
Translate this page into:
Wakeboard accident, avulsion adductor longus
Address for correspondence: Dr. Dieter Hesch, Mövenweg 87, Ch 8597 Landschlacht, Germany. E-mail: dieter@hesch.ch
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Hesch D. Wakeboard accident, avulsion adductor longus. J Orthop Allied Sci 2018;6:97-8.
Sir,
I would like to share this rare case of a complete avulsion of adductor longus and sartorius muscle at the same time occurring on a wakeboarder.
Complete avulsion of the adductor longus muscle is uncommon in general, but it has been described in soccer, football, hockey, one case of skiing and horse riding.[1,2] The rider reported herein is an experienced wakeboarder, performing the sport since 25 years. He started from the regular position, left foot in front and legs deeply bended. Immediately after acceleration of the boat by the driver, he experienced popping and extreme pain in the left groin and suprapubic area.
Critical conditions at the wakeboard start are weight and training state of the rider (in this case, 169 cm and 69 kg, well trained) tension of the rope at the start, position and bending of legs on board. We can only speculate about the cause of the accident, but retrospectively an unusual acceleration speed of the boat with abrupt load on the rope and rider may have added possibly to the accident.
Clinical
The clinical course was similar to most other cases but nearly identical in all aspects to the case reported by Lands et al.[2] The rider was brought on land, he presented with heavy pain as described. A medical investigation including palpation of inner thigh, groin, and suprapubic area was painful due to tissue damage and accompanying swelling. Passive abduction and adduction at this time were merely impossible, but the rider could walk with pain a few meter. For 2 days he rested.
Diagnostic
On day 4 after the injury an ultrasonography [Figure 1] was performed and on day 5 a magnetic resonance imaging, [Figure 2a and b].
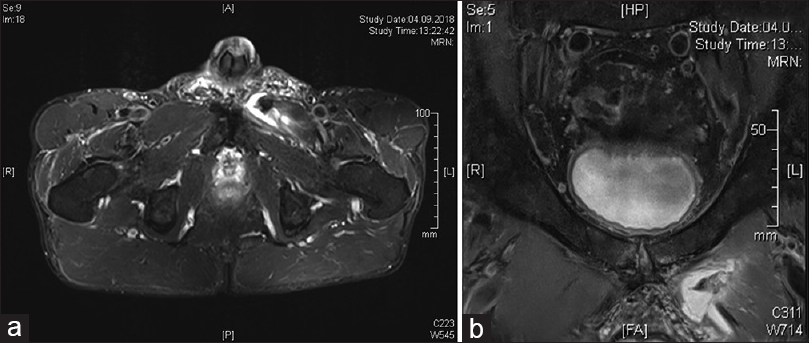
- (a and b) Magnetic resonance imaging transversal showing complete osseous avulsion of adductor longus muscle, retraction 8 mm, hematoma
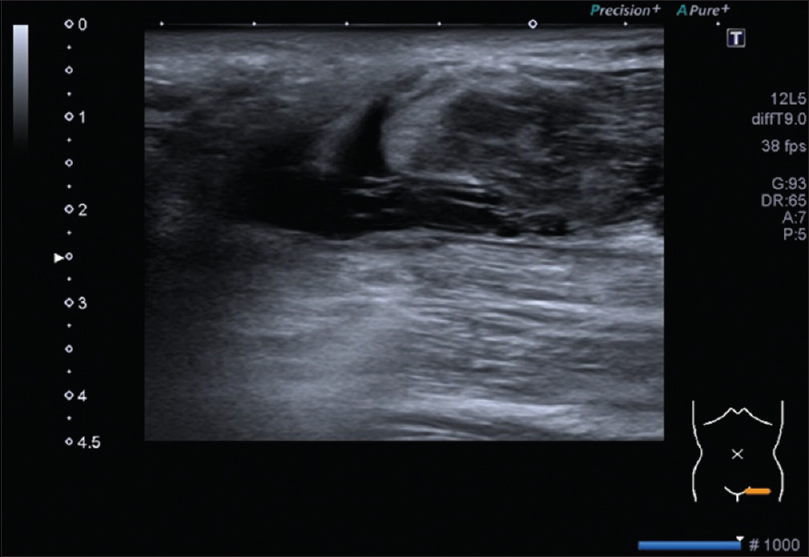
- Ultrasonography: Complete avulsion of adductor longus muscle, retracted muscle, hematoma
Both imaging modalities showed a complete avulsion of the adductor longus and sartorius muscle with retraction of the adductor longus tendon and muscle of about 8 mm from the pubic bone. Hematoma had developed rapidly and progressed over 5 days down to popliteal fossa.
Therapy
The rider, after informed consent with experts, decided to apply conservative treatment, mainly because he learned that rehabilitation was a favorable option.
Since part of the pain was considered as consequence of inflammation a systemic treatment with prednisone was initiated (40 mg over 5 days, 20 mg over 5 days, and 10 mg for another 5 days). A general reduction of pain was noted 2 days after starting prednisone. The large cutaneous hematoma was treated with Hemoclar over 10 days. The swollen area left groin probably also due to the retracted muscle shrank satisfactorily, and most inner hematoma were resorbed after 12 days by inspection and palpation.
Rehabilitation exercises were started at day on day 5 after the accident consisting of physiotherapy following consultation with and personal advise by Thorborg et al., University of Copenhagen[3] following the program published by Hölmich et al.[4] and intensified using TheraBand.
Only 2 days after initiation of this program general daily complaints vanished. On day 17, the rider was nearly free of pain during daily life and when performing the exercise program. Muscular exercises were intensified at day 18 using an adductor weight training machine (Techno Gym) starting with 2o kg.
Based on the mentioned literature a complete regeneration could be expected after 6–10 weeks with a return to board sports and this was the achieved also in this case.
Thorborg, in his consulting, supposed that the avulsed muscle and his tendon may possibly find its way back.
Conclusion
In summary, a conservative treatment of a completely avulsed adductor longus muscle as first here described on a wakeboarder, seems favorable over operative interventions, using an intense accelerated rehabilitation program. Early prednisone therapy, not reported so far, may be a valuable and effective intervention for pain and inflammation reduction with less risk than using nonsteroidal drugs which may intensify bleeding risk and hematoma forming.
Financial support and sponsorship
Nil.
Acknowledgment
The author would like to thank Dr. Denis Wetter, Radiology, Kantonsspital, CH-8596 Muensterlingen for performing ultrasound and magnetic resonance imaging studies.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- A rare case of adductor longus muscle rupture. Case Rep Orthop. 2015;2015:840540..
- [CrossRef] [PubMed] [Google Scholar]
- Complete avulsion of the adductor longus in a semi-professional football player: Rapid return to play with nonoperative treatment. J Orthop Allied Sci. 2016;4:45-8.
- [CrossRef] [Google Scholar]
- Clinical recovery of two hip adductor longus ruptures: A case-report of a soccer player. BMC Res Notes. 2013;6:205..
- [Google Scholar]
- Effectiveness of active physical training as treatment for long-standing adductor-related groin pain in athletes: Randomised trial. Lancet. 1999;353:439-43.
- [CrossRef] [PubMed] [Google Scholar]




