
Translate this page into:
Management of clubfoot by ponseti method: A prospective study
Address for correspondence: Dr. Akshat Vijay, Department of Orthopedics, Jhalawar Medical College, Jhalawar, Rajasthan, India. E-mail: akshat.vijay15@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Saini MK, Vijay A, Gupta M, Harshwardhan H. Management of clubfoot by ponseti method: A prospective study. J Orthop Allied Sci 2017;5:27-34.
Abstract
INTRODUCTION AND AIM:
Clubfoot is usually diagnosed immediately after birth; hence, most of the surgeons believes in an early initiation of treatment. Thus, our study was aimed to assess the efficacy of Ponseti technique in correcting congenital talipes equinovarus deformity of foot, to determine the type of clubfoot best suited for this technique and to find the lacunae and disadvantages of Ponseti technique, if any.
MATERIALS AND METHODS:
It was a prospective study of 50 cases with 76 feet of clubfoot in tertiary level hospital from September 2012 to October 2016. All these cases included were classical clubfoot deformities (idiopathic clubfoot), excluding syndromic and complicated cases with previous failed operative treatment. Children were evaluated by Pirani severity scoring system. All the patients were treated by Ponseti technique of corrective casting and achilles tenotomy.
RESULTS:
In the present study, about 84% of patients had good results, 4% had fair results, and 12% of patients had poor results showing failure with Ponseti technique. Overall, 88% of the patients presented with satisfactory results. Overall, mean Pirani score for all the feet was 5.01. There were thirty complications among all the patients, constituting 39% of total feet.
CONCLUSION:
The observations of the present study clearly showed that age at initial presentation, quality (mobility) of foot and Pirani score at presentation directly affects final results. Ponseti technique for the treatment of clubfoot is a simple and effective which is suitable in the Indian subcontinent as it is economical.
Keywords
Clubfoot
Pirani score
Ponseti technique

Introduction
Clubfoot, also termed congenital talipes equinovarus (CTEV), is a congenital deformity involving one foot or both. It is occurring in about one in every 1000 live births. Clubfoot is not an embryonic malformation. A normally developing foot turns into a clubfoot during the second trimester of pregnancy. Therefore, such as developmental hip dysplasia and idiopathic scoliosis, clubfoot is a developmental deformation.[1] In 1950, Ignacio Ponseti, at the University of Lowa, developed a method of treating clubfoot by serial manipulation, a different technique of cast application and a possible percutaneous achilles tenotomy. The clinical correction achieved using this method has produced a functional, plantigrade foot without requiring posteromedial release in 85%–90% of cases.[2-4] The unsatisfactory results associated with complete soft tissue releases at 10–15 years of follow-up[5,6] and good to excellent results by Ponseti technique reported by many authors[6-9] encouraged us to study the subject. Thus, our study was aimed to assess the efficacy of Ponseti technique in correcting CTEV deformity of foot, to determine the type of clubfoot best suited for this technique, and to find the lacunae and disadvantages of Ponseti technique, if any.
Materials and Methods
The present study was a prospective study of 50 cases with 76 feet of clubfoot in tertiary level hospital from September 2012 to October 2016. All these cases were having classical clubfoot deformities (idiopathic clubfoot); cases which had other antecedent causes (syndromic cases) such as arthrogryposis multiplex congenita, spina bifida, cerebral palsy, and poliomyelitis and cases with earlier failed operative treatment were also excluded from this study. Permission was obtained from the Ethical Committee in accordance with 1975, Declaration of Helsinki before starting the study. Written consent was obtained from all the patients before starting treatment.
A complete and detailed antenatal, natal, and postnatal history of mother was taken to find any eventful condition during or after pregnancy. Family history for clubfoot and other congenital diseases was also inquired. Each patient was subjected thorough general, physical, and systemic examination including spine, hip, and extremities. After taking complete history, mobility of foot was assessed by applying gentle corrective manipulation. Foot was classified into supple type if manual reduction was possible and rigid type, where manual reduction was impossible.
