
Translate this page into:
Malignant peripheral nerve sheath tumor presenting as pathological fracture of femur in neurofibromatosis patient
Address for correspondence: Dr. Suhailur Rehman, Department of Pathology, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, Uttar Pradesh, India. E-mail: suhailurrehman2k2@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Khan R, Rehman S, Maheshwari V, Alam K. Malignant peripheral nerve sheath tumor presenting as pathological fracture of femur in neurofibromatosis patient. J Orthop Allied Sci 2017;5:84-7.
Abstract
Malignant peripheral nerve sheath tumors (MPNSTs) are rare soft tissue sarcomas that arise from a peripheral nerve or cells associated with the nerve sheath, such as Schwann cells, perineural cells, or fibroblasts. MPNSTs account for 5%–10% of all soft tissue sarcomas. Neurofibromas in Neurofibromatosis-1 (NF-1) may undergo malignant transformation in 2%–5% of patients. We are reporting a very rare case in NF-1 patient who, presented with pathological intertrochanteric fracture of femur and liver metastasis. X-ray from left hip joint shows lytic lesion which on histopathology turned out to be MPNST. S-100 was positive confirming its neural origin. Elbow lesion which was excised later, also showed similar features with S-100 positivity. Ultrasonography abdomen showed target lesions in liver. Fine-needle aspiration cytology from liver showed scattered malignant spindle cells. A final diagnosis of metastatic MPNST was made. Although malignant transformation in neurofibromas is extremely rare when it occurs, it is associated with NF-1 in 75% of patients. This case highlights the possibility of fracture femur as the presenting complains, in patients of NF with malignant transformation. The case is unique with regard to its presentation and rarity of metastatic sites.
Keywords
Femur
fracture
liver
malignant peripheral nerve sheath tumor
metastasis
S-100

Introduction
Malignant peripheral nerve sheath tumors (MPNSTs) account for 5%–10% of all soft tissue sarcomas (STSs).[1] Neurofibromas in neurofibromatosis-1 (NF-1) may undergo malignant transformation in 2%–5% of patients.[2] NF is an autosomal dominant disorder of neural crest origin affecting all three germinal layers. Any organ system can, therefore, be involved. Clinically two distinct types are recognized; NF-1, or von Recklinghausen disease affecting 85% of patients, and NF2, or bilateral acoustic neuromas/schwannomas affecting 10% of patients.[3] Distinct multiple cutaneous and/or subcutaneous neurofibromas may develop at any age although rare before adolescence and continue to develop throughout life. Malignant transformation in neurofibromas is extremely rare; however, when it occurs, it is associated with von Recklinghausen disease in 75% of patients.[2,3] They represent one of the most common soft tissue tumors in pediatric age group after rhabdomyosarcoma and usually occur in young adults from a previously predictable plexiform neurofibroma in the perspective of NF-1, with a noted change in size and pain. At present, there are only limited reported data available regarding the occurrence of MPNST in NF-1 in children and adults.[4] Metastasis to brain and bone has been defined in few literatures only.[5] Herein, we report a case of MPNST in NF-1 patient presenting with pathological intertrochanteric fracture of femur and liver metastasis. To the best of our knowledge, this is the first case report of MPNST in NF-1 patient presenting as pathological intertrochanteric fracture of femur.
