
Translate this page into:
Joint line restoration in total knee arthroplasty
Address for correspondence: Dr. Nishikant Kumar, AIIMS, New Delhi, India. E-mail: knishikant@ymail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Kumar N, Mukhopadhaya J, Yadav C, Anand S, Singh S. Joint line restoration in total knee arthroplasty. J Orthop Allied Sci 2017;5:10-4.
Abstract
Total knee Arthroplasty is the most common and successful surgery world wide. Foundation of TKA is based on three pillars soft tissue balancing, bone cuts and cementing. All these factors are equally important and mistake at any level will lead to failure. We here would like to add the fourth pillar 'Joint line Restoration' for successful TKA.
Keywords
Adductor ratio
kinematic axis
patellofemoral

Introduction
Total knee arthroplasty (TKA) is the most commonly performed surgery worldwide. It is now being done in small towns and setups. TKA is a promising surgery for the relief of symptoms of patients with severe arthritic knee. Hence, the expectations of patients have increased. Foundation of TKA is based on three pillars soft tissue balancing, bone cuts, and cementing. All these factors are equally important and mistake at any level will lead to failure. We here would like to add the fourth pillar “Joint line Restoration” for successful TKA. In TKA, our aim is to restore mechanical axis, joint line, restoration of patellofemoral alignment, balanced flexion and extension gaps and balancing of soft tissue. Herein, this article we tried to collect evidence for the restoration of joint line and its importance and current practice which is being followed in Indian scenario.
Overview of Biomechanics of Knee Joint (Kinematic Axis)
Knee joint is a ginglymus (hinge) and arthrodial (pivot) joint with 6 degree of freedom including 3 for each rotations and translations. During flexion and extension, there is continuous change of axis of movement with rolling, gliding, and rotation.[1] Tibia flex and extends around a line centered in each femoral condyle [Figure 1 - Green line]. Patella flex and extends around a line anterior and proximal to first [Figure 1] - Violet Line]. Tibia internally and externally rotates around an axis perpendicular to both [Figure 1] - Yellow line]. Surprisingly each of these axes is either parallel or perpendicular to the joint line [Figure 1]. Hence, we need this kinematic alignment[1,2] maintained after the TKA as well.

- Kinematic axis knee
If we put implant proximally and posteriorly (elevation of joint line) retinacular ligaments will be unstable in extension, medial collateral ligament (MCL) will be unstable in extension whereas it will be tight in flexion. If we put implant distally (lowering joint line) retinacular ligaments will be tight in extension while LCL will be tight in extension while LCL will be unstable in flexion. Hence, any change in joint line and natural angle leads to instability and early failure.[2]
The importance of joint line first came to everybody's attention with Figgie et al.[3] (JBJS 1986), who in their study of 116 patients with 2.5 year follow-up concluded that elevation of joint line more than 8 mm at primary TKA is associated with inferior outcomes.
How do Joint Line Malposition Effects Knee Balance
In 1985, Hungerford and Krackow[4] stated that importance of femoral component placement and joint line position relative to femoral origin of collateral and cruciate ligament. Classically this works for cruciate retaining (CR) knee which has advantage of varus/valgus stabilization improved proprioception and control over roll back.[4,5] Prerequisite for CR knee is PCL must be in adequate tension. If the PCL is lax this will lead to tibiofemoral instability, sagging of tibia, posterior tibiofemoral impingement, and limited flexion. While if it is too tight that will lead to excessive femoral roll back with limited flexion and increased polyethylene wear. In case, joint line is elevated PCL may be tensed in 90 degree flexion which requires partial PCL release.[5]
Superficial MCL (sMCL) behaves as near isometric ligament. Alteration in joint line leads to change in isometric point of sMCL. Femoral component malposition leads to excessive strain on insertion of sMCL and lateral collateral ligament relative to the center of rotation which may lead to excessive tensioning and laxity on flexion.[1,3,5,6]
Effect of Elevated Joint Line
Anterior knee pain (patellofemoral)
Decrease range of motion (ROM)
Patella baja
Midflexion instability
Patellar tendon impingement
Accelerated wear.
