
Translate this page into:
Femoral head chondral delamination injury and associated osteonecrosis: A case report of treatment
Address for correspondence: Dr. Vince W. Lands, St. Luke's University Health Network, 801 Ostrum Street PHPP2, Suite 201, Bethlehem, Pennsylvania 18015, USA. E-mail: vince.lands@sluhn.org
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Lands VW, Malige A, Reddy CS. Femoral head chondral delamination injury and associated osteonecrosis: A case report of treatment. J Orthop Allied Sci 2017;5:51-4.
Abstract
Avascular necrosis can develop secondary to a traumatic or atraumatic interruption of blood supply to a bony region. We present an unusual case of femoral head osteonecrosis in a patient who concomitantly suffered a complete delamination injury to the articular surface and ultimately underwent progressive degenerative changes in the femoral head requiring total hip arthroplasty (THA). A 57-year-old man without significant medical comorbidities presented for orthopedic evaluation in the outpatient setting complaining of left hip pain. The patient reported a slip and fall onto his left hip 4 months prior with no preexisting discomfort. Since then, the progressively worsening pain has centered on the left groin with radiation into the lateral aspect of the hip. Physical examination is negative for focal deficits, but provocative maneuvers for intra-articular pathology were positive. X-rays demonstrated mild degenerative changes while magnetic resonance imaging (MRI) showed a complete delamination injury to the articular surface with associated femoral head collapse. Nonoperative treatment failed to provide pain relief, and so the patient ultimately underwent surgical intervention. Treatment consisted of left uncemented THA with cable augmentation. Postoperatively, the patient was monitored with periodic follow-ups while undergoing postsurgical rehabilitation. Interval improvement was demonstrated and patient overall did well.
Keywords
Avascular necrosis
chondral lesions
osteonecrosis

Introduction
A vascular necrosis (AVN) is a painful and debilitating condition that must be diagnosed and treated promptly to avoid long-term morbidity. This disease is thought to result from an interruption to the blood supply of a bony region. AVN, or osteonecrosis, of the femoral head, occurs due to prolonged ischemia resulting from a loss of blood supply from the medical circumflex and inferior gluteal arteries.[1] Repeated microtrauma and impaired repair leads to cell death and resulting chondral injury, subchondral sclerosis, and bony collapse.[2,3] Patients may present with pain, loss of strength or limited functionality and range of motion in the affected extremity. While trauma to the femoral head and neck can cause osteonecrosis, nontraumatic etiology may also be a cause,[4] including corticosteroid use[5] and alcohol abuse.[6] The development of osteonecrosis in patients with chondral delamination of the articular surface, however, has not been well documented in the literature. Chondral delamination injuries, resulting from forceful impact or extreme torsional loading, involve a fracture of the surface that separates noncalcified articular cartilage from the calcified surface.[7,8] Delamination of the chondral surface coupled with chondral injury caused by AVN potentially complicates treatment success.[9] We present an unusual case of AVN in a patient who concomitantly suffered a complete delamination injury to the articular surface and ultimately underwent progressive degenerative changes in the femoral head requiring total hip arthroplasty (THA).
Case Report
A 57-year-old man presented for orthopedic evaluation in the outpatient setting complaining of the left hip pain. The patient reports slipping 4 months before presentation while plowing snow and falling on his left hip with no preexisting pain. Since falling, the patient consistently complained of progressive pain centered on the left groin with radiation into the lateral aspect of the hip. He reported weakness in the thigh and difficulty with flexing his hip. Physical examination was negative for focal neurological deficits. However, the examination was positive for mild quadriceps wasting and tenderness. The patient had a positive Patrick's test (FABER) with ipsilateral tenderness as well as pain on log roll testing. The patient demonstrated limited active and passive motion ranging from 10° to 100°. Painful and restricted internal rotation and external rotation demonstrated 10° and 0° of motion respectfully. The strength of the affected extremity was graded at 3/5 compared to contralateral extremity effort. X-rays demonstrated loss of sphericity of the femoral head from the 9 O'clock position extending laterally and associated changes in the lumbar spine and sacroiliac joint [Figure 1a-c]. A follow-up MRI revealed degenerative changes within the femoral acetabular joint, femoral head collapse, and complete articular cartilage delamination injury [Figure 2a-c]. Both conservative and operative treatment options were discussed with the patient. The patient initially elected to undergo a single fluoroscopic corticosteroid injection which provided only temporary relief. He subsequently elected to undergo cementless left total hip replacement.