Case Report
A 54-year-old female with a known history of NF-1, presented to the emergency department, with pain and difficulty in walking following injury to the left hip joint, due to slippage in the bathroom. Clinical examination showed multiple neurofibromas all over the body [Figure 1a]. X-ray both hip joint showed lytic lesion with a fracture in the intertrochanteric region of the left femur [Figure 1b]. Closed reduction and internal fixation with proximal femoral nail were done and debrided tissue sent for histopathological examination. H and E section from the debrided lytic lesion of the femur showed spindle-shaped cells arranged in sheets and fascicles along with the necrotic bone. These cells showed moderate nuclear atypia, hyperchromasia, and coarse chromatin. Mitosis was seen 1–2/hpf [Figure 1c]. Immunohistochemistry for S-100 was positive. A provisional diagnosis of MPNST with metastasis to femur was made. The patient was advised magnetic resonance imaging (MRI) of the elbow lesion and ultrasonography (USG) abdomen for any extension and metastasis. USG abdomen showed multiple target lesions in the liver of variable size. MRI of neurofibroma in elbow region showed features of STS with no bony involvement [Figure 1d]. Excision of the tumor around elbow joint was done and sent for histopathological examination. Gross examination showed 17 cm × 9 cm well defined encapsulated globular tissue with cut section having necrotic, cystic, and hemorrhagic areas [Figure 2a]. H and E section showed hyper and hypocellular areas of spindle-shaped cells with formation of sheets and whorls at places. Thick wall blood vessels with perivascular accentuation of tumor cells were also present. Mitotic activity 1/hpf along with necrosis was also seen. All the margins including deep resection margins and overlying skin was involved by the tumor cells [Figure 2b]. S-100 positivity was seen in the tumor cells [Figure 2c]. Fine-needle aspiration cytology (FNAC) from the liver showed malignant spindle cells scattered along with the normal hepatocytes [Figure 2d]. Keeping in view with all these findings, a final diagnosis of MPNST was made with metastasis to femur and liver. The patient was given chemotherapy and other palliative treatment.
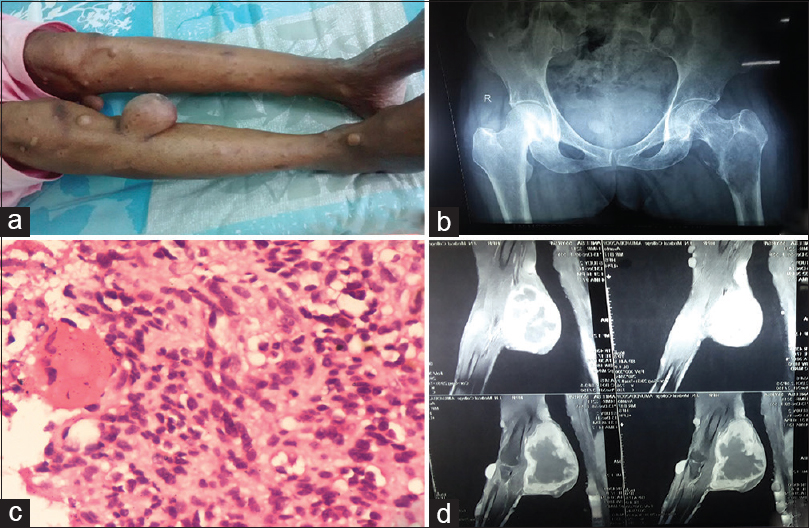
- (a) Multiple neurofibromas seen all over the body. (b) X-ray both hip joint showed lytic lesion with fracture in the intertrochanteric region of the left femur. (c) H and E section (×10) from debrided tissue from femur showed spindle-shaped cells arranged in sheets and fascicles along with the necrotic bone. (d) Magnetic resonance imaging of neurofibroma in elbow region showed features of soft tissue sarcoma with no bony involvement.
