introduction
Treatment of back pain, sciatica, and claudication has changed due to understanding of anatomy, physiology of pain generators leading to change in access, philosophy, and equipment. I have tried to summarize what was the traditional past, why change is necessary and what has changed, and how the change is incorporated in Gore matrix for diagnosis and gore system for treatment in back pain, sciatica, and claudication by proposing spine surgery as stitchless and under local anesthesia in awake and aware patients.
Why Change?
Uncertainty is unmeasurable risk and risk is measurable uncertainty [Figure 1].
- Uncertainty and risk
Due to pain being subjective impression of the patient and not correlated with images well, diagnosis and outcomes in lumbar degenerative spine surgery for treating pain have been uncertain. The patient is afraid in his/her mind about risks and the surgeon has uncertainty about outcomes. We need to reduce the risk and overcome the uncertainty. This is possible by an algorithmic approach and not trial and error in diagnosis and treatment plan.
Our new ability to pinpoint the “pain generators” has made surgery safe and precise and predictable. Only selected spots generate pain and claudication, so surgical corridor to treat those can be subcentimeter [Figure 2].[1] In case of stenosis, newer understanding of anatomy of ligamentum flavum can make our access and treatment more targeted and effective.[2]
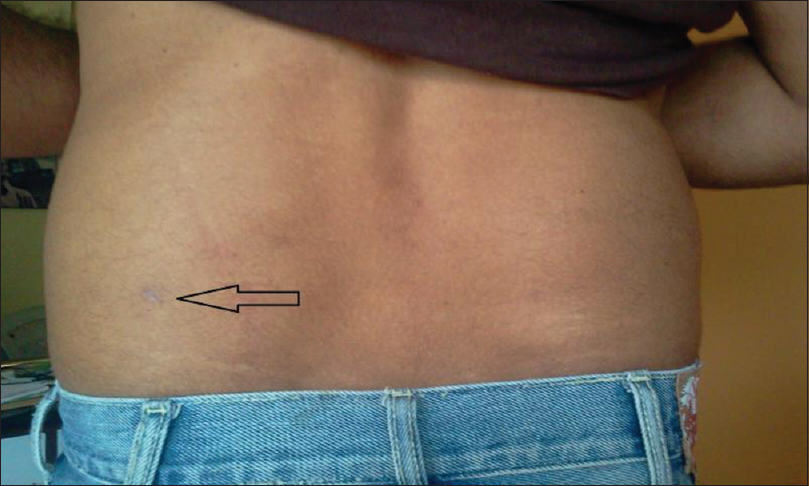
- Stitchless spine surgery
What Is Traditional Thinking About Pain and Claudication and Its Limitations?
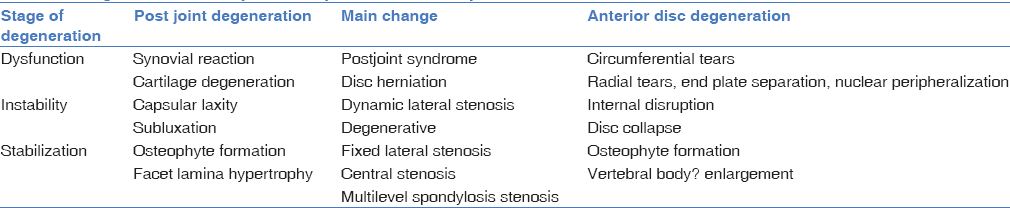
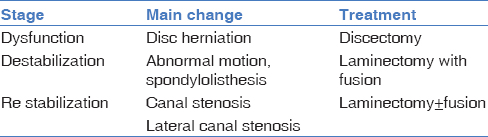
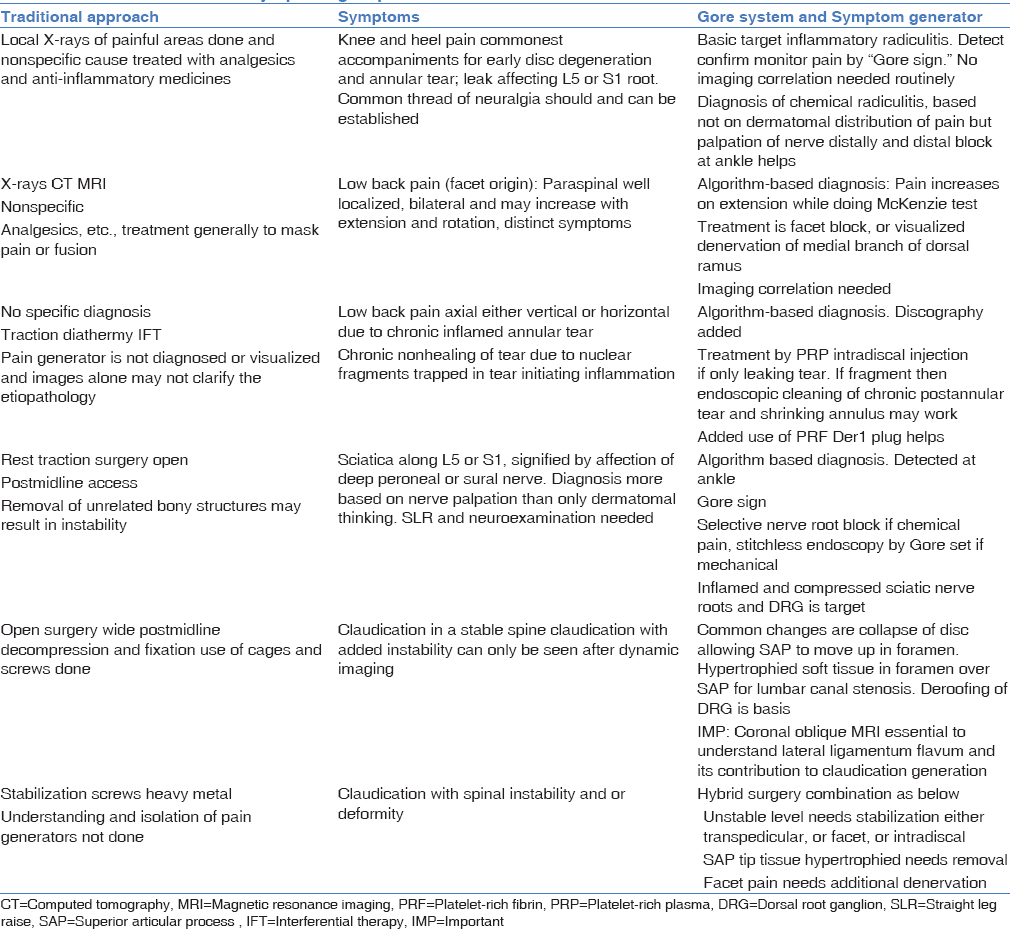
In traditional degenerative cascade, anteriorly disc and posteriorly facet changes were staged as dysfunction, instability, and then stabilization. Changes seen in cadaver and images have defined surgical treatment till the recent past. The cadaver study-based degenerative cascade by Kirkaldy-Willis leads to emphasis on decompression and stabilization [Tables 1 and 2]. The cadaver study selectively ignores nerve supply of functional spinal unit, location of dorsal root ganglion (DRG) in relation to the segment, asymmetry