Children were evaluated for severity of clubfoot by Pirani severity scoring system[1,10,11] which registers the deformity of six different components of the clubfoot. It comprises two scores midfoot score (MS; including three components, namely, curvature of lateral border of foot, medial crease, and lateral part of the head of the Talus) and hindfoot score (HS; including three components, namely, posterior crease, empty heel, rigid equinus). Each component was given a score of 0 (normal), 0.5 (moderately abnormal), or 1.0 (several abnormal) depending on severity. The congenital clubfoot undergoing treatment was assessed at each visit (weekly) and assigned:
A MS of up to 3 (0 = normal, 3 = severe deformity)
A HS of up to 3 (0 = normal, 3 = severe deformity)
A total score (TS) of up to 6 (0 = normal, 6 = severe deformity).
The feet were then classified into three groups with respect to the severity of the deformity on the basis of initial Pirani score.
Group I - Feet with a Pirani score of 1.5–2.5 points
Group II - Feet with a Pirani score of 3–4.5 points
Group III - Feet with a Pirani score of 5 points or more.
Consequently, the TS was from 0 to 6 points, with 6 representing the most severe deformity. The scores were plotted on a graph to know how the foot was recovering on the treatment. The Ponseti technique[1,2] was used at our institution according to the following regimen.
Treatment was started as soon as possible after birth and consisted of gentle manipulation of the foot and the serial application of long leg plaster casts without the use of anesthesia as described by Ponseti. The same method was also applied to older children (up to 14 months of age) who were referred to us for the first time or in those who have had previous unsuccessful nonoperative treatment elsewhere.
In all the patients, cavus was rectified first by supinating the forefoot and dorsiflexing the first metatarsal. Failure to supinate the forefoot as the first step ultimately leads to incomplete correction of the clubfoot. To correct the varus and adduction, supinated foot was abducted while counter pressure was applied with the thumb against the head of the talus. The patients were asked for weekly visits with continuous mobilization and casting at each visit, and simultaneous correction of the cavus, adduction, and heel varus deformity. The heel was never forcibly everted while the calcaneus was locked under the talus because this would have caused a breach in the midfoot and resulted in a bean-shaped foot.[2] During mobilization and casting, the talus was fixed in the ankle mortise by firm pressure on the lateral aspect of the talar head while the foot under the talus was abducted. When full abduction of the foot on the talus was achieved, and all other deformities were corrected, the equinus was corrected by percutaneous achilles tenotomy or by casting. Percutaneous tenotomy of the achilles tendon was performed when:
Residual equinus was observed, i.e. after the abduction of the foot and the varus deformity of the heel has been corrected
Last 15° of dorsiflexion has not been obtained with the use of casts
When HS >1, MS >1, the head of the talus was covered.
We performed the tenotomy in the Indoor Plaster Room without any anesthesia, which allowed easy feel of achilles tendon and no risk of drug allergy complication to the patients. This approach differs from that of Ponseti,[2] Colburn and Williams,[12] Morcuende et al.[13] and Herzenberg et al.,[14] who prefer that the achilles tenotomy be done in the clinic with a topical and/or local anesthetic.
After painting and draping with full aseptic precaution, a number 15 surgical knife was introduced through the skin onto medial edge of the tendon achilles about 1 cm above its calcaneal insertion. The cutting surface of the blade should point proximally at this stage. The tendon was felt with the tip of the knife, and care was taken not to spear it. The knife was introduced in front of the tendon and then rotated 90°, which allowed the tendon to be severed from front to back. A “pop” was felt as the tendon was released. An additional 20°–25° of dorsiflexion was typically gained after the tenotomy, and the equinus deformity was corrected.[1,15] After the tenotomy, an additional cast was applied with the foot abducted 60°–70° for 3 weeks which was crucial in obtaining complete correction and in helping to prevent early recurrence. After 3 weeks, the cast was removed [Figures 1-10].

