
Trochantric severity score a useful tool to assess outcomes after intertrochantric fractures
Address for correspondence: Dr. Sandeep Thomas George, Department of Orthopaedics, PSG Hospitals and PSG IMSR, Peelamedu, Coimbatore - 641 004, Tamil Nadu, India. E-mail: sndepgeorge@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: George ST, Rai BK, Mannem A. Trochantric severity score a useful tool to assess outcomes after intertrochantric fractures. J Orthop Allied Sci 2017;5:35-9.
Abstract
INTRODUCTION:
Intertrochanteric fractures (ITF) are of intense interest globally. These fractures are most frequently operated type having the highest postoperative fatality rates and hence have become a serious health resource issue.
AIM:
The aim of this study is to assess the risk factors and their effect on the outcome of intertrochanteric fractures treated by sliding hip screw fixation.
SETTINGS AND DESIGN:
This is a retrospective and prospective observational study of all the intertrochanteric fractures treated by sliding hip screw fixation at our institute between January 2013 to August 2015.
MATERIALS AND METHODS:
A total of 78 intertrochanteric fractures have met the inclusion criteria proposed for the study. Preoperative and intraoperative risk factors were assessed for all the cases and treated by sliding hip screw. The Radiological outcome was assessed after a minimum follow-up of 3 months for all the cases.
RESULTS:
When comparing all the preoperative and intraoperative variables independently with the outcome, P value was found to be statistically significant only in displacement, reverse obliquity, inadequate lateral wall thickness, and reduction. We devised a scoring system to assess the risk outcome in the treatment of trochanteric fractures based on local fracture factors. Least score of zero and a maximum score of eight was seen in the study participants.
CONCLUSION:
Trochantric severity score is a useful tool to assess the outcome of management of intertrochanteric fractures. Sliding hip screw may not be an ideal implant for, trochantric fractures with inadequate lateral wall thickness (failure rate of 63%), reverse oblique type of trochanter fractures (failure rates of 50%), and displaced comminuted fractures (failure rate of 13%).
Keywords
Dynamic hip screw
intertrochanteric fractures
sliding hip screw
trochanteric severity score
unstable intertrochanteric fractures

Introduction
Ninety percent (90%) of intertrochanteric fractures (ITF) occur through osteoporotic bone due to simple fall, whereas in young individuals, it may be a result of high-energy injuries such as motor vehicle accidents or fall from height.[1,2] Though many devices can achieve rigid fixation, the dynamic hip screw is the most commonly used device for intertrochanteric fractures of the femur as it encourages impaction of fracture.[3,4] Unstable intertrochanteric fractures needs to be differentiated from their stable counterparts with regards to treatment plan and prognosis.[5] Risk factors for unstable intertrochanteric fractures include: (1) Loss of medial buttress, (2) Reverse obliquity fractures, (3) Severe comminution, (4) Subtrochantric extension of fracture, (5) Shattered lateral wall (6) Extension into neck area, and (7) Severe osteoporosis (Singh index of <3).[6,7] The treatment of unstable trochantric fractures is more controversial and has got multiple modalities of treatment with no clear cut guidelines.
The purpose of this study was to create a scoring system to assess the risk factors that affect the outcomes of ITF treated by sliding hip screw. In this study, we have followed Evans and AO fracture classification of the intertrochanteric fractures.[8,9]
Materials and Methods
This study included 78 trochantric fractures in 78 consecutive patients, more than 60 years of age, and of either gender. Pathological fractures, infection, neglected fractures, patients medically unfit for surgery, compound fractures associated with vascular injuries, ipsilateral femoral shaft fractures, and pelvic fractures, patients not willing for treatment were excluded from the study.