at that level, changes around DRG, and mechanism of pain, namely, chemical or mechanical. Pain causation is kept in background with emphasis only on anatomical variations and image changes. There is no set time frame for the cascade of changes. Images are known not to correlate with symptoms and pathology only in 30% patients. So our main question, “Where is pain and claudication coming from? and Why it persists?” remains unanswered.
Technology such as robotic navigation is proposed as an answer in general, but we do not understand the biochemistry of pain and biomechanics causing claudication and so continue to fail as surgeons. The clinical assessment alone is inadequate to address the present issues as we have no sign for differentiating mechanical and chemical radicular pain, we have no sign to monitor progress of sciatica or back pain when treated nonoperatively, we have no objective sign for pain, and we have no thinking on heel and knee pain that may be early forms of sciatica. This causes severe limitations in analysis of the patients' clinical inputs or images and we are uncertain about the effectiveness of the surgical plan. Our recent improved ability to understand pain comes from surgery under local anesthesia. The new understanding about sciatica includes its subsets and stages.[3]
What has Changed in Our Understanding?
Traditional imaging to in vivo visualization
Decision-making in traditional surgery is based mostly on anatomical changes in degenerative cascade, so images depicting these changes become supreme, ignoring minute changes and unable to distinguish chemical and mechanical cause of pain. Imaging has evolved from “myelography” with negative imaging of structures around the dural sac to computerized tomography (CT). Advent of CT scan made us aware of bony structures and cross-sectional anatomy and real change was advent of magnetic resonance imaging (MRI). However, MRI lacks correlation with pain. Once MRI is available, understanding of pathoanatomy changed but still biochemistry and neurophysiology was out of purview of the surgeons. Creating a very unusual situation where overemphasis on anatomy and pathoanatomy led to “image-guided decision-making” prevails even today.