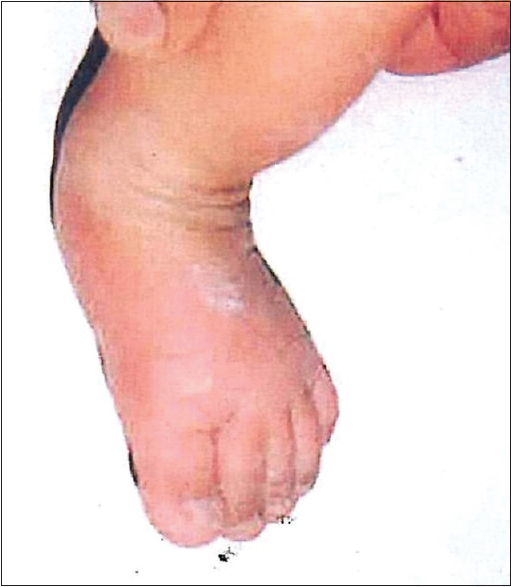
- At initial presentation

- After first cast application
- Right foot after second cast application

- Left foot after second cast application
- Right and left foot after third cast application
- Both feet after fourth cast application

- After percutaneous tendo-achilles tenotomy (right Foot)
- After percutaneous tendo-achilles tenotomy (left foot)

- Right foot after final correction
- Left foot after final correction
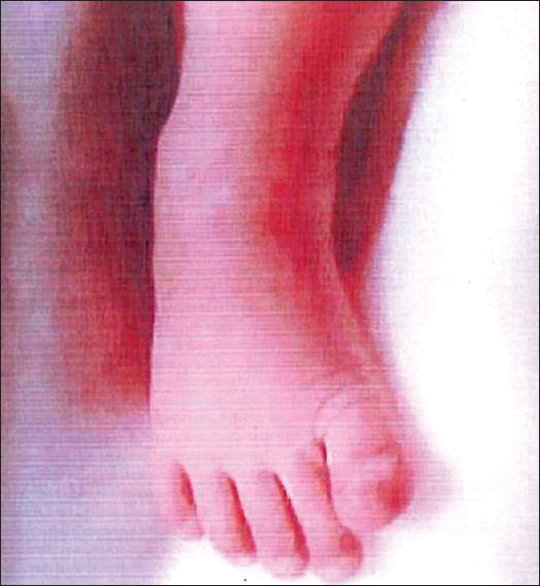
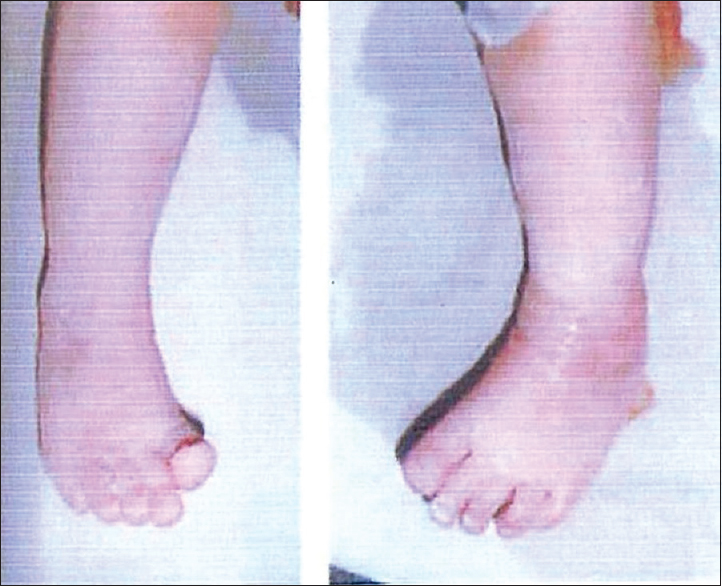
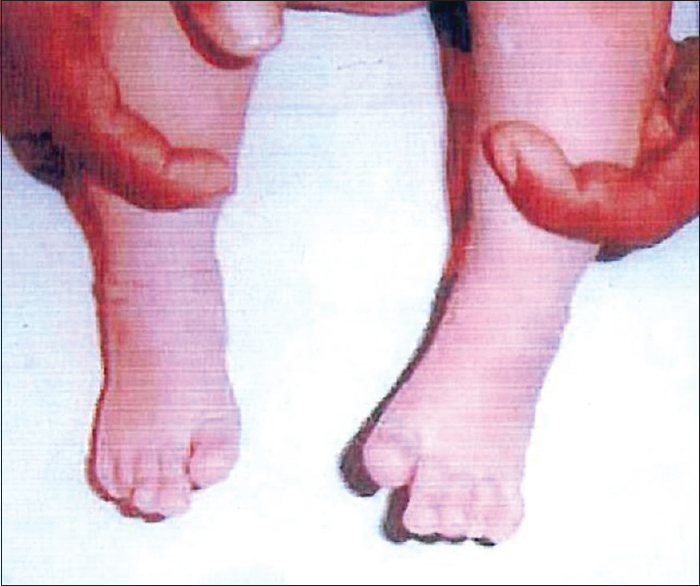
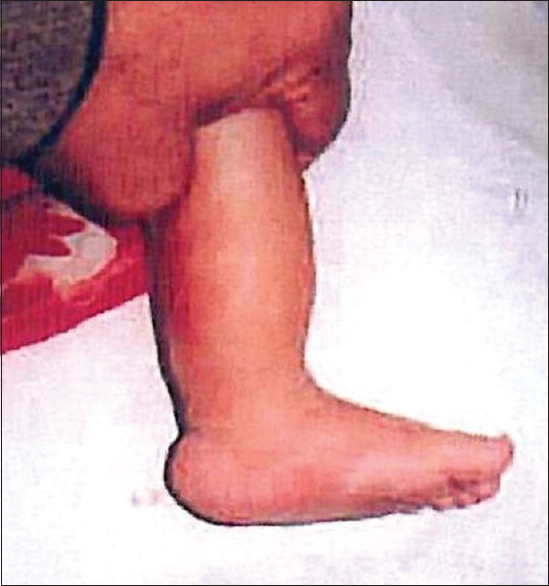
Follow-up [Figures 11-16]; after the last cast was removed and once all deformities were corrected, the patients were given foot abduction brace (FAB) [Figure 11]. The FAB preserved the corrected foot in 70° of external rotation with ankle in dorsiflexion which was accomplished by bending the bar with the convexity of the bar distally directed. If the deformity was unilateral, the normal foot was placed in 40° of external rotation. Patients were given FAB for 23 h a day for the first 3 months and then gradually decreased to 12 h a day till 2 years.[12,13,16] To prevent recurrence of equinus deformity, the parents were instructed about range-of-motion exercise for the ankle when it was out of the brace. These exercises maintained the ankle motion achieved at the time of the tenotomy.[16] Patients were assessed every 15 days until the age of 6 months, and then every month, after initial completion of treatment to boost parental compliance to FAB and to assess maintenance of correction. Patients were regularly checked for relapse if any. If relapse was observed at follow-up, patients were again kept for Ponseti regimen. Achilles tendon tenotomy was repeated when dorsiflexion of the ankle was <15° for up to 12 months of age; thereafter, the tendon lengthening was done through an open approach and was usually accompanied by a posterior release of the ankle and subtalar joint.

- After full correction, foot abduction brace was applied with external rotation of 70° in both feet

- At 12 months follow-up, patient in the standing position (front)

- At 12 months follow-up, patient in standing position (back)

- At 12 months follow-up, the left foot as seen from side

