
Translate this page into:
Tuberculosis presenting as a scaphoid fracture: A rare case report
Address for correspondence: Dr. Ganesh Singh, Department of Orthopaedics, Government Medical College, Haldwani - 263 139, Uttarakhand, India. E-mail: drganeshortho@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Dharmshaktu GS, Pangtey T. Tuberculosis presenting as a scaphoid fracture: A rare case report. J Orthop Allied Sci 2019;7:31-3.
Abstract
Tuberculosis of the wrist is an uncommon clinical entity and mostly presents as insidious pain and swelling. Presentation of singular carpal bone involvement is rare as the presenting feature. A case of scaphoid fracture was evaluated in a 20-year-old male patient, and underlying tuberculosis was diagnosed on magnetic resonance imaging and culture of joint fluid. Antitubercular therapy under appropriate supervision resulted in clinical improvement and optimal regain of function. No reactivation of the disease was noted in a follow-up of 2 years. This case highlights a rare presentation of tuberculosis presenting with a fracture of scaphoid.
Keywords
Carpal
fracture
scaphoid
tuberculosis
wrist

Introduction
Wrist joint is an uncommon location for osteoarticular tuberculosis with reported incidence of <1% of all skeletal tuberculosis cases.[1] Initially, synovial or joint capsule involvement is found, which may later affect the entire joint with synovial hypertrophy and bone erosions. Radiographs may reveal joint-space narrowing, eccentric lesion, and juxtaarticular osteoporosis as the usual features. Pathological fracture of isolated carpal bone like scaphoid is a rare event and may delay the diagnosis in the absence of constitutional features.
Case Report
A 20-year-old male patient was brought to us for left wrist pain for 3 months that was increasing for the last 2 weeks, and the radiographs revealed fracture of scaphoid waist region without associated bony injuries. He was given plaster splints for a total period of 6 weeks following which the radiograph revealed the presence of fracture gap without union [Figure 1]. The pain and swelling were found to be increased with limitation of range of motion. The magnetic resonance imaging (MRI) was advised and evaluated to reveal marrow edema in scaphoid with fracture through the waist area. A few cystic changes were noted near the irregular fracture line. The entire scaphoid was seen with altered signals with hypointense in T1 and hyperintense in T2 and fat-suppression images. There was extensive surrounding soft-tissue edema with synovial proliferation around the scaphoid, and a probable diagnosis of infective etiology was suspected [Figures 2 and 3]. The wrist joint was aspirated under fluoroscopic guidance, and the aspirate was sent for culture and sensitivity, Gram stain, stain for acid-fast bacilli, and polymerase chain reaction (PCR) for tuberculosis. The culture was positive for Mycobacterium tuberculosis. Appropriate body weight-related four-drug antitubercular treatment was initiated following relevant baseline blood investigations. A marked improvement was noted after 5 weeks of therapy that was continued till 18 months as per the institutional protocol with staged conversion to three- and two-drug regimen. Pain and swelling were decreased, and the range of motion was also improved leading to improved activities of daily living. Radiograph at the end of therapy, however, showed ankylosis between carpals and almost pancarpal ankylosis while clinical profile was dramatically improved.
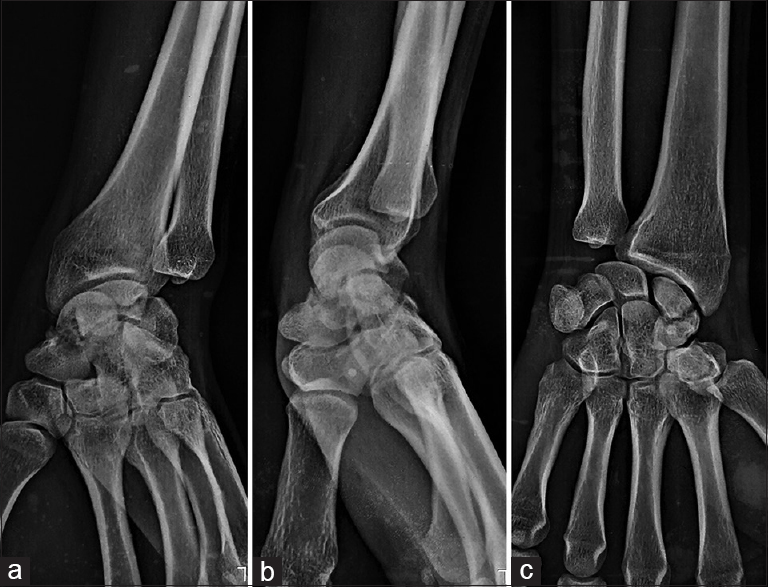
- The radiograph showing fracture of scaphoid in oblique