
Translate this page into:
Compound palmar ganglion causing compressive neuropathy of the median nerve
Address for correspondence: Dr. Tribhuwan Narayan Singh Gaur, Department of Orthopaedics, People's College of Medical Sciences and Research Centre, Bhopal - 462 037, Madhya Pradesh, India. E-mail: harishrao27@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Gaur TN, Shah M, Rao H. Compound palmar ganglion causing compressive neuropathy of the median nerve. J Orthop Allied Sci 2017;5:48-50.
Abstract
Tuberculosis (TB) of synovial sheath of tendon is uncommon, it is a severe form of extrapulmonary TB, diagnosis is obvious on clinical grounds in later stages, but is always confirmed by histopathology. Here, we are presenting a case of a 50-year-old female, who presented to us with gradual increasing swelling in her left hand and wrist and numbness over left thenar eminence. The patient was successfully treated with debulking operation and anti-tubercular drugs. Tubercular tenosynovitis of wrist and hand is a severe form of extrapulmonary TB. Intraoperatively, the presence of rice body or melon seed bodies is pathognomonic for confirming the diagnosis. Early diagnosis and intervention give good prognosis.
Keywords
Compound palmar ganglion
neuropathy
tubercular tenosynovitis

Introduction
Isolated tuberculosis (TB) of the synovial sheath or bursa occurs rarely; the disease is thought to reach the synovial sheath by the direct hematogenous spread or from underlying bone or joint. The infected synovium gets edematous and filled with granulation, becomes hyperplastic thickened and villous. Excessive synovial fluid (serous exudates) produces almost painless swelling. With movement and friction, the broken villi and fibrinous exudates get molded to resemble rice body [Figure 1] or melon seed body.[1] Griffith et al.[l] suggested that ultrasonography as an ideal first-line investigation for tenosynovitis to reveal the degree and extent of involvement of the tendon sheath.[2]

- Intraoperative rice body
Palmar synovial bursa is covered by dense palmar fascia when infected it causes inflammation of all tendon sheaths about the hand and wrist resulting in median nerve compression.[3] It can also lead to the destruction of underlying bone if left untreated. It is best treated with early surgical debulking along with antitubercular drugs. We report this case for its rarity and successful early management.
Case Report
A 50-year-old female presented to us with swelling over the left hand and wrist [Figure 2], for 2 years. The swelling started in her left wrist; it was painless initially, but from the last 6 months she expressed tingling, and numbness in left thenar area and the swelling also appeared over hand region. The pain and tingling increase during night. There was no history of loss of appetite or weight loss or evening rise in temperature but family history of TB was present, there was no history of any other joint involvement. On examination, the cross fluctuation was present the entire area of median nerve innervation was numb. X-ray of the hand and wrist was normal did not show any bony involvement. Chest was normal clinically and radiologically, no other lesion of TB was clinically detectable. Ultrasonography [Figure 3] of left wrist and hand suggested synovial thickening and proliferation of flexor digitorum tendon at wrist and hand with the presence of multiple oval shaped hypoechoic bodies. Findings suggestive of infective etiology, on blood examination were erythrocyte sedimentation rate 29 end of first-hour other parameter were within normal limit. Excision biopsy was planned and carried out through volar approach to wrist and hand. Skin and fascia were incised and retracted, flexor retinaculum dissected and median nerve carefully retracted [Figure 4], there was a single continuous fluctuant mass which was filled with fibrinous material and straw colored fluid. The fluid and melon seed bodies evacuated, inflamed tendon sheath excised. These findings were suggestive of tubercular nature of pathology.[4] A through wound wash was given and closed in layers. The histopathology report revealed inflammatory lesion with large granuloma of epithelioid cells and multiple giant cells [Figure 5] and central caseous [Figure 6] material, suggesting tubercular nature of pathology. The patient was treated with anti-tubercular drugs according to the WHO and set the international standard for TB care.[5] Initially, isoniazid (INH), rifampin (RIF), pyrazinamide, ethambutol for 2 months during intensive phase followed by 4 months continuous phase of INH and RIF thrice a week.