- At 12 months follow-up, the right foot as seen from side

- At 12 months follow-up, patient in the squatting position
Final grading of the patients was done into good, fair, and poor results.
Good results: Patients were labeled as having a good result if Pirani score is 1.5 points or less or if all deformities get corrected by Ponseti technique alone at final follow-up
Fair results: Patients were labeled as having a fair result if additional surgical procedures, such as tendon lengthening through an open approach or a posterior release of the ankle and subtalar joint were done to get correction
Poor results: Patients were labeled as having a poor result, if Ponseti technique failed to give complete correction of foot even once.
Results
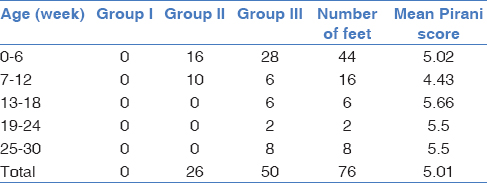
In this study, there were 50 children (76 feet) of idiopathic clubfoot deformity, treated by Ponseti technique. Most of the children were below 6 week of age. The youngest patient in the series was of 3 weeks, whereas the oldest was of 26 weeks. Treatment was initiated at mean age of 9.08 weeks (range, 3–26 weeks). 72% of the children were male. The male to female ratio in the series was 2.5:1. Twenty-four patients (48%) had unilateral while 26 (52%) had bilateral foot involvement; however, the right side was found to be more commonly involved (52%) than the left (48%) in cases with unilateral foot involvement. Sixty-six percent feet were supple, and 34% were rigid at the time of initial presentation. Feet were divided into three groups as per Pirani scoring system. No foot (0%) fall into Group I category while 26 feet (34%) had scores of Group II and III had the maximum number of feet 50 (66%). Feet classified into Group II and III had mean Pirani score of 4.13 and 5.42, respectively. Overall, mean Pirani score for all the feet was 5.01. Mean Pirani score for male and female feet was 5.08 and 4.75, respectively. It was also found that mean Pirani score of supple and rigid feet were 4.76 and 5.5, respectively. The majority of the patients presenting at an early age had supple foot with mild to moderate deformity and low Pirani scores; while in those presenting late, rigid variety of foot was more common with severe deformity and high scores [Table 1].