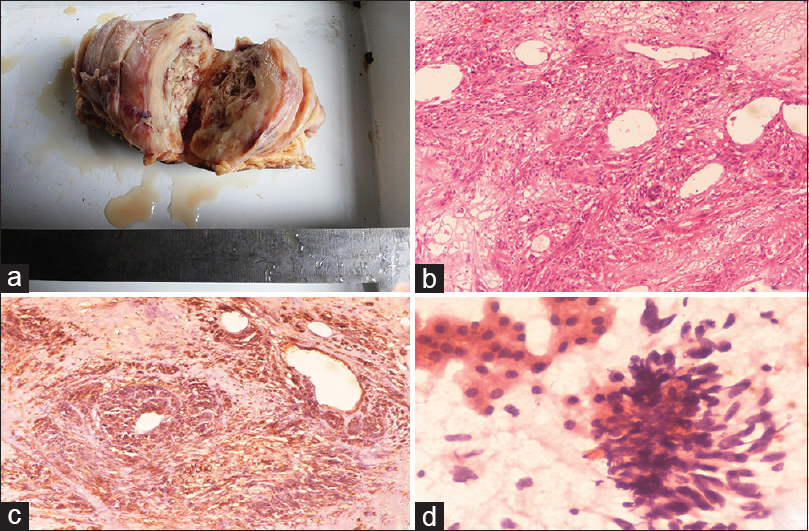
- (a) Gross examination showed well-defined encapsulated globular tissue with cut section having necrotic and cystic areas. (b) H and E section (×10) showed spindle-shaped cells with formation of sheets and whorls at places. Perivascular accentuations of tumor cells were also present. (c) Immunohistochemistry was positive for S-100 in the tumor cells (×10). (d) Fine-needle aspiration cytology from the liver (×10) showed malignant spindle cells scattered along with the normal hepatocytes
Discussion
MPNST is also known as malignant schwannoma, neurofibrosarcoma, and neurogenic sarcoma. These tumors are very aggressive, with an incidence of 5%–10% of all STSs and the STSs staging system proposed by the American Joint Committee on Cancer [AJCC] is most commonly used for staging these lesions. This case presented with stage IV according to AJCC classification.[1,6] Two definite risk factors include NF and previous radiation exposure.[1,7] Malignant transformation in neurofibromas is associated with NF-1 in 75% of patients, and the reported 5-year survival rate is only 15%.[2,3]
Various case reports were found in the literature describing rare sites of MPNST associated with the NF, for example oral cavity,[2] cervical vagus nerve[8], omentum[9] and chest wall.[10] Distant metastasis and high local recurrence are associated with poor prognosis. Only few literatures describe bone and brain as the metastatic sites.[5] This case is unique as the patient presented with pathological intertrochanteric fracture of the femur with a known history of NF-1. Well-defined lytic lesion in the intertrochanteric region of femur, on X-ray hip joint, is exceptional in its own kind and presentation. Differential diagnosis of lytic lesion presenting with pathological fracture in old age includes metastasis, multiple myeloma, and lymphoma.[11]
Histopathologically, MPNSTs are characterized by hypo- and hyper-cellular area having atypical spindle-shaped cells with nuclear pleomorphism, mitosis, necrosis, and a high proliferative index. Perivascular accentuation of tumor cells around blood vessels is also a characteristic feature.[10]
Although histopathological features in a patient of NF are characteristic of MPNST differential diagnosis should be kept in mind while dealing with MPNST. In tumors with monomorphic cell population, differential diagnosis of fibrosarcoma and monophasic synovial sarcoma should be considered. There was no herringbone pattern seen in this patient as seen in fibrosarcoma. Careful search of the monophasic synovial sarcoma having predominantly sarcomatous component also shows foci of epithelial areas forming glands. If the tumor is more bizarre, then the differentials include pleomorphic liposarcoma and malignant fibrous histiocytoma (MFH). The presence of lipoblasts, which is the hallmark of liposarcoma, was not seen in this case. MFH is characterized by storiform pattern of growth, having highly pleomorphic tumor cells and is the diagnosis of exclusion. Metaplastic MPNST should be differentiated from rhabdomyosarcoma, osteosarcoma, chondrosarcoma, or liposarcoma.[12,13]
Characteristic histopathology and S-100 confirms the malignant transformation of neurofibromas present over the elbow, into MPNST. Similar morphology on histopathological examination of femur lesion along with S-100 positivity, confirms the metastatic MPNST. S-100, which is traditionally regarded as the best marker for MPNST, is positive in about 50%–90% of the tumors.[13] Other than S-100, CD56 and protein gene product 9.5 (PGP 9.5) are also considered sensitive markers for peripheral nerve sheath tumors. Although sensitive, CD56 and PGP 9.5 expression is in no way specific for tumors of MPNST.[13,14]
FNAC from the liver showed malignant spindle cells scattered along with the normal hepatocytes. This finding further supports the diagnosis and making liver as another rare site of metastasis in case of MPNST.