This is wrongly complemented by “untimely” and “premature” unindicated stabilizations which allegedly mimic natural end stage of stabilization in degenerative cascade. The methodology has become so skewed now that more aggressive decompression is recommended and stabilization is promoted for almost all disc surgeries. We note multiple examples associated with failed surgery where patients remain symptomatic, only with a better-looking image as end point of the intervention.
Need for in vivo visualization
It is known that images match the anatomy to only about 87%. To overcome this difficulty and make our treatment fine-tuned, we need refined visualization of the interface where symptoms are generated and its correlation with pathoanatomy and physiology is now possible in awake and aware surgery where we probe the pain generators and pathology during in vivo visualization. The pain then can be better correlated.
Minute structural changes in early part of degeneration are now appreciated better due to in vivo visualization and so managed well. Degeneration unlike aging is structural failure and symptoms including pain and claudication are response of the nervous system to this structural failure. Now, we can visualize this pain generator, e.g., annular tear by awake and aware surgery under local anesthesia (in vivo visualization) by transforaminal endoscopy and correlate symptom and pathology better. Pain generator is physiological target of treatment and has been repeatedly ignored by overemphasis on images. It has led to many failures in the past, e.g., in case of disc, if the outline of the disc is not changed, most clinicians are clue less as to what intervention is relevant.
Our ability to visualize the symptomatic area in vivo in awake and aware patients to “see” pain generator and put back this learning in clinical analysis has resulted into our matrix changing our approach to plan back and leg pain management. Matrix is a clinical symptom-based cascade adding an element of time and some predictability to the progression of changes and better correlation with symptoms.
Degenerative annular tear starts inside out. Once it reaches out to nerve supply depending on location and type of the tear and neurovascular changes, at this interface, it becomes symptomatic as back or leg pain. It may heal and become asymptomatic. Traditional surgery never had an inside view of the “disc” ignoring that the problem started inside as “annular tear.” It never highlighted interface of disc and nerve DRG and changes in this interface and how to precisely target this symptom generating structural failure. Traditional surgery was and is blind to these changes. Start and early stages of degeneration were thus ignored in traditional treatment.
Proposing microdiscectomy as gold standard stopped further refinements and evolution of traditional philosophy. Microdiscectomy and supposed refined versions of targeting disc herniation are practiced widely. The surgery has evolved from discectomy and laminectomy to more decompression and stabilization for all stages of the degenerative cascade [Figure 2]. It highlighted better visualization of “tip of the iceberg in cases of herniation” completely ignoring early-stage basic annular tear and inflammatory change at disc and nerve interface. Inflammation is known to give patchy pain along sciatic nerve; like knee and heel pain.
Decompression was promoted as therapeutic and refinement only came in form of better decompression by use of access tubes and camera, light source and scope at site of interlaminar surgery. More aggressive decompression slowly set in as better modalities of stabilization emerged. More aggressive decompression many times leads to instabilities begetting more stabilization. Hence, evolution of traditional surgery started with more decompression and stopped at more stabilization. Today, even though we do not have any evidence supporting use of stabilization and hardware in degenerative spine except may be in instability or deformity, it is taken as norm.
Access itself at times was promoted as treatment modality, e.g., laminectomy and “decompression” never highlighting the key target “inflammation” at disc or facet and nerve interface. This entirely has missed the point “where is the pain coming from and why is it persisting, how do we reach the pain generator and take care of it?”
Decompression to targeted treatment of pain generator
Our new philosophy has evolved from basic idea of taking care of pain generator in all its manifestations and at all stages of symptom cascade and has evolved over time. We take care by ablating, washing, irrigating, and excising. Surgical stabilization if 360° by its very nature destroys the pain generators and nerve supply. It still may not relieve the pain if all pain generators are not removed.
Pain generation now in common cases of radiculitis is well understood. In cases of stenosis, it needs further refinement in understanding. The importance of DRG in foramen forming lateral wall of the safe triangle and importance of transforaminal ligament is not yet appreciated fully. Location of L45 DRG is intraforaminal L5S1 it is intracanal just inside foramen, so access through foramen to peri DRG area is basis of transforaminal access under local anesthesia. The access is to nearby inflamed symptom generating interface so can be of subcentimeter size.
The change
In summary, our approach changed from decisions based on history, images, and cadaver anatomy in degenerative cascade to in vivo visualized pathology of symptom generator at surgery under local anesthesia with awake and aware patients. Learning from this gave us the matrix and the clinical cascade. This further led to targeted surgery for the symptom generator with subcentimeter access. Surgery included irrigation, ablation, lavage, decompression, mobilization, and stabilization. The anatomical target being subcentimeter is stitchless.
