
Translate this page into:
Lumbosacral lipoma and low-lying cord with minimal deficits
Address for correspondence: Dr. Amit Agrawal, Department of Neurosurgery, Narayana Medical College Hospital, Chinthareddypalem, Nellore - 524 003, Andhra Pradesh, India. E-mail: dramitagrawal@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Agrawal A. Lumbosacral lipoma and low-lying cord with minimal deficits. J Orthop Allied Sci 2017;5:91-2.
Sir,
Spinal lipomas are congenital lesions formed due to an abnormal embryonic development in the process of separation of primitive ectoderm into neuroectoderm, neural crest, and cutaneous ectoderm.[1,2] A 23-year-old female presented with urinary incontinence for the last 5 years. There were no other deficits. No history of back pain. Local examination revealed no localized swelling, no tenderness over spine or any abnormal pigmentation in the lower lumbosacral. There were no specific abnormal findings on the neurologic examination. The magnetic resonance imaging (MRI) showed diffuse subcutaneous fat masses with high signal intensities in T1- and T2-weighted images from the S1 area to the sacrum [Figures 1 and 2]. Through the bony defect from S1, the subcutaneous fat was connected to the spinal cord (that was extending till S1). There was no evidence of abnormal signal change in the spinal cord. Although the conus medullaris showed tethering down to the S1 area, there were no neurological deficits except bladder dysfunction. In view of extensive involvement and minimal deficits, the patient was managed conservatively. Lipomas arising in the lumbosacral are rare but the most common cause of tethered cord syndrome and occur in 4–8 per 100,000 of the general population.[3-7] Lipomyeloceles and lipomyelomeningoceles are clinically frequently asymptomatic and characterized by the presence of a subcutaneous fatty mass above the intergluteal crease.[8] Although these lesions are benign because of their of communication with connections with the spinal cord, filum terminale, or cauda equina can cause spinal cord tethering with consequent neurological deterioration.[5-7,9-11] In some patients, the deficits may not occur until middle age and if occurs then usually in the form of bladder incontinence.[11] The present case was unique as in spite of the large size of the lesion the patient had only urinary incontinence and no other neurological deficits. Although the computed tomography scan has greatly facilitated the diagnosis of occult spinal dysraphism and intraspinal lesions, MRI is the investigation of choice for detail investigation of these patients.[12,13] MRI will provide additional images in the coronal, transaxial, or oblique planes to define the conus tip better make the identification of the filum terminale easy.[14] The management of patients with spinal lipoma who are asymptomatic or had minimal deficits is controversial and ranges from prophylactic surgery to a regular follow-up.[5-7,15-17] It has been shown that there are poor postoperative results when the terminal lipoma is attached to the conus, compared with good results when it is attached to the filum terminale.[17] In the present case, the cord was extending till lower lumbar level, and there was a lipomatous continuation of the conus as well as filum. The patient had minimal deficits and also it was almost impossible to perform prophylactic surgery.
