
Translate this page into:
Tuberculous spine infection and metal instrumentation
 , Pradip Patil2, Umesh Dhanraj Jain2, Salim Lad2,, Amol Gowaikar2, Suraj Deshmukh2
, Pradip Patil2, Umesh Dhanraj Jain2, Salim Lad2,, Amol Gowaikar2, Suraj Deshmukh2
*Corresponding author: Salim Lad, Department of Orthopaedics, D. Y. Patil Medical College, Kolhapur, Maharashtra, India drslad283@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Ghate UV, Patil P, Jain UD, Lad S, Gowaikar A, Deshmukh S. Tuberculous spine infection and metal instrumentation. J Orthop Spine. 2025;12:2. doi:10.25259/Joasp_29_23
Abstract
Objectives
The aim of this study was to investigate the impact of tuberculous infection on metal implants in the spine. Spinal infections include a wide range of illnesses such as discitis, Vertebral osteomyelitis, and spinal epidural abscess. With more advanced surgical methods and diagnostic equipment becoming available, the treatment of spinal infections is changing. Magnetic resonance imaging (MRI) with contrast is the ideal imaging test. Computed tomography-guided biopsy is necessary for choosing antibiotics. Patients with neurological deficit, marked spinal ligamentous instability due to infection, and those who have not improved without surgery are subjected to surgical debridement and metal instrumentation. The cornerstone of therapy is the use of anti-Koch’s drugs.
Materials and Methods
This study is described as a retrospective observational study. This means that it involves the analysis of data collected from past cases rather than a controlled experiment. It appears that the study aimed to analyse the outcomes and effectiveness of the treatment approach (posterior instrumentation and transpeduncular debridement) for spinal tuberculosis in these ten patients. If you have any specific questions or need more information about this study, please feel free to ask.
Results
We found that despite having active infection on surgical time in case of tubercular mycobacterium no significant complication regarding implants such as implant loosening, breakage, worsening of symptoms after instrumentation, surgical site infection and re-surgery were noted.
Conclusion
A wide range of illnesses, including discitis, Vertebral osteomyelitis, and sub epidural abscess, are classified as spine infections. Staphylococcus aureus is the most frequent cause of pyogenic spine infection, whereas Mycobacterium tuberculosis is the most frequent cause of granulomatous infectious disease. The optimum surgical strategy depends on the site, the degree of the infection, and the degree of spine instability.
Keywords
Implants
Spine infection
Tuberculosis

INTRODUCTION
A wide range of illnesses, including discitis, Vertebral osteomyelitis, and spinal epidural abscess, fall within the category of spinal infections.1 As more cutting-edge surgical methods and diagnostic equipment become accessible, the treatment of spinal infections is changing. The ideal imaging test is magnetic resonance imaging (MRI) with contrast. Computed tomography-guided biopsy is necessary for choosing antibiotics. Patients with neurological deficit, marked spinal ligamentous instability due to infection, and those who have not improved without surgery are subjected to surgical debridement and metal instrumentation. The cornerstone of therapy is the use of anti-Koch’s drugs.2
Spinal tuberculosis
The most frequent cause of spinal granulomatous infection is Mycobacterium tuberculosis. 10–20% of tuberculosis (TB) patients in industrialised countries and up to 20–41% in underdeveloped countries had vertebral granulomatous infections. Commonly,3,4 from the metaphyseal regions of the vertebral body anteriorly.1 Behind the anterior longitudinal ligament, and cranial-caudally, a tubercular infection spread.1 The spread could be irregular, resulting in paravertebral abscesses and skip lesions. Additionally, it has been discovered that an immunocompromised state raises the frequency of musculoskeletal lesions. While musculoskeletal lesions occur in 3–5% of individuals with pulmonary TB, they occur in approximately 60% of people with Human Immuno Deficiency Virus. Spinal tuberculosis exhibits a higher propensity for thoracic spine involvement, deformity, and substantial neurologic impairments than does pyogenic spinal infections.
MATERIAL and METHODS
Study setting
Between July 2020 and June 2023 ten Patients underwent metal instrumentation in cases of spinal tuberculosis at Dr D. Y. Patil Hospital and Research Institute, Kolhapur. Malaise, night sweats, back pain, and weight loss are frequent presenting indications as well as prevalent constitutional symptoms.1 A restricted range of motion and localised spinal deformity was found during a physical examination. Increase in erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) and Total Lukocyte count on lab reports was seen. All patients had MRI of spine confirming spinal infection. All patients underwent posterior instrumentation and trans peduncular debridement. Informed consent was taken from all patients. This is a retrospective observatory study.