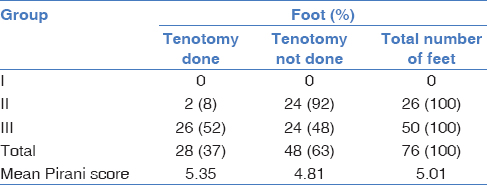
The incidence of tenotomy was less in patients presenting at an early age as compared to patients with late initial presentation. Mean age of tenotomy done was 11.4 weeks which was higher than those in nontenotomy group 7.21 weeks. More than three-fourth patients with rigid clubfoot required tenotomy as compared to supple foot; in which, only 20% of the feet required it. In four feet of rigid feet group, posteromedial soft tissue release (PMSTR) was required. In Group II, 2 feet (8%) underwent percutaneous tenotomy while in Group III, 26 feet (52%) required it. Total of 28 (37%) of the 76 clubfeet underwent a percutaneous achilles tenotomy to correct a residual equinus deformity. Mean Pirani score of tenotomy feet was 5.35 as compared to 4.81 of nontenotomy feet [Table 2].
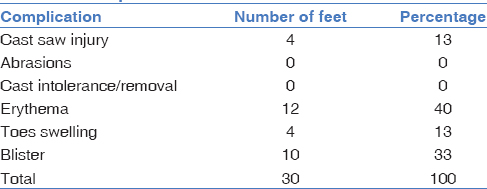
The mean number of casts required to obtain correction was 7.7 (range, 5–10 casts). The more severe the initial deformity (higher Pirani score), the more number of casts were required to obtain correction. Forty-four patients (88%) under treatment showed good compliance while 6 patients (12%) were noncomplaint with FAB. All four patients which had recurrence of the deformity belong to the noncompliant group. Relapses were treated with a second series of manipulation and casting, followed by the use of the FAB. There were thirty complications among all the patients, constituting 39% of total feet. Majority of complications were minor erythema (40%) seen in young neonates that may be due to soft skin [Table 3].
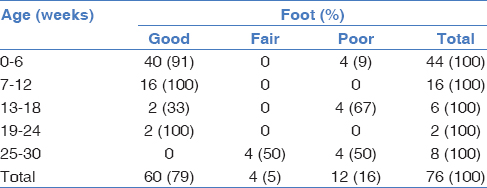
In the present study, about 84% of patients had good results, 4% had fair results, and 12% of patients had poor results showing failure with Ponseti technique. Overall, 88% of the patients presented with satisfactory results. None of the supple foods required extensive surgery such as PMSTR to correct the deformity while approximately 36% of the rigid foot required PMSTR showing poor results with Ponseti technique. Among patients presenting within the first 6 weeks of age, 91% of the patients were having good results [Table 4].
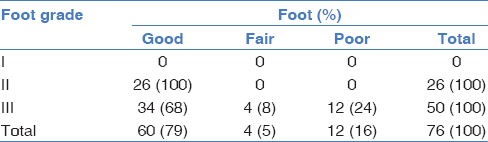
In Group II, none of the patients required any extensive surgery to correct clubfoot deformity. Although 68% of the patients under Group III also claimed good result; however, 24% patients had poor results [Table 5].