- Clinical photo

- Ultrasonography
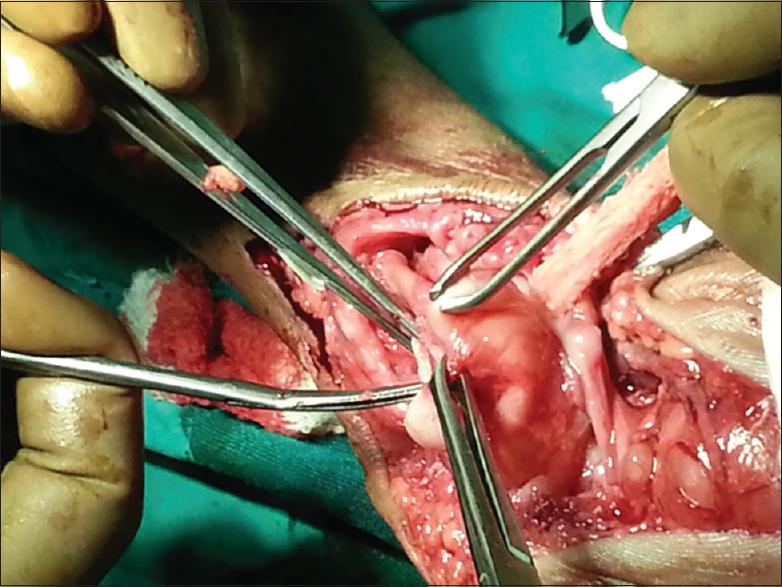
- Intraoperative photo
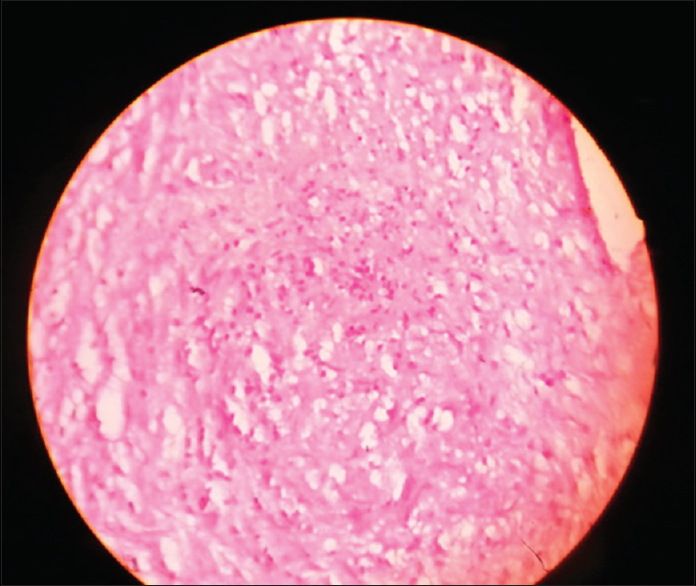
- Histopathology of ganglionic tissue
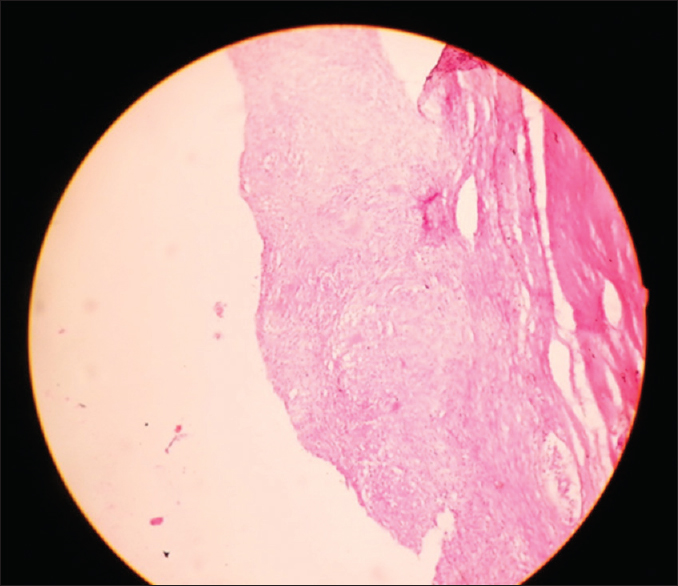
- Histopathology of ganglionic tissue magnified view
The range of movement exercises of wrist and hand were started from the second postoperative day and increased according to the patient's pain tolerance. On subsequent follow patient showed complete recovery from numbness, at the end of 3 months, patient gained full function of the affected side, after 6 months of antitubercular treatment (ATT) completion patient was reviewed and there was no sign of recurrence. Related case report available in literature.[6,7]
Discussion
TB is still widely prevalent in developing countries, in affluent countries due to better socioeconomic status; it is mostly a disease of immunocompromised people. It can affect many organs of the body, but the involvement of synovial sheath of hand is quite rare, TB tenosynovitis of the hand constitutes <1% of skeletal TB[8] that hence diagnosis is delayed. The treatment of the TB of the hand is generally nonoperative surgery is reserved for specific indication, namely biopsy, debridement, fusion of disorganized joint, or carpal tunnel decompression.[9] The diseases are slowly progressive, which causes difficulties in the early diagnosis. Late diagnosis leads to poor functional outcome even in the presence of regular ATT.[10] The diseases are diagnosed early it can be successfully treated conservatively. In a later stage, it can be successfully treated with debulking surgery and ATT.
Interfering with the disease before the involvement of underlying bone is the main goal of treatment.
Clinical message