X-ray findings
The early stages of a spinal infection are often characterised by normal plain radiographs. Narrow disc space and endplate degradation can be shown on radiographs. Although bone damage might not be seen for a few weeks [Figure 1]. In contrast, spinal TB is more frequently observed posteriorly and may manifest as vertebral body involvement during the early stages of infection while preserving the disc space.
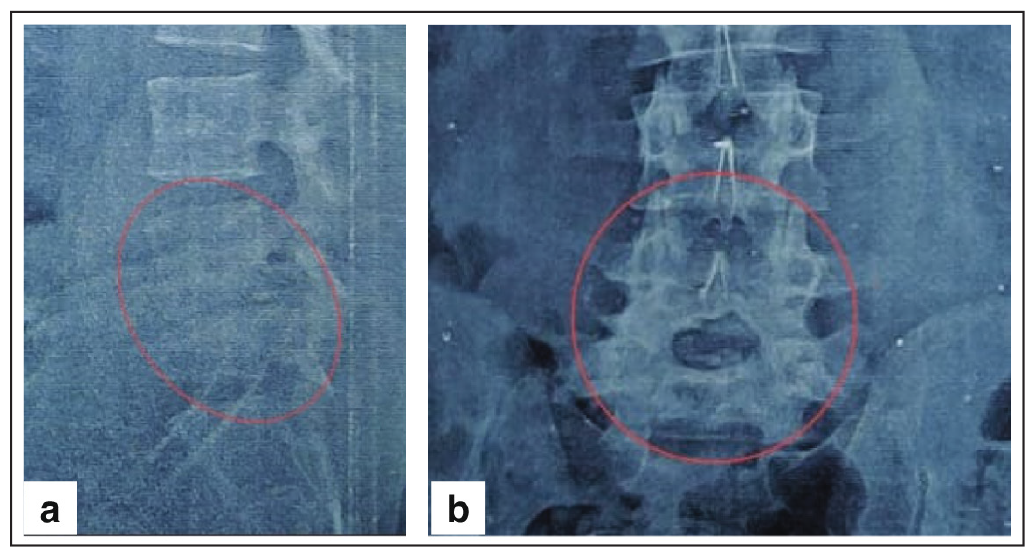
- Pre-operative (a) lateral–shows reduce disc space and (b) anteroposterior (AP)–arthropathy. Disc space reduction shown with red circle in x-ray.
Magnetic resonance imaging findings
The pictures contrast-enhanced MRI is the preferred method for detecting spinal infections. MRI use in determining the difference between pyogenic spine infection and tubercular spinal infections, give superior imaging of the paraspinal soft tissue, and indicate the extent of the infection. When there are neurologic impairments, MRI is essential for planning the surgical strategy, levels of decompression, and stabilisation. For the best outcomes in determining whether there are any skip abscesses or other areas of neurologic compression.1 MRI scanning of the whole spine if available. Early MRI changes associated with infection usually indicate increased T2 and decreased T1 signal intensity in the affected discs and surrounding endplates/vertebrae, as well as elevated T2 signal in the paraspinal soft tissues.1 Early MRI findings of increased internal contrast uptake and T2 disc signal are quite sensitive (70–100%) for diagnosis. A huge thoracic spine involvement, well-defined paraspinal abscess with limited rim enhancement and smooth borders, and subligamentous extension to neighbouring vertebrae are MRI findings that can assist differentiate spinal TB from pyogenic spine infection [Figure 2] with skip lesion, multilayer involvement, and intact disc height. To show the degree of osseous deterioration and for preoperative planning, a computer tomography (CT) scan should be acquired; however, the epidural spaces and soft tissue involvement are not well evaluated on CT.