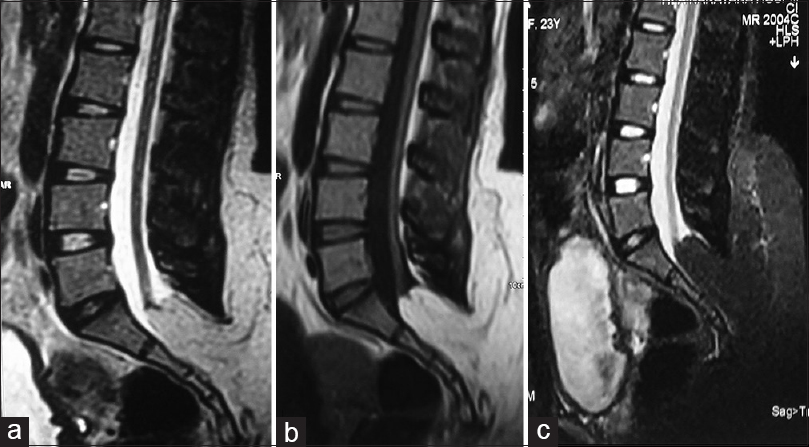
- Magnetic resonance imaging lumbar spine showing low-lying cord and extensive lipoma arising from low-lying conus (a) T2-weighted image, (b) T1-weighted image, and (c) fat suppression image
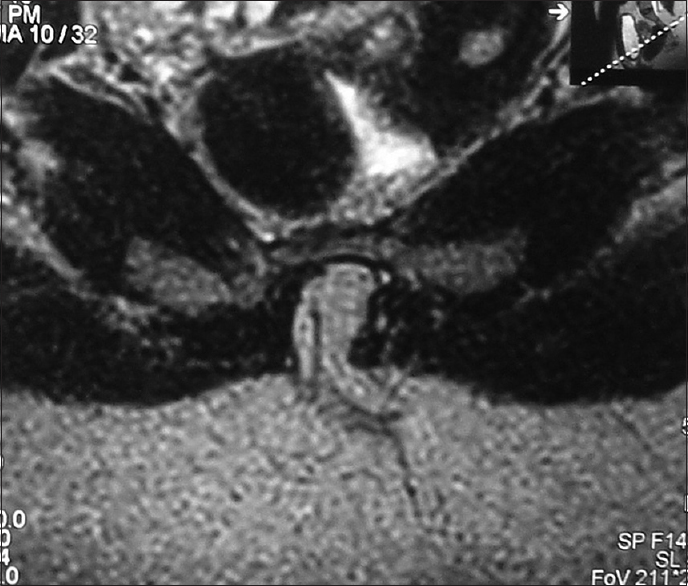
- Magnetic resonance imaging lumbar spine fat suppression image showing continuation of the filum terminale as a lipoma into the subcutaneous tissue
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Pathogenesis of lumbosacral lipoma: A test of the “premature dysjunction” theory. Pediatr Neurosurg. 2001;34:124-30.
- [CrossRef] [PubMed] [Google Scholar]
- A new understanding of dorsal dysraphism with lipoma (lipomyeloschisis): Radiologic evaluation and surgical correction. AJR Am J Roentgenol. 1983;140:1065-78.
- [CrossRef] [PubMed] [Google Scholar]
- Spinal lipomas in infancy and childhood. Childs Brain. 1979;5:192-203.
- [CrossRef] [PubMed] [Google Scholar]
- Management of lipomyelomeningoceles. Experience at the Hospital for Sick Children, Toronto. J Neurosurg. 1985;62:1-8.
- [CrossRef] [PubMed] [Google Scholar]
- Spinal lipomas in children. Pediatr Neurosurg. 2000;32:295-307.
- [CrossRef] [PubMed] [Google Scholar]
- Spinal lipomas in children: Outcome of 270 procedures. Pediatr Neurosurg. 1997;26:8-16.
- [CrossRef] [PubMed] [Google Scholar]
- Intraspinal lipomas with spina bifida. Prognosis and treatment in 73 cases. J Neurosurg. 1986;65:756-61.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging in spine and spinal cord malformations. Eur J Radiol. 2004;50:177-200.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical outcome differences for lipomyelomeningoceles, intraspinal lipomas, and lipomas of the filum terminale. Neurosurg Rev. 2001;24:192-4.
- [CrossRef] [PubMed] [Google Scholar]
- Pathophysiology of “tethered cord syndrome”. J Neurosurg. 1981;54:494-503.
- [CrossRef] [PubMed] [Google Scholar]
- Lumbosacral lipomas: Critical survey of 26 cases submitted to laminectomy. J Neurol Neurosurg Psychiatry. 1967;30:174-81.
- [CrossRef] [PubMed] [Google Scholar]
- Magnetic resonance imaging of lipomyelomeningocele and tethered cord. Neurosurgery. 1989;25:336-40.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis of tethered cords by magnetic resonance imaging. Surg Neurol. 1988;30:60-4.
- [CrossRef] [PubMed] [Google Scholar]
- Magnetic resonance imaging of the pediatric spine. Radiographics. 1987;7:1129-52.
- [CrossRef] [PubMed] [Google Scholar]
- Conservative management of asymptomatic spinal lipomas of the conus. Neurosurgery. 2004;54:868-73.
- [CrossRef] [PubMed] [Google Scholar]
- Results after surgery for lumbosacral lipoma: The significance of early and late worsening. Childs Nerv Syst. 1999;15:439-42.
- [CrossRef] [PubMed] [Google Scholar]
- Congenital lumbosacral lipomas. Childs Nerv Syst. 1997;13:298-334.
- [CrossRef] [PubMed] [Google Scholar]