Anterior knee pain
Joint line elevation leads to increased patellofemoral contact forces. König et al.[7] in their study showed that the patellofemoral joint was more affected than tibiofemoral joint. Stair climbing caused a larger increase in contact force than walking in both patellofemoral and tibiofemoral joint. A joint line elevation of 10 mm caused an increase in patellofemoral joint contact force of 60% of the participant's body weight (BW) during stair climbing, and 30% BW during normal walking. A further elevation of the joint line from 10 to 15 mm only minimally affected the tibiofemoral joint in either activity, with an additional increase in contact force of <6% BW. In the patellofemoral joint, however, this additional joint line elevation further increased the contact forces by about 30% BW during stair climbing, resulting in a total increase of 90% BW compared to the anatomically reconstructed joint line. Thus, a patient of 85 kg could experience an increase in patellofemoral contact forces of up to 750 N with 15 mm joint line elevation.
Decreased range of motion
Joint line elevation leads to patellar maltracking and decreased ROM. According to Chiu et al.[7] elevation of joint line 10 mm or more causes decrease in flexion of more than 25%.
Patella baja
Joint line elevation leads to patella baja and increased patellofemoral joint contact forces leading to decreased ROM and anterior knee pain.
Midflexion instability
Elevated joint line leads to midflexion instability.[8] Knee becomes stable in extension, but becomes unstable as knee is flexed due to relaxing effect of posterior capsule and collaterals. This can be avoided by posterior release, minimizing distal femur cut, and restoring joint line.
Patellar tendon impingement
Elevated joint line leads to patella baja so the patellar tendon impinges over the poly and regular attrition may lead to rupture of extensor apparatus [Figure 2].

- Patellar impingement
How to Determine Joint Line
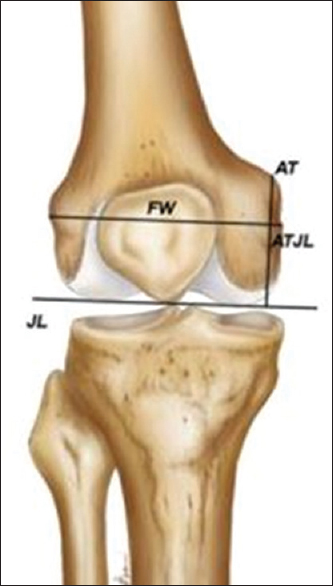
Servien et al.[9] have shown that bony landmarks have to be relied upon to determine our joint line intraoperatively [Figure 3]. Bony landmarks being used to use determine joint line are

- Different tools to measure joint line
Medial femoral epicondyle joint line (MEJL)
Lateral femoral epicondyle joint line
Fibular head joint line (FHJL)
Inferior pole of patella
Adductor tubercle joint line (ATJL).[10]
A properly placed joint line should be approximately 30 mm distal to MEJL, 27 mm distal to lateral femoral joint line and 15 mm proximal to FHJL.[9-11]
The main difficulty with these landmarks is that these landmarks are difficult to localize intraoperatively. Furthermore, since average distance values are used it is not customized individually to every patient. Besides this, there is marked variation between males and females. For Medial epicondyle alone there can be variation up to 60%.
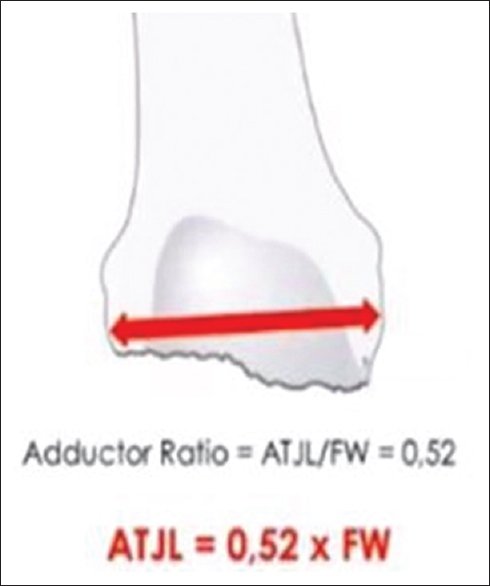
Luyckx et al.[12] reported strong and significant linear correlation between distance from ATJL and center of knee with the femoral width. This signifies that most of variation in ATJL is contributed by difference in femoral width. Hence, a new tool “adductor ratio”[10,12] was found.