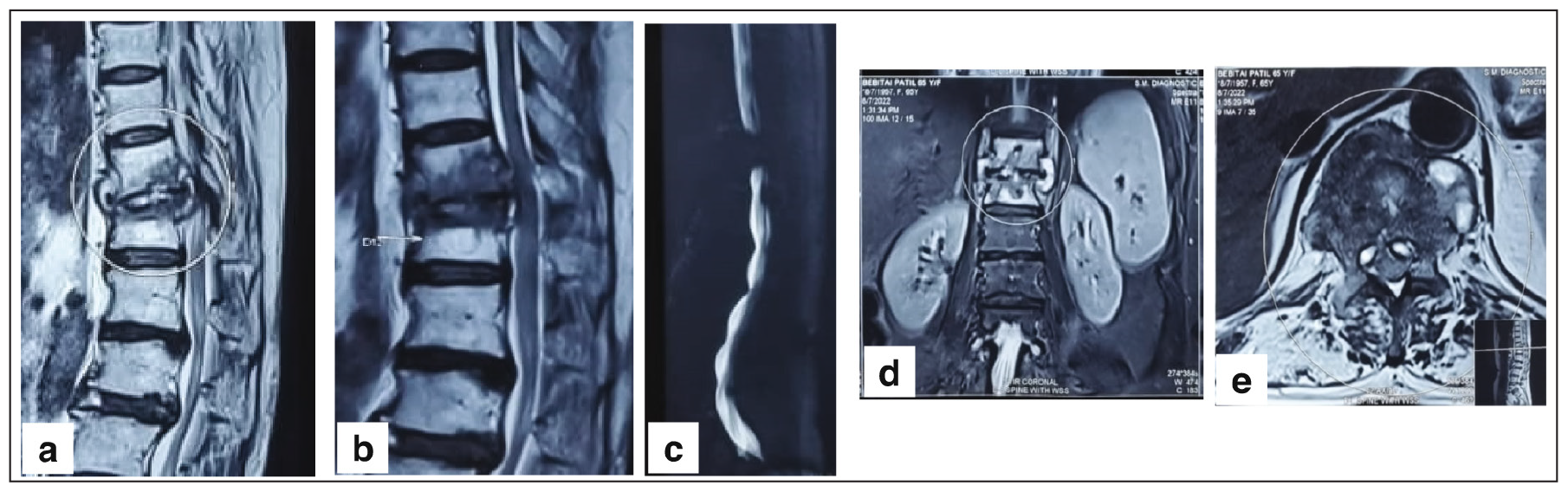
- (a) Saggital T2, (b) Saggital T1, (c) Mylogram, (d) Coronal cut and (e) Axial cut. Pott’s disease-related pan vertebral involvement of the D12 vertebra and pedicle degradation are visible in the magnetic resonance imaging (MRI) of a 69-year-old female patient (circle).
Laboratory
Two serological indicators that can be used as screening methods to distinguish between less significant and more serious causes of back pain are ESR and CRP. Although CRP and ESR are frequently increased together, CRP has a shorter half-life than ESR, making it more sensitive and useful for monitoring therapy response.5 White blood cell (WBC) count is frequently employed as a screening technique; TB is less commonly linked to increased inflammatory markers than pyogenic spine infection. Despite the fact that blood cultures lack sensitivity, since positive results influence antibiotic selection and may point to inferior nonoperative outcomes, they should be carried out on every patient with a suspected spinal infection.5
Cultures and biopsy
Despite the usefulness of improved imaging, the management of antimicrobial treatment depends heavily on diagnostic cultures. Tissue biopsy with a CT-guided needle biopsy is frequently necessary in individuals who don’t show signs of needing immediate surgical treatment. Prior to getting cultures, antibiotics should be withheld, since studies have indicated that empirical therapy is linked to a reduced diagnostic yield [Figure 3].
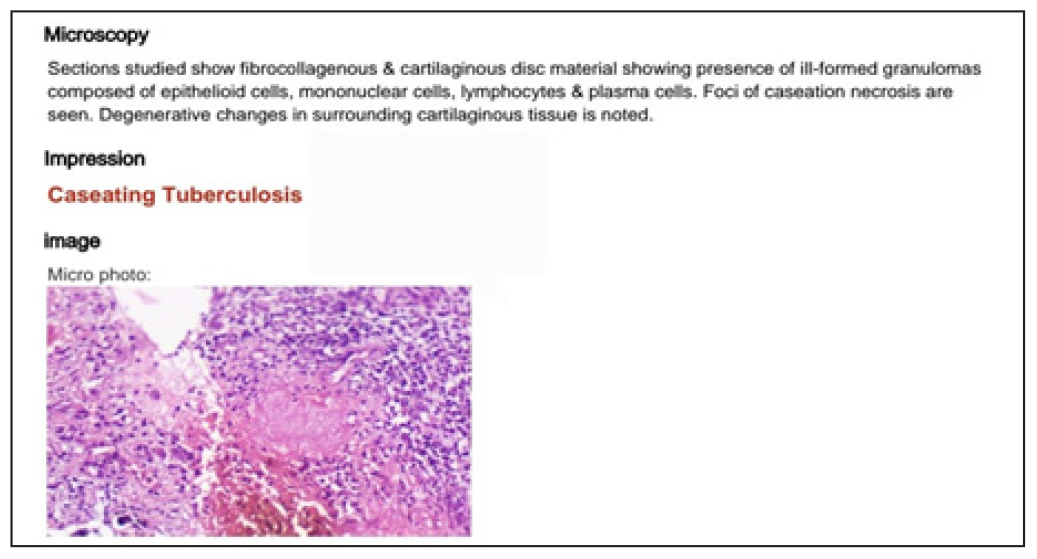
- Microbiological reports of biopsy sample.