Local factors such as loss of medial buttress, displacement, reverse obliquity, osteoporosis, comminution at the fracture site, lateral wall thickness were assessed using preoperative radiographs. General medical status was assessed using the American Society of Anesthesiologists grading. Fracture reduction was also assessed using intraoperative and postoperative radiographs. The loss of medial buttress implies that lesser trochanter will be a separate fragment. Displacement is identified radiographically by the loss of contact of any original surface on proximal segment with its corresponding surface on distal segment. Whenever there is <5 mm distance between the fractures fragments it is said as minimally displaced fractures and whenever there is >5 mm gap between any two-fracture fragments it is said as grossly displaced fractures. Reverse obliquity fracture pattern refers to fracture line running from proximal medial to distal lateral instead of the usual pattern. Singh index was used to assess osteoporosis of intact proximal femur. Grade 3 and below were considered osteoporotic bones, and it is identified by thinned trabecular with break in the principal tensile group. More than two fracture fragments around the trochantric region indicated comminution at the fracture site. The presence of comminution at the fracture site is noted on radiographs and scoring was given. Lateral wall thickness is defined as the distance in mm from a reference point below the innominate tubercle of the greater trochanter, angled at 1350 upward to the midpoint between the two cortex lines. Postoperative radiographs assessed reduction by the amount of displacement and neck shaft alignment. The reduction is divided into good, acceptable, and poor. A good reduction had normal/slightly valgus neck shaft angle and displacement of <4 mm. Acceptable reduction met the requirement of either alignment or displacement but not both. Poor reductions met neither criteria.
In this study, all the above variables were assessed with outcome both independently and in combination. Follow up radiographs were taken at a minimum period of 12 weeks and the outcome was assessed. Outcome variables in our study were united with no collapse collapsed but united and fracture failure [Figures 1 and 2].
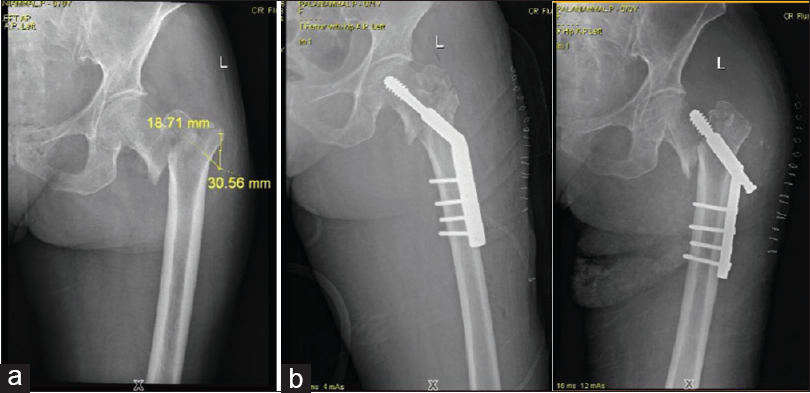
- (a) Preoperative X-ray shows poor lateral wall thickness. (b) Immediate and 15 days postoperative X-rays showing failure

- (a) Radiograph of intertrochanteric fracture which collapsed but united (3 months postoperative). (b) Radiograph of intertrochanteric fracture which united without collapse (>3 months postoperative)
Statistical analysis was performed using unpaired t-test, Chi-square test, and comparison between groups were made using nonparametric Mann Whitney test. The value of P< 0.05 using a two-tailed test was taken as being of significance for all statistical tests.
Results
Seventy-eight patients who met the inclusion and exclusion criteria and were willing and able to participate in this study were enrolled. When comparing the above-mentioned variables independently with the outcome, P value was found to be statistically significant only in displacement, reverse obliquity, inadequate lateral wall thickness and reduction.
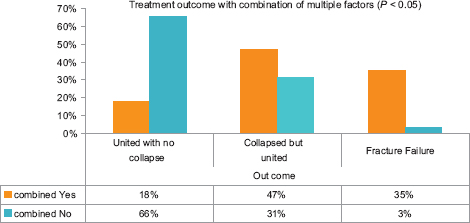
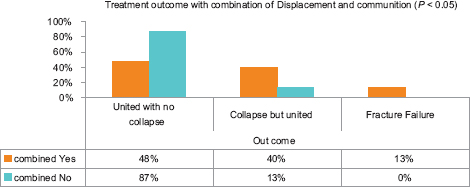
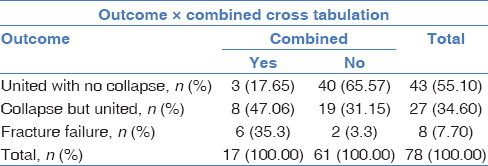
78 patients, 63 patients had combination of displacement and comminution. Of these 63 cases, 30 cases had union without collapse, 25 had union with collapse, and there were 8 fracture failures. The P value was found to be significant (P < 0.05). Of 78 patients, 17 patients had a combination of loss of medial buttress, comminution, displacement and a lateral wall thickness of <20.5 mm. Of these 17 cases, 3 had union without collapse, 8 had union with collapse, and 6 had fracture failure [Tables 1-3].
