
Translate this page into:
Luxatio erecta: A case series from a tertiary care centre in North India
Address for correspondence: Dr. Ganesh Singh Dharmshaktu, Department of Orthopaedics, Government Medical College, Haldwani - 263 139, Uttarakhand, India. E-mail: drganeshortho@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Dharmshaktu GS, Khan I, Singh P. Luxatio erecta: A case series from a tertiary care centre in North India. J Orthop Allied Sci 2017;5:55-6.
Sir,
The absence of good congruity and reliance on supportive soft-tissue envelope is an inherent anatomical feature, leading to increased risk of dislocation of shoulder joint. Inferior joint dislocation is rarer forms of shoulder dislocation, with reported incidence of 0.5% in the literature.[1] Most of the cases with true inferior variants had been associated with conditions involving joint effusion, labral damage, or muscle weakness.[2] Characteristic posture of hyperabducted shoulder with painful limitation of adduction is the key diagnostic and presenting feature.
Case 1 – A young male patient consulted us in the emergency department following shoulder injury presented with his right upper extremity held in abduction at shoulder and flexed at elbow. The active and passive attempt of adduction was painful, thus not permitted by the patient. There were severe pain and discomfort with intact distal neurovascular status. The characteristic attitude was suggestive of luxatio erecta. Radiograph confirmed the dislocation of head of humerus out and inferior to the glenoid cavity. The shaft of the humerus was lying parallel to the scapular spine, suggestive of inferior dislocation. Emergent closed reduction under short general anesthesia was attempted after proper informed consent. A longitudinal traction along the line of deformity was given with one assistant providing countertraction over the axillary area maneuvering the humeral head back into the glenoid cavity till subjective feeling of relocation was felt and later confirmed under image intensifier. Uneventful reduction followed shoulder immobilizer of appropriate size applied with active physiotherapy of the elbow or fingers. Case 2 and 4 – Both cases presented as bus fell into a gorge while they were holding a metallic bar in the bus facing sudden jolt with hyperabduction at shoulder [Figures 1 and 2]. The technique used in Case 1 was applied in one case and two-step technique in the other with success. Case 3 was a truck driver with history of road traffic accident. His affected upper extremity was caught in the vehicle while the body was thrown out after collision, thus hyperabducting the arm. The associated pneumothorax following rib fractures was managed by the surgical unit. The relevant details about cases are depicted in Table 1.

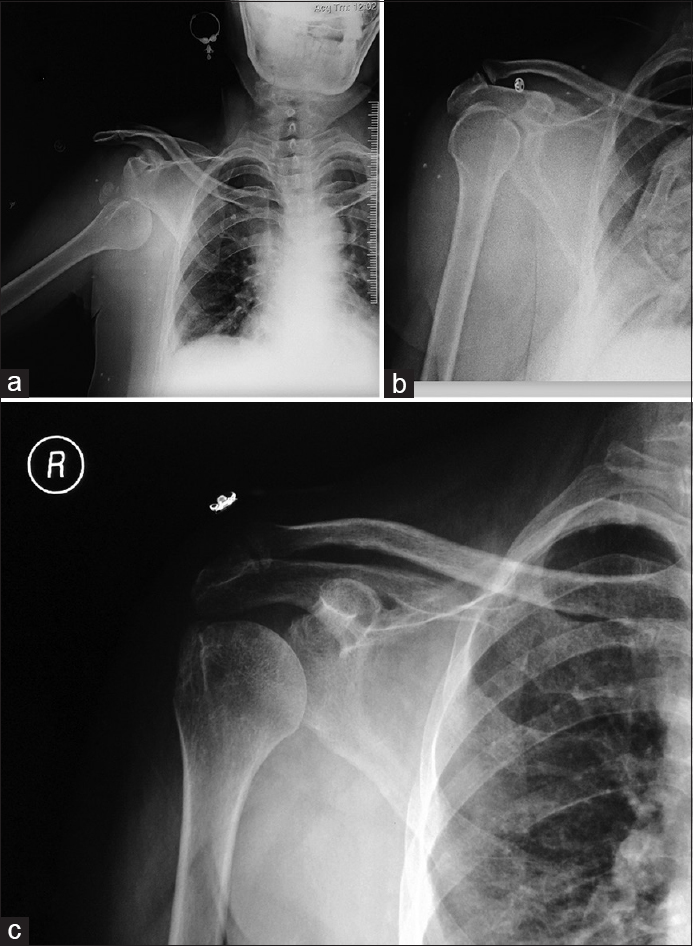
- Radiograph of right inferior dislocation with greater tuberosity fracture (a), immediate postreduction (b), and follow-up with united fracture (c)
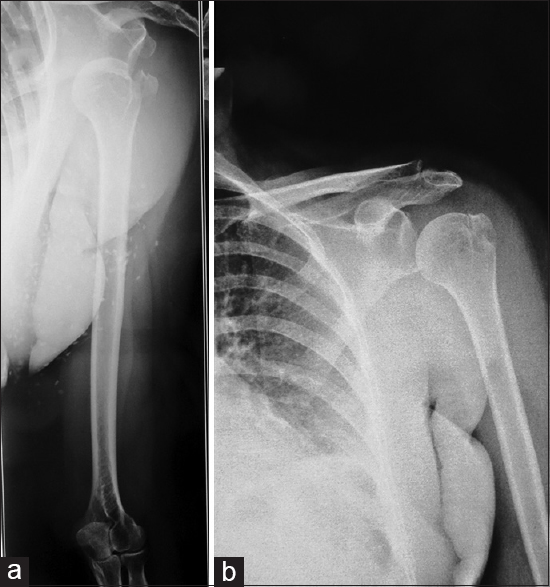
- Radiograph of right inferior dislocation with greater tuberosity fracture (a) and follow-up with united fracture (b)
The follow-up showed no recurrence and stable joint in all cases. A compliant rehabilitation program ensured satisfactory outcome with quick disability of arm, shoulder, hand used to measure the outcome.
The inferior dislocation is the result of either direct or an indirect pattern of injury. Direct injury results from axial loading of a fully abducted arm, while indirect mechanism involves hyperabduction stress directing humeral head inferiorly by placing humeral neck against the acromion process.[3,4] A full trauma series including anteroposterior, lateral, and scapular Y-view should be a norm to better assess these injuries.[5] The characteristic feature is a shaft of the humerus lying parallel to the scapular spine, with head placed subglenoid or subcoracoid.[2,3,5] The two-step maneuver described by Nho et al. has been an effective method and used successfully.[6] We used traditional traction-countertraction method with successful result.[7]
The associated vascular injury to axillary artery has been reported to be mostly found in elderly patients although overall incidence is 3.3%.[5,8] Associated axillary or other nerve injuries such as median, ulnar, or radial should be assessed and their incidence is increased in the presence of associated vascular injury or greater tuberosity fractures.[3,8] Thankfully, our cases had no immediate or remote features of associated neurovascular insult. The adequacy of reduction was assessed in postreduction radiograph and arm splinted for subsequent tissue healing and to decrease the risk of recurrence.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Results of treatment of luxatio erecta (inferior shoulder dislocation) J Shoulder Elbow Surg. 2010;19:423-6.
- [CrossRef] [PubMed] [Google Scholar]
- Locked posterior dislocation of the shoulder. J Bone Joint Surg Am. 1987;69:9-18.
- [CrossRef] [Google Scholar]
- Luxatio erecta (inferior dislocation of the shoulder): A report of 5 cases and a review of the literature. Am J Orthop (Belle Mead NJ). 2003;32:601-3.
- [Google Scholar]
- Locked anterior-inferior shoulder subluxation presenting as luxatio erecta. J Emerg Med. 2004;27:245-8.
- [CrossRef] [PubMed] [Google Scholar]
- Luxatio erecta: Clinical presentation and management in the emergency department. J Emerg Med. 2005;29:85-9.
- [CrossRef] [PubMed] [Google Scholar]
- The two-step maneuver for closed reduction of inferior glenohumeral dislocation (luxatio erecta to anterior dislocation to reduction) J Orthop Trauma. 2006;20:354-7.
- [CrossRef] [PubMed] [Google Scholar]
- Subluxations and dislocations about the glenohumeral joint. In: Rockwood CA, Green DP, eds. Fractures in Adults Vol 2. (5th). Philadelphia, PA: Lippincott; 2002. p. :1160.
- [Google Scholar]
- Axillary artery injury secondary to inferior shoulder dislocation. J Emerg Med. 2010;39:599-601.
- [CrossRef] [PubMed] [Google Scholar]