Spinal instability
Chronic inflammation of the two columns, as in spinal TB, may not always result in the spine being unstable because tissues demonstrate a contemporaneous healing response despite being damaged by the infectious process.1,6 When a pathological fracture of infected vertebral body results from a mechanical trauma, there is a severe instability of the spine. All three spinal columns may become unstable and unable to withstand temporary loads in tubercular lesions, which might cause the spinal column to dislocate or sub lux pathologically, resulting in a profound neurological deficiency. Similar to this, doing a laminectomy on an infected vertebral body results in a greater neurological deficit and ensuing paraplegia. Biomechanical stresses are more pronounced in tubercular lesions of junctional sites, such as the cervico-dorsal, dorsolumbar, or lumbo-sacral spine, where a fixed segment and a moveable segment meet and the spinal curvature is changed from kyphosis to lordosis or vice versa.3,4 Since a portion of the damaged vertebral body must be removed during surgery to enable spinal-cord decompression, axial pain, pain on movement, pain during turning in bed this process increases instability.7
Posterior instrumentation with intradiscal debridement
In this procedure, a midline posterior incision is used to expose the spine Laheri et al. employed the Hartshill technique [Figures 4a and 4b], we used pedicle screw to fix the segment [Figures 4c and 4d]. Thorough disc debridement is done and sample for microbiology obtained. Unlike the majority of recent research that used pedicle screw fixation. The posterior instrumentation had complications such as implant prominence, fracture, and implant loosening. Additionally, there were side effects from the method, include skin necrosis, infection, and wound dehiscence. This procedure is challenging and is associated with a lengthier surgery time and greater blood loss.3,4
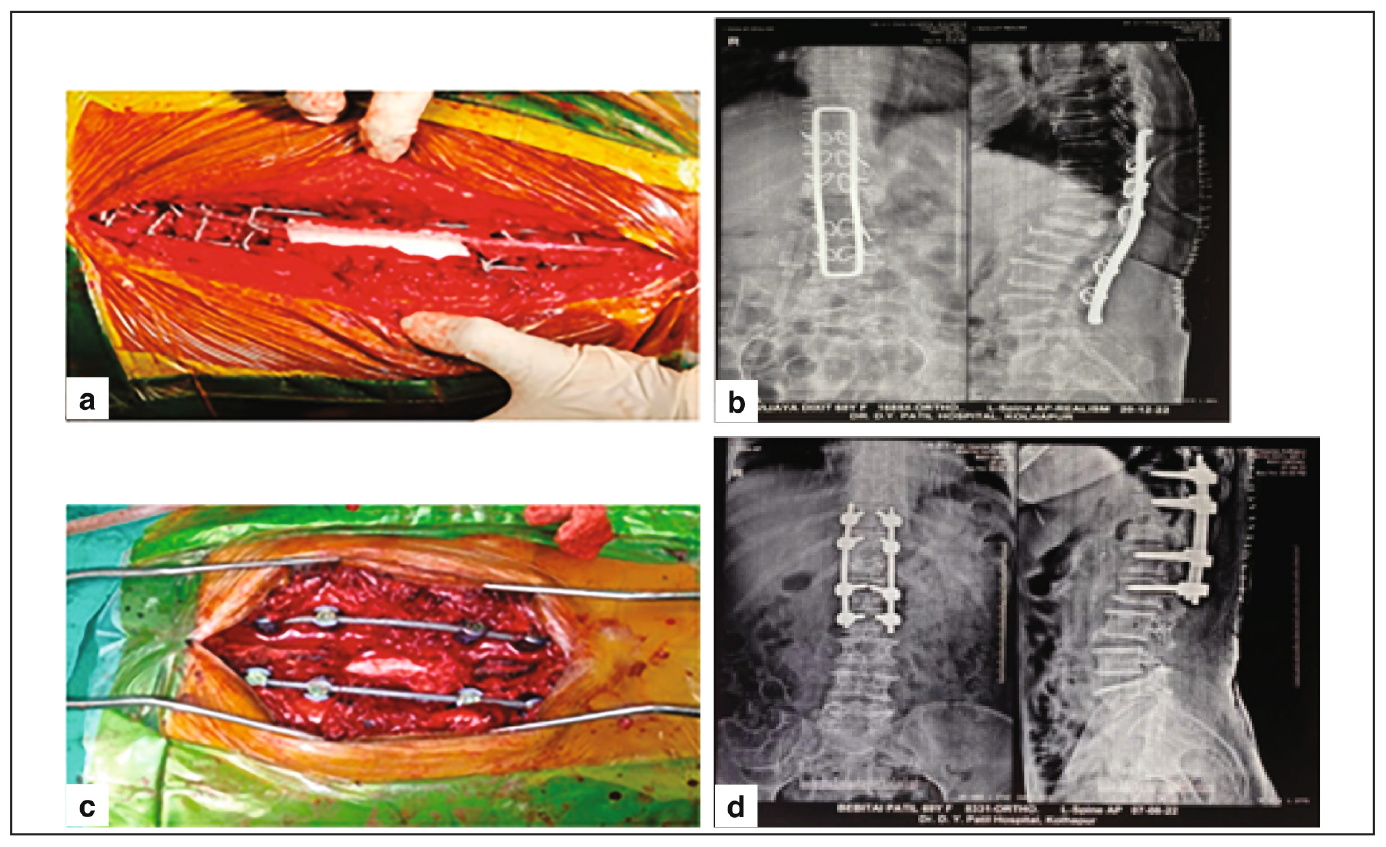