With the worldwide resurgence of musculoskeletal TB, there is an increased in cases affecting atypical sites, including hand so whenever we are treating the tenosynovitis the diagnosis of TB should always be kept in mind so that early diagnosis and timely intervention can be done for complete recovery of the patient.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Tuberculosis of the Skeletal System: Bone, Joints, Spine, and Bursal Sheaths. (3rd). New Delhi: Jaypee Brothers Medical Publishers; 2004. p. :184.
- [Google Scholar]
- Imaging of musculoskeletal tuberculosis: A new look at an old disease. Clin Orthop Relat Res (398):32-9.
- [CrossRef] [PubMed] [Google Scholar]
- Compound palmar ganglion with carpal tunnel syndrome. J Coll Physicians Surg Pak. 2007;17:230-1.
- [Google Scholar]
- Rice bodies, millet seeds, and melon seeds in tuberculous tenosynovitis of the hand and wrist. Ann Plast Surg. 2011;66:610-7.
- [CrossRef] [PubMed] [Google Scholar]
- Publication Weekly Epidemiological Record, No 5, Date 3rd Feb 2006. An Old Disease. Clin Orthop. 2002;398:32-9.
- [Google Scholar]
- Compound palmar ganglion: A case report and literature review. Ann Saudi Med. 1986;6:55-9.
- [CrossRef] [PubMed] [Google Scholar]
- Tuberculous tenosynovitis of the hand (”compound palmar ganglion”): Literature review and case report. Orthopedics. 1980;3:1093-6.
- [CrossRef] [PubMed] [Google Scholar]
- Atypical extraspinal musculoskeletal tuberculosis in immunocompetent patients: Part II, tuberculous myositis, tuberculous bursitis, and tuberculous tenosynovites. Can Assoc Radiol J. 2006;57:278-86.
- [Google Scholar]
- Tuberculosis of the hand: Clinical presentation and functional outcome in 32 patients. J Bone Joint Surg Br. 2009;91:1054-7.
- [CrossRef] [PubMed] [Google Scholar]
- Tuberculosis of the wrist. Symptoms and outcome in eleven cases. Rev Chir Orthop Reparatrice Appar Mot. 2004;90:337-45.
- [CrossRef] [PubMed] [Google Scholar]