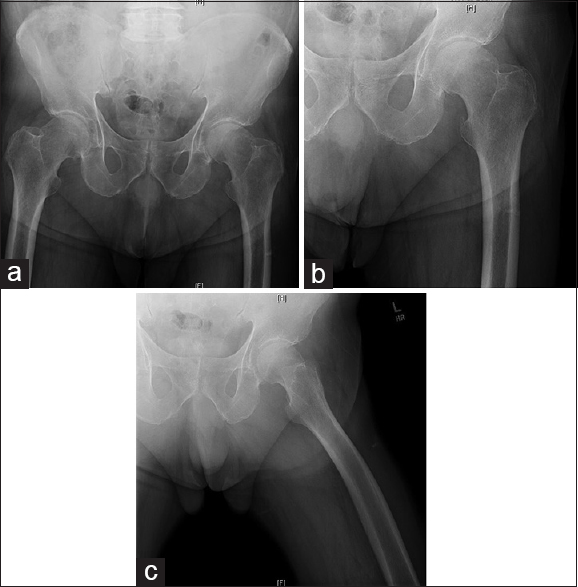
- There is no fracture or dislocation. Minimal narrowing of the hip joint spaces. Loss of sphericity of femoral head. Mild narrowing of the sacroiliac joint right greater than the left. Degenerative changes noted in the lumbar spine. (a) Anteroposterior pelvis X-ray, (b) anteroposterior left hip X-ray, (c) lateral hip X-ray
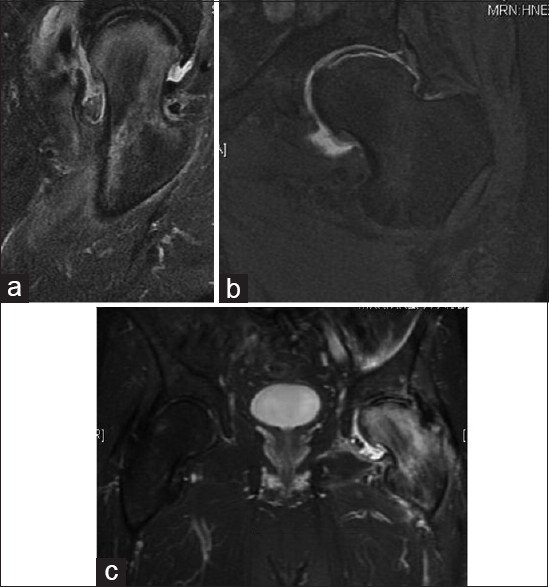
- The study revealed a large area of avascular necrosis of the left femoral head, associated with subchondral collapse. Reactive edema present and a large articular cartilage delamination of the femoral head. (a) Axial, T2-weighted image. (b) Coronal, T1-weighted image. (c) Coronal, T2-weighted image
After an unsuccessful corticosteroid injection provided only temporizing pain relief, the patient underwent cementless left THA. A standard anterior approach was performed utilizing the intermuscular plane between the tensor fascia lata and the sartorius. The femoral head was extracted and visualized intraoperatively, demonstrating a complete delamination of the articular surface > 50% as well as severe end-stage osteoarthritic changes to the femoral head and acetabulum with fraying of the labrum [Figure 3]. Of note, while preparing the femoral canal, the medial femoral cortex was breeched. A prophylactic cable was placed to prevent further propagation. Components consisted of a 56 mm acetabular cup with two screws fixating the interface in appropriate anteversion and abduction, a 15 mm collared stem, and a standard neck with a +1.5 36 mm head. The hip was taken through a stable arc of motion, and the patient was extubated without complication following the procedure.

- Intraoperative image of left femoral head revealing a large delamination injury to femoral head with subchondral collapse
The patient was monitored postoperatively with periodic follow-ups while undergoing rehabilitation. This initially consisted of passive stretching of the hamstrings, quadriceps, hip flexors, and abductors as well as an active range of motion exercises for the hip and knee. Strengthening exercises were slowly incorporated to primarily strengthen the quadriceps, hip abductors, and hamstrings musculature. Deep venous thrombosis prophylaxis was also implemented following surgery. Postsurgical radiographs ordered by the orthopedic surgeon of the left hip showed the presence of an uncemented left total hip prosthesis in good alignment [Figure 4a-c].
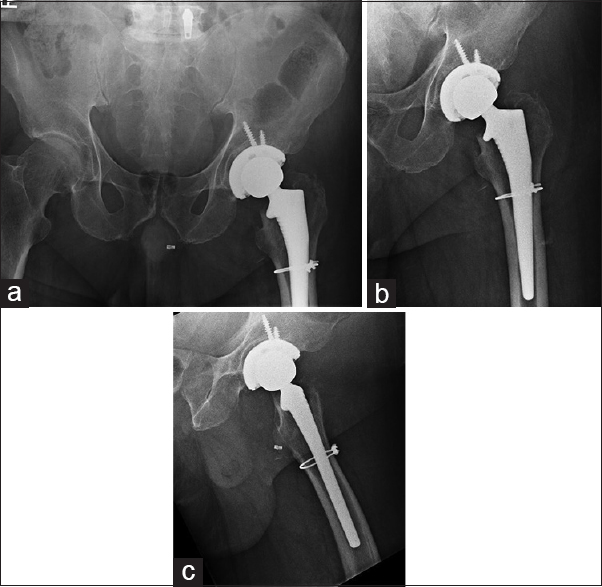
- Postoperative images of left cementless total hip arthroplasty with cable augmentation. (a) Anteroposterior pelvis X-ray, (b) anteroposterior left hip X-ray, (c) lateral hip X-ray
Discussion
Chondral delamination is the separation of the articular cartilage from the underlying subchondral bone at the tidemark. These injuries occur as result of shearing stress that is concentrated at the junction of the noncalcified and calcified cartilage. The delamination line runs parallel to the joint surface, but the overlying articular cartilage remains initially intact. Still, unrecognized and untreated chondral delamination injuries can have poor prognoses,[10] with possible sequelae including further propagation of cartilaginous injury to AVN. Femoral head AVN can further progress into collapse and ultimately result in end-stage degenerative changes. While our patient did not have an initial MRI to prove that he had no preexisting pathology, the accelerated nature of progressive hip pain without any other contributing factor leads one to think that his fall likely could have provided the shear injury to his articular surface allowing for the delamination injury. Furthermore, the patient did not have any significant comorbidities or risk factors which could have contributed to the development of AVN.