- (a) Hartshill fixation intraop image. (b) Intraop pedicel screw fixation. (c) Post op pedical screw fixation. (d) Post op hartshill fixation.
RESULTS
In patients with spinal TB who had surgery and received posterior spinal instrumentation. Experimental analysis was done to determine the mycobacterium TB’s ability to stick to metal such as stainless steel. Staphylococcus adheres to stainless steel more frequently than mycobacteria, which rarely do.5,8 In contrast to mycobacteria, pyogenic organisms produce a thin biofilm. So, technically, using an implant when infected with TB is safe.5,9 When the whole spine was involved or laminectomy was required for an anterior illness, Harrington distraction rods or sublaminar segmental wiring were originally used for stability.8 In investigations that followed, posterior stabilisation with Harrington rods or Luque segmental wire was found to stop graft-related problems and eventual development of kyphosis in patients with larger preoperative vertebral body loss or graft lengths longer than two-disc heights.3,8 None of the major complications linked to posterior instrumentation, such as loosening, breakage, and implant prominence, were observed, with the exception of approach-related problems such infection, skin necrosis, and wound dehiscence.5
CONCLUSION
In this study total seven patients with pot’s spine underwent Posterior Instrumentation and disc debridement and continue kept on drug therapy according to culture sensitivity in period of 2020 to 2022. Following visits at one month, three months, and six months, cheeks were checked for pain alleviation (based on Vas Score) [Table 1], functional recovery for day-to-day activity, and radiologically and clinically instrumentation status. We found that despite having active infection on surgical time in case of tubercular mycobacterium no significant complication regarding implants such as implant loosening, breakage, worsening of symptoms after instrumentation, surgical site infection and re-surgery were noted.
| No. | VAS Pre op | VAS on one month | VAS on three month | VAS on six month | Day to day activity able to DO Y/N | Complication |
| 1. | 7 | 3 | 2 | 3 | Yes | No complication |
| 2. | 6 | 3 | 1 | 2 | Yes | No complication |
| 3. | 8 | 2 | 3 | 2 | Yes | No complication |
| 4. | 6 | 4 | 2 | 1 | Yes | No complication |
| 5. | 7 | 5 | 4 | 4 | No | Bowel bladder incontinence and neuro deficit |
| 6. | 8 | 3 | 2 | 3 | Yes | No complication |
| 7. | 7 | 2 | 1 | 1 | Yes | No complication |
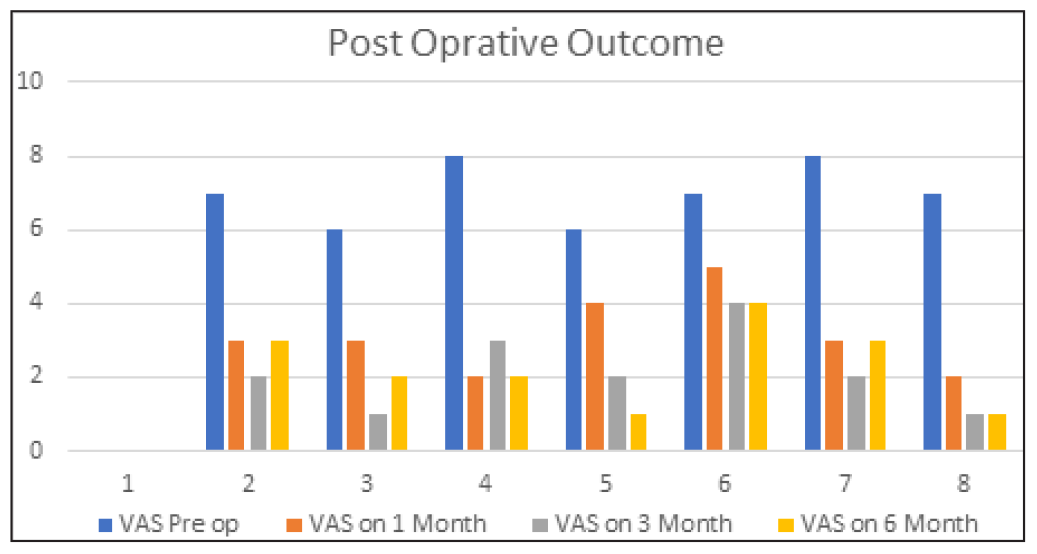
VAS: Visual analog score, Y/N: Yes/No.
DISCUSSION
A wide range of illnesses, including discitis, Vertebral osteomyelitis, and sub epidural abscess, are classified as spine infections.7 S. aureus is the most frequent cause of pyogenic spine infection, whereas M. tuberculosis is the most frequent cause of granulomatous infectious disease. High levels of suspicion are essential, especially in patients with risk factors like immunosuppression, IV drug use, and recent travel to endemic areas. MRI is the imaging study of choice, both with and without contrast. But for the best possible care, it is crucial to do diagnostic culture via CT-guided or open biopsy.1The majority of spine infections can be successfully treated without surgery using bracing and antibiotics. Surgery is required in cases of neurologic deficits, spine instability, advancing deformity, and nonoperative therapeutic failure. The optimum surgical strategy depends on the site, the degree of the infection, and the degree of spine instability.
Ethical approval
Institutional Review Board approval is not required as it is a retrospective observatory study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of Artificial Intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
REFERENCES
- Evaluation and management of pyogenic and tubercular spine infections. Curr Rev Musculoskelet Med. 2018;11:643-52.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Spinal tuberculosis: Current concepts. Global Spine J. 2018;8(4 Suppl):96S-108S.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Instrumented stabilisation in spinal tuberculosis. Int Orthopaedics. 2012;36:285-92.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Evaluation of the risk of instrumentation as a foreign body in spinal tuberculosis: Clinical and biologic study. Spine. 1998;23:1160-3.
- [CrossRef] [PubMed] [Google Scholar]
- Drug therapy in spinal tuberculosis. Eur Spine J. 2006;15(Suppl 4):587-93.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Pyogenic vertebral osteomyelitis: Report of nine cases and review of the literature. Rev Infect Dis. 1980;2(2):196-206.
- [CrossRef] [PubMed] [Google Scholar]
- Single stage decompression, anterior tnterbody fusion and posterior instrumentation for tuberculous kyphosis of the dorso-lumbar spine. Spinal Cord. 2001;39:429-36.
- [CrossRef] [PubMed] [Google Scholar]
- Tuberculosis of spine: A fresh look at an old disease. J Bone Joint Surg. 2010;92:905-13.
- [CrossRef] [PubMed] [Google Scholar]
- The classic wiring of the vertebrae as a means of immobilisation in fractures and Pott’s disease. Clin Orthop Related Res. 1975;112:4-8.
- [Google Scholar]