Discussion
Understanding the pathomechanics and treating clubfoot successfully has always been unsolved mystery for modern medicine. In the present study, the Ponseti technique was followed for the correction of clubfoot. It was fundamentally different from Kite's maneuver[17] in a way that cavus was corrected first by supinating the forefoot and dorsiflexing the first metatarsal. During entire process, the forefoot was kept in supination as the primary deformity in clubfoot is drop of the first metacarpal and pronation of forefoot.[3,18] This maneuver is against the earlier maneuver by Kite's serial casting[18] where the forefoot was abducted at midtarsal joint against pressure at calcaneocuboid joint and in pronation. Ponseti called this maneuver “Kite's error” because it blocks the correction of hindfoot varus and internal rotation.
In our study, the mean age at initial presentation of 9.08 weeks which was in agreement with age incidence observed by Dobbs et al.[16] and Lehman et al.[19] Presenting age at initial presentation has a direct bearing on quality (mobility) of foot, Pirani score, the need of tenotomy and final results. Similar finding was reported by Lehman et al.[19] and Morcuende et al.[13] where they have stressed the importance of initiating treatment at an early age. In the present study, 72% patients (18 patients) treated were males, and 28% percent (7 patients) were females. The male to female ratio was 2.5:1 similar to other studies.[13,16,20] In the present study, maximum number of patients fall into Group III of Pirani scoring system with Overall, means Pirani score of 5.0. Similarly, mean Pirani score of 4.6 was noted by Lehman et al.[19]
The indication for tenotomy has been clearly described and is reported to be necessary in approximately 44% patients. Tenotomy of the achilles tendon was an integral part of Ponseti technique.[3,4,9] We preferred to perform the tenotomy in the indoor plaster room without anesthesia. This approach differs from that of Ponseti,[2] Colburn and Williams,[12] Morcuende et al.[13] and Herzenberg et al.,[14] who prefer that the achilles tenotomy be done in the clinic with a topical or local anesthesia. A total of 28 (37%) of the 76 clubfeet underwent a percutaneous achilles tenotomy to correct a residual equines deformity. Similar results were seen in study by Lehman et al.[19] while high preponderance of percutaneous tenotomy was observed in other studies.[13,14,16] Results of the present study showed that there was a direct correlation between the increase incidence of tenotomy with higher Pirani score, with increased rigidity of clubfoot and with higher age at presentation. The present study revealed that the need for a tenotomy can be predicted at the initiation of treatment fairly and accurately. In addition, the rigidity of the foot, and not just the overall severity of the initial equinus, is an important factor in predicting the need for a tenotomy. Thus, the Pirani score was a good prognostic indicator, which renders the objectivity of clubfoot treatment.
In the present study, the mean number of casts required to obtain correction in Group I, II, and III were 0, 7.4 and 8, respectively with an overall mean of 7.7. These results were quite similar to Laaveg and Ponseti[3] and Herzenberg et al.[14] series. However, less number of casts is required by other studies.[16,19,21]
After completion of the casting regimen, the feet were placed in foot abduction brace to maintain the correction. Families of six children (12%) complained that they had not complied with use of the FAB. A similar observation regarding noncompliance was observed by Lehman et al.[19] and Morcuende et al.[13] The most common reason for noncompliance was inconvenience, which was maximum in the first 3 months of FAB prescription. In the present series, 8% of the patients reported relapses after initial successful treatment; these relapses were significantly associated with noncompliance with the FAB. Ponseti[22] has reported a relapse rate of 78% in patients noncompliant with the FAB and a relapse rate of 7% in compliant patients. We speculate that the tendency to relapse may be caused by the intrinsic contractile nature of the soft tissue in clubfoot deformity as postulated by Ponseti,[2] Fukuhara et al.[23] and Zimny et al.[24] Our results and those of Ponseti suggested that the importance of maintaining correction with the FAB is paramount to successful treatment.
There were 30 minor complications among all the casting performed constituting 39% of total feet. No infections, skin necrosis, neurovascular compromise, or bleeding were observed even in posttenotomy period. Other studies[13,15,19] also mentioned similar complications.
In our study, 88% patients had satisfactory outcomes (good to fair) by sequential casting alone with or without tenotomy. However, out of remaining six feet having poor results, in four a formal posteromedial surgical release was required as full correction was never obtained. Other studies[7,13,14] also proposed similar results.
The observations of the present study clearly showed that age at initial presentation, quality (mobility) of foot, and Pirani score at presentation directly affects final results.