Adductor ratio[12] is defined as ratio between ATJL and femoral width [Figure 4]. This comes out to be a constant value (0.52) with almost no variation. Furthermore, no significant difference was found among males and females. The adductor ratio was most accurate ratio and reconstructed joint line within 4 mm of its original level in 92% of the cases. In simple terms, we can say that ATJL is half of femoral width of typical patient. Hence, adductor ratio overcomes size dependent variation.
- Method to measure adductor ratio (adductor ratio = adductor tubercle joint line/femoral width)
However, identifying joint line in revision TKA is difficult as above landmarks are not easily palpable in revision cases intraoperatively. Many surgeons use metal rular under MCL until it abuts its origin. Reference using patella which includes Insall-Salvati ratio, Caton-Descamps ratio and Blackburn-peel ratio can be used in primary TKA of same knee preoperatively or using opposite knee in unilateral TKA and revision TKA. These references are unreliable in revision TKA because of altered anatomy of patella and patella tendons.
How to Measure Joint Line in Revision Total Knee Arthroplasty[13]
As stated above localizing bony landmarks is not easy in revision cases due to bone loss either due to loosening or following implant removal.[12,13]
Steps:
Measure femoral width intraoperatively from metal ruler as distance between most prominent points in femoral condyle [Figure 5]. If there is difficulty in doing this Preoperative X-ray or even contralateral knee can be chosen as well
Now multiply femoral width with 0.52 to get ATJL (roughly half of femoral width)
Introduce intramedullary rod in canal and ATJL distance plotted. Distal femoral cutting block is fixed at ATJL which is plotted [Figure 6]
Now we can assess and select appropriate size of augments to reconstruct joint line.
- Method to determine adductor tubercle joint line in revision total knee arthroplasty
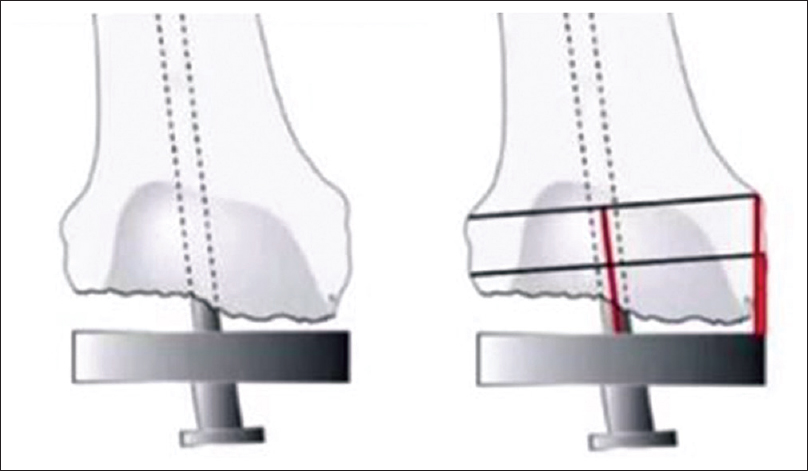
- Method to determine joint line in revision total knee arthroplasty
What are the Reasons of Joint Line Alteration
Primary total knee arthroplasty[10,12-14]
In primary TKA excessive distal femoral cut causes joint line elevation. Some times its difficult to avoid excessive distal femoral cut because of flexion contracture, excessive scarring in sequelae of septic knee and posttraumatic arthritis with bone loss. Occasionally, choice has to be made between full extension and excessive femoral cut, in that case full extension is primary aim.