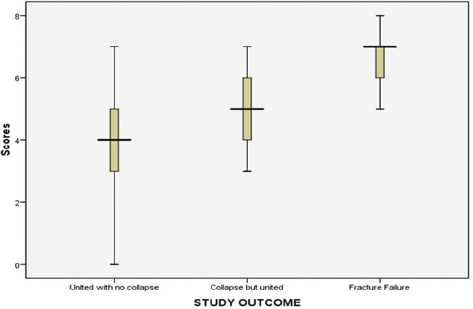
We devised a scoring system to assess the risk outcome in the treatment of trochantric fractures based on local fracture factors. Least score of zero and maximum score of eight was seen in the study participants. A mean score of 3.93 was seen in patients who had union with no collapse, 5.19 in patients who union with collapse and 6.62 in patients who had fracture failure. Out of 24 patients who had a score of ≥6, 25% of patients had union without collapse, 46% of patients had union with collapse and 29% of patients had fracture failure. The P value was found to be significant (P < 0.001) [Table 4].
Discussion
In this study, we have devised a scoring system based on all fracture patterns comparing it with the outcome. The outcome was found to be significant with P< 0.001. Till date, there was no such scoring system designed for preoperative assessment of risk factors in the available literature comparing them with the outcome. According to Evans intertrochanteric fractures are considered stable or unstable depending on the integrity of posteromedial cortex. Fractures with intact posteromedial cortex are considered stable fractures while fractures with loss of posteromedial cortex are considered unstable fractures. Posteromedial cortex constitutes mainly the lesser trochanter.
Of 78 patients, 22 had intact medial buttress and 56 had lost medial buttress. This correlated with the finding of Jacobs et al. that incidence of unstable intertrochanteric fractures is increasing. In this study, we have found that incidence of unstable fractures was 72%.[10] In addition to the incidence of unstable ITF we also compared the loss of medial buttress with the radiological outcome. However in that comparison we have found that P> 0.05. All undisplaced fractures showed perfect anatomical union, minimally displaced fractures showed union with collapse and grossly displaced fractures showed a high incidence of fracture failures (50%). The P value was found to be significant (P < 0.01). The study results in this study were compared with Lichtblau et al. observation on unstable intertrochanteric fractures stating that displacement as one of the risk factors for unstable intertrochanteric fractures.[6] In patients having the reverse oblique type of fracture pattern 38% had fracture failure. Sadowski et al. in their study on treatment of intertrochanteric fractures with reverse oblique fracture pattern, implant failure or nonunion was noted in seven of the nineteen patients (38%) who had been treated with the screw-plate. Only one of the twenty fractures that had been treated with an intramedullary nail did not heal. This supported the use of intramedullary nail rather than the use of blade plate for these fracture pattern.[11] Hence, sliding hip screw is not an ideal implant in treatment of these fractures. In the scenario of comminution at the fracture site, our results were compared with Lichtblau et al. report stating that comminution at the fracture site is one of the risk factors for intertrochanteric fractures but not significantly affecting the outcome. Nearly 29% of patients with inadequate lateral femoral wall had fracture failure in this study. Palm et al. in their study observed that only 3% of 168 patients with an intact lateral femoral wall underwent reoperation within 6 months, whereas 22% of 46 patients with a fractured lateral wall were operated once again. They concluded that patients with preoperative or intraoperative fracture of the lateral wall are not treated adequately with sliding compression screw device.[12] Hsu et al. in their study have observed that 19 of 39 patients with lateral wall fracture (48.7%) had failures. They concluded that fracture classification and lateral wall thickness significantly contributed to postoperative lateral wall fracture. They also concluded that intertrochanteric fractures with lateral wall thickness <20.5 mm should not be treated with sliding hip screw alone.