The classification of AVN according to standard radiographs has previously been described. Ficat proposed a four-stage classification system describing femoral head changes. In Stage I, the radiographs are normal. In Stage II, the contour of the femoral head is normal but the radiographs show evidence of bone remodeling including cystic and sclerotic areas. Stage III involves flattening of the femoral head. In Stage IV, there is joint space narrowing with secondary degenerative changes in the acetabulum[11,12] The classification system was expanded by Steinberg et al., by dividing stage III lesions into femoral heads with and without collapse or hips with acetabular involvement.[11]
Various treatment options exist for AVN for the femoral head at a precollapse level. These options include, but are not limited to, restricted weight bearing, use of pharmacologic agents such as lipid-lowering drugs, anticoagulants, and vasodilators, core decompression, and the utility of nonvascularized and vascularized cortical grafts.[12] If intervention is not quick and effective, a physician must focus on treatment of resulting end-stage necrosis and degenerative disease. Treatment of this stage is mainly surgical, generally involving a total hip replacement or arthroplasty using either a cemented or cementless prosthesis. Cemented total hip arthroplasties have been reported as being inferior with high failure rates in younger patients and patients with femoral head necrosis because of their inferior durability. Improved outcomes have been reported with cementless total hip arthroplasties for patients with femoral head osteonecrosis.[13]
Conclusion
We present a 57-year-old male with no preexisting hip pain or comorbidities, who fell on his left hip and rapidly progressed to ambulatory dysfunction within a 4-month period. Physical examination was suspicious for intra-articular pathology. X-rays demonstrated mild degenerative changes while MRI showed a complete delamination injury to the articular surface with associated femoral head collapse. Nonoperative treatment failed to provide adequate pain relief and subsequently the patient ultimately underwent uncemented left THA. Postprocedure, the patient was able to return to base ambulatory function.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- The surgical anatomy of the blood supply to the femoral head: Description of the anastomosis between the medial femoral circumflex and inferior gluteal arteries at the hip. Bone Joint J. 2008;90:1298-303.
- [CrossRef] [PubMed] [Google Scholar]
- Avascular necrosis of the femoral head: Vascular hypotheses. Endothelium. 2006;13:237-44.
- [CrossRef] [PubMed] [Google Scholar]
- Pathophysiology and natural history of avascular necrosis of bone. Joint Bone Spine. 2006;73:500-7.
- [CrossRef] [PubMed] [Google Scholar]
- Non-traumatic avascular necrosis of the femoral head. J Bone Joint Surg Am. 1995;77:459-74.
- [CrossRef] [PubMed] [Google Scholar]
- Incidence of osteonecrosis associated with corticosteroid therapy among different underlying diseases: Prospective MRI study. Rheumatology (Oxford). 2011;50:2023-8.
- [CrossRef] [PubMed] [Google Scholar]
- Natural history of nontraumatic avascular necrosis of the femoral head. Bone Joint J. 1991;73:68-72.
- [CrossRef] [PubMed] [Google Scholar]
- Chondral and osteochondral injuries: Mechanisms of injury and repair responses. Oper Tech Orthop. 1997;7:263-9.
- [CrossRef] [Google Scholar]
- Chondral delamination of the knee in soccer players. Am J Sports Med. 1996;24:634-9.
- [CrossRef] [PubMed] [Google Scholar]
- Avascular necrosis complicating chondral resurfacing techniques. Knee Surg Sports Traumatol Arthrosc. 2016;24:1660-4.
- [CrossRef] [PubMed] [Google Scholar]
- MRI appearance of chondral delamination injuries of the knee. AJR Am J Roentgenol. 2005;184:1486-9.
- [CrossRef] [PubMed] [Google Scholar]
- A quantitative system for staging avascular necrosis. J Bone Joint Surg Br. 1995;77:34-41.
- [CrossRef] [Google Scholar]
- Management of avascular necrosis of femoral head at pre-collapse stage. Indian J Orthop. 2009;43:6-16.
- [CrossRef] [PubMed] [Google Scholar]
- Avascular necrosis of the hip in a 41-year-old male: A case study. J Can Chiropr Assoc. 2004;48:137-41.
- [Google Scholar]