MPNST is usually associated with poor prognosis and in general, has limited treatment options. The reason for poor prognosis is high local recurrence rate and distant metastasis.[5] Patients with distant metastasis, are usually given chemotherapy and palliative treatment.
Conclusion
Although malignant transformation in neurofibromas is extremely rare when it occurs, it is associated with NF-1 in 75% of patients. Keeping in view with this fact, it is essential for every patient of NF to be in regular follow-up, to reduce the chances of malignant transformation and metastasis. Earlier detection of metastasis will reduce the morbidity of the patient. This case highlights the possibility of fracture femur as the presenting complains, in patients of NF with malignant transformation.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Acknowledgment
We would like to thank Dr. Roobina Khan, Dr. Suhailur Rehman, Prof. Veena Maheshwari and Prof. Kiran Alam together screened and diagnose this case and guided in writing this paper.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- A case report of malignant peripheral nerve sheath tumour (mpnst) which present as an acute traumatic sciatic neuropathy. Int J Clin Case Rep. 2014;4:1-4.
- [CrossRef] [Google Scholar]
- A case report of a malignant peripheral nerve sheath tumor of the oral cavity in neurofibromatosis type 1. Case Rep Otolaryngol. 2012;2012:936735..
- [CrossRef] [PubMed] [Google Scholar]
- Malignant peripheral nerve sheath tumor in neurobifromatosis type-1: Two case reports. Cases J. 2009;2:7612..
- [CrossRef] [PubMed] [Google Scholar]
- Malignant peripheral nerve sheath tumors (MPNST) in NF1-affected children. Anticancer Res. 2007;27:1957-60.
- [Google Scholar]
- Multiple brain metastases from malignant peripheral nerve sheath tumour (MPNST) Folia Neuropathol. 2004;42:43-8.
- [Google Scholar]
- Completely resected recurrent soft tissue sarcoma: Primary anatomic site governs outcomes. J Am Coll Surg. 2002;194:436-47.
- [CrossRef] [PubMed] [Google Scholar]
- Malignant peripheral nerve sheath tumors. A clinicopathologic study of 120 cases. Cancer. 1986;57:2006-21.
- [CrossRef] [PubMed] [Google Scholar]
- Malignant peripheral nerve sheath tumor of the cervical vagus nerve in a neurofibromatosis type 1 patient – An unusual presentation. Online J Health Allied Scs. 2010;9:10..
- [Google Scholar]
- Malignant peripheral nerve sheath tumor arising from the greater omentum: Case report. World J Surg Oncol. 2011;9:33..
- [CrossRef] [PubMed] [Google Scholar]
- Malignant peripheral nerve sheath tumor of the chest wall associated with neurofibromatosis: A case report. J Thorac Dis. 2013;5:E78-82.
- [Google Scholar]
- Bone tumors and tumorlike conditions: Analysis with conventional radiography. Radiology. 2008;246:662-74.
- [CrossRef] [PubMed] [Google Scholar]
- Pathology of peripheral nerve sheath tumors: Diagnostic overview and update on selected diagnostic problems. Acta Neuropathol. 2012;123:295-319.
- [CrossRef] [PubMed] [Google Scholar]
- Malignant peripheral nerve sheath tumors: Differentiation patterns and immunohistochemical features – A mini-review and our new findings. J Cancer. 2012;3:303-9.
- [CrossRef] [PubMed] [Google Scholar]
- Protein gene product 9.5 (PGP 9.5) is not a specific marker of neural and nerve sheath tumors: An immunohistochemical study of 95 mesenchymal neoplasms. Mod Pathol. 2003;16:963-9.
- [CrossRef] [PubMed] [Google Scholar]