Conclusion
Ponseti technique for treatment of clubfoot is simple, effective, noninvasive, nonoperative and economical procedure, which is suitable in the Indian subcontinent as it is economical. The Ponseti technique also provides flexibility to recast patients who lose correction and salvaging patients with poor outcomes by recasting with tenotomy.
Financial support and sponsorship
Nil.
Acknowledgments
We are grateful to Dr. Nand Lal Jhamaria and Dr. Devkant for their help in conducting the study and preparation of the manuscript.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Editor- Staheli L: Club foot: Ponsetti Management. Vol 3. (2nd). Global Help Publication; 2005. p. :4.
- [Google Scholar]
- Congenital Clubfoot: Fundamentals of Treatment. New York: Oxford University Press; 1996.
- [Google Scholar]
- Long-term results of treatment of congenital club foot. J Bone Joint Surg Am. 1980;62:23-31.
- [CrossRef] [Google Scholar]
- Treatment of congenital club foot. J Bone Joint Surg Am. 1992;74:448-54.
- [CrossRef] [Google Scholar]
- Resistant congenital club foot – One-stage posteromedial release with internal fixation. A follow-up report of a fifteen-year experience. J Bone Joint Surg Am. 1979;61:805-14.
- [CrossRef] [Google Scholar]
- Long-term results of early surgical release in club feet. J Bone Joint Surg Br. 1985;67:791-9.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term comparative results in patients with congenital clubfoot treated with two different protocols. J Bone Joint Surg Am 2003:1286-94.:85-94.
- [CrossRef] [PubMed] [Google Scholar]
- Experience in the conservative treatment of congenital clubfoot in newborns and infants. J Pediatr Orthop. 1989;9:134-6.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of idiopathic clubfoot. A thirty-year follow-up note. J Bone Joint Surg Am. 1995;77:1477-89.
- [CrossRef] [PubMed] [Google Scholar]
- A Method of Evaluating the Virgin Club Foot with Substantial Interobserver Reliability. Presented at the Annual Meeting of Pediatric Orthopedic Society of North America, Miami; 1995
- [Google Scholar]
- An independent assessment of two clubfoot-classification systems. J Pediatr Orthop. 1998;18:323-7.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of the treatment of idiopathic clubfoot by using the Ponseti method. J Foot Ankle Surg. 2003;42:259-67.
- [CrossRef] [PubMed] [Google Scholar]
- Radical reduction in the rate of extensive corrective surgery for clubfoot using the Ponseti method. J Pediatr Orthop. 2003;23:780-7.
- [Google Scholar]
- Ponseti versus traditional methods of casting for idiopathic clubfoot. J Pediatr Orthop. 2002;22:517-21.
- [CrossRef] [PubMed] [Google Scholar]
- Bleeding complications following percutaneous tendoachilles tenotomy in the treatment of clubfoot deformity. J Pediatr Orthop. 2004;24:353-7.
- [CrossRef] [PubMed] [Google Scholar]
- Factors predictive of outcome after use of the Ponseti method for the treatment of idiopathic clubfeet. J Bone Joint Surg Am 2004:22-7.:86-7.
- [CrossRef] [PubMed] [Google Scholar]
- Congenital clubfoot: The results of treatment. J Bone Joint Surg 1963:261-75.:45-75.
- [CrossRef] [Google Scholar]
- A method for the early evaluation of the Ponseti (Iowa) technique for the treatment of idiopathic clubfoot. J Pediatr Orthop B. 2003;12:133-40.
- [CrossRef] [Google Scholar]
- Predicting the need for tenotomy in the Ponseti method for correction of clubfeet. J Pediatr Orthop. 2004;24:349-52.
- [CrossRef] [PubMed] [Google Scholar]
- Relapsing clubfoot: Causes, prevention, and treatment. Iowa Orthop J. 2002;22:55-6.
- [Google Scholar]
- The pathogenesis of club foot. A histomorphometric and immunohistochemical study of fetuses. J Bone Joint Surg Br. 1994;76:450-7.
- [CrossRef] [Google Scholar]
- An electron microscopic study of the fascia from the medial and lateral sides of clubfoot. J Pediatr Orthop. 1985;5:577-81.
- [CrossRef] [PubMed] [Google Scholar]