Simultaneous social changes in expectations from surgery and predicted surgical morbidity, issues about general anesthesia, complications from surgery, access-related inevitable negative outcomes, age- and medical comorbidities-related limitations, and fear of surgery have now led to a new idea and platform “awake and aware surgery” or stitchless surgery under local anesthesia in symptomatic lumbar spine.
Figure 3 shows the schematic change at skin and target. In open traditional or microlumbar disc surgery, surgical damage is like a cone. Skin cut is long and working area smaller with intervening destruction or denervation of tissue. In endoscope-assisted surgery, it is like tent, small skin cut but large tissue dissection under it. In transforaminal endoscopy, there is subcentimeter skin cut and muscles are not cut but dilated and small millimeter cut at intended target.
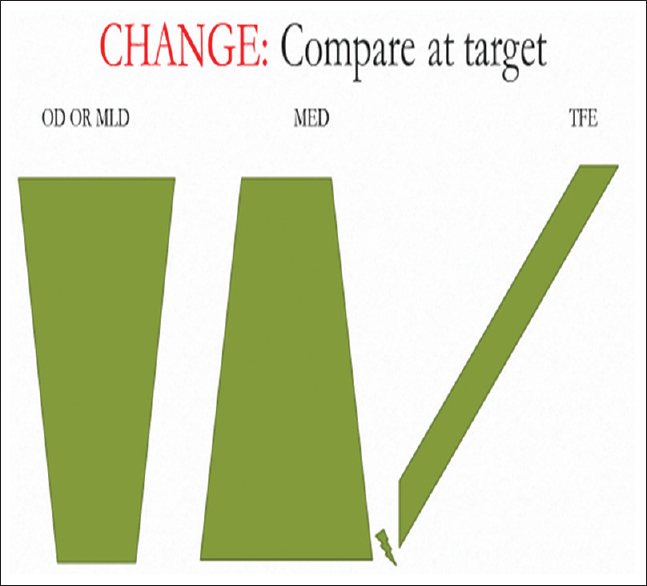
- Minimally invasive at target
New Gore symptom matrix replaces cadaver degenerative cascade or image-based decisions.
Six common variants of symptoms and relevant treatment targets summarized as Gore Matrix© and clinical cascade [Table 3].
Matrix has resulted in a shared decision focused on a broader spectrum of surgical as well as nonsurgical treatments and not only masking the pain generator.
It has moved away from decisions based on diagnostic images alone that cannot explain the pain experienced by everyone as images do not always show variations in nerve supply and pathoanatomy.
Attention to pain pattern and mechanisms and nerve supply of the functional spinal segment is important. The ability to isolate and visualize “pain” and other symptom generators in the foramen and treating persistent pain or claudication by visualizing inflammation and compression of DRG and nerves, essentially located in a small limited juxtaforaminal area in the lumbar spine, is the basis for stitchless surgery under local anesthesia. There is a better algorithmic presurgical planning with more specific and defined goals in mind. In case of stenosis, newer three-dimensional visualization in fusion CT MRI images of the ligamentum flavum in foraminal juxta DRG area has made us refine our targets in claudication. We move away from midline to foraminal area and deroof the DRG in and around foramen.
Refinement in answers to fundamental questions about origin of symptoms has led to stitchless surgery of the functional spinal unit under local anesthesia.
Gore system is a comprehensive group of solutions covering all spectrum of symptoms in degenerative lumbar spine. Learning from awake and aware surgery about pain manifestation, pain generators, and symptom generators in canal stenosis is put back into promoting a paradigm shift in spine surgery. The same philosophy then is extended to the development and design of specific instruments to achieve the surgical goals.
The minimum is a needle that helps in accessing the pain generator and masking it. This masking may result in a better decision-making and prediction.
REFERENCES
- The “inside out” transforaminal technique to treat spinal pain in an awake and aware patient under local lumbar anesthesia: Results and a review of the literature. Available from: http://ijssurgery.com/10.14444/1028
- [Google Scholar]
- Lumbar Stenosis: Oblique Coronal Images in MRI for assessment of Ligamentum Flavum. J Spinal Surg. 2016;3:117..
- [CrossRef] [Google Scholar]
- Sciatica: Detection and Confirmation by New Method. Available from: http://ijssurgery.com/10.14444/1015
- [Google Scholar]