Revision total knee arthroplasty[14]
In revision TKA, there is bone loss in distal femur due to osteolysis, aseptic loosening, and proximal migration of component or following implant removal. Prosthesis placement over good bone stock of distal femur will lead to large insert placement that causes joint line elevation; however, the use of distal femur augment can restore joint line position near to original one to restore the joint line alignment and biomechanics.
Problems and Solution of Joint Line Unique to Revision Total Knee Arthroplasty[14]
Bone loss - Putting implant over existing bone without reconstruction leads to joint line elevation. This can be resolved with proper use of distal and posterior femoral augments to reconstruct joint line
Use of Stems in femur in revision[15] - Use of stem is common in revision situations. If we use straight stem what happens is because of anterolateral bow of femur the straight stem engages over the bow and pull the implant anteriorly increasing the flexion space. To compensate for this increase in flexion space we need to increase the extension space by increasing distal femur cut thus increasing joint line. This can be best managed by using offset femoral stems.[11,14,15]
How to Avoid Joint Line Malposition[11]
It is clear from above discussion and literature that to obtain adequate gap balancing and midflexion stability joint line restoration is must. After proper preoperative planning joint line must be determined for all primary and revision cases.[11] Extradistal femoral cut must be avoided without posterior release. Over resection of distal femur will lead to elevation of joint line which will be stable in extension but on flexion there will be instability because of relaxed posterior capsule and collaterals.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Does a kinematically aligned total knee arthroplasty restore function without failure regardless of alignment category? Clin Orthop Relat Res. 2013;471:1000-7.
- [CrossRef] [PubMed] [Google Scholar]
- The influence of tibial-patellofemoral location on function of the knee in patients with the posterior stabilized condylar knee prosthesis. J Bone Joint Surg Am. 1986;68:1035-40.
- [CrossRef] [Google Scholar]
- Varus-valgus and rotational stability in rotationally unconstrained total knee arthroplasty. Clin Orthop Relat Res 1987:147-57.
- [CrossRef] [Google Scholar]
- Review article: Knee flexion after total knee arthroplasty. J Orthop Surg (Hong Kong). 2002;10:194-202.
- [CrossRef] [PubMed] [Google Scholar]
- Joint line elevation in revision TKA leads to increased patellofemoral contact forces. J Orthop Res. 2010;28:1-5.
- [CrossRef] [PubMed] [Google Scholar]
- The influence of joint line position on knee stability after condylar knee arthroplasty. Clin Orthop Relat Res 1990:146-56.
- [CrossRef] [Google Scholar]
- Reliability of bony landmarks for restoration of the joint line in revision knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2008;16:263-9.
- [CrossRef] [PubMed] [Google Scholar]
- The adductor tubercle: A reliable landmark for analysing the level of the femorotibial joint line. Knee Surg Sports Traumatol Arthrosc. 2013;21:2725-9.
- [CrossRef] [PubMed] [Google Scholar]
- Joint line restoration after revision total knee arthroplasty. Clin Orthop Relat Res 1999:165-71.
- [CrossRef] [Google Scholar]
- The adductor ratio: A new tool for joint line reconstruction in revision TKA. Knee Surg Sports Traumatol Arthrosc. 2014;22:3028-33.
- [CrossRef] [PubMed] [Google Scholar]
- Joint line restoration during revision total knee arthroplasty: An accurate and reliable method. Springerplus. 2015;4:736..
- [CrossRef] [PubMed] [Google Scholar]
- Joint line position restoration during revision total knee replacement. Clin Orthop Relat Res 2002:169-71.
- [CrossRef] [PubMed] [Google Scholar]
- Modular femoral offset stems facilitate joint line restoration in revision knee arthroplasty. Clin Orthop Relat Res. 2006;446:93-8.
- [CrossRef] [PubMed] [Google Scholar]