[13] Emrahsahin et al. compared the quality of fracture reduction between intramedullary and extramedullary implants and they have observed not much of statistical difference (P = 0.83). In this study, we have compared the fracture reduction with radiological outcome and we have observed that fracture failures are more commonly seen in fractures with poor reduction. The P value was found to be significant (P < 0.05). In the study by Baumgaertner and Solbergon tip apex distance (TAD), they have observed that the mean TAD was 20 mm in the study group and 25 mm in control group. They also observed that there were no cut-out failures in 118 fractures of study group at a mean follow-up of 8 months compared with 16 of 198 in the control group.[14]
In this study, we compared the combination of displacement and comminution with the outcome. We observed that 100% of patients with fracture failure had a combination of these two factors. From this observation, combination of these two variables had a significant affect on the outcome. No studies were carried out comparing these two variables with the outcome. Of 78 patients, 17 patients had a combination of all these factors. In 17 patients, 6 had fracture failure (35.3%), 8 had union with collapse, and 3 had an anatomical union. From the above results, we also state that combination of multiple factors had fracture failures and nonanatomical union.
Conclusion
The trochantric severity score is a useful tool to assess the outcome of management of intertrochanteric fractures. A score of <4 showed very good results when treated with sliding hip screw. The sliding hip screw is still a good implant for the majority of intertrochanteric fractures provided they do not fall in the higher severity score group. Sliding hip screw may not be an ideal implant for, trochantric fractures with inadequate lateral wall thickness (failure rate of 63%), reverse oblique type of trochanter fractures (failure rates of 50%), and displaced comminuted fractures (failure rate of 13%).
Clinical significance
Trochantric severity score helps to grade patients with intertrochanteric fractures to plan the type of fixation and to give the best outcomes after surgery.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Rockwood and Green's Fractures in Adults. Philadelphia: Lippincott Williams & Wilkins; 2006.
- [Google Scholar]
- The stability of intertrochanteric fractures treated with a sliding screw-plate. J Bone Joint Surg Br. 1990;72:37-40.
- [Google Scholar]
- Potentially unstable intertrochanteric fractures. J Orthop Trauma. 2005;19:5-9.
- [CrossRef] [PubMed] [Google Scholar]
- The unstable intertrochanteric hip fracture. Orthopedics. 2008;31:792-7.
- [CrossRef] [PubMed] [Google Scholar]
- The treatment of trochanteric fractures of femur. J Bone Joint Surg. 1949;191:53-63.
- [Google Scholar]
- The Comprehensive Classification of Fractures of Long Bones. Berlin: Springer; 1990.
- [CrossRef] [Google Scholar]
- Internal fixation of intertrochanteric hip fractures: A clinical and biomechanical study. Clin Orthop Relat Res. 1980;146:62-70.
- [Google Scholar]
- Treatment of reverse oblique and transverse intertrochanteric fractures with use of an intramedullary nail or a 95 degrees screw-plate: A prospective, randomized study. J Bone Joint Surg Am 2002:372-81.:84-81.
- [CrossRef] [Google Scholar]
- Integrity of the lateral femoral wall in intertrochanteric hip fractures: An important predictor of a reoperation. J Bone Joint Surg Am. 2007;89:470-5.
- [CrossRef] [PubMed] [Google Scholar]
- Lateral femoral wall thickness. A reliable predictor of post-operative lateral wall fracture in intertrochanteric fractures. Bone Joint J 2013:1134-8.:95-8.
- [CrossRef] [PubMed] [Google Scholar]
- Awareness of tip-apex distance reduces failure of fixation of trochanteric fractures of the hip. J Bone Joint Surg Br. 1997;79:969-71.
- [CrossRef] [PubMed] [Google Scholar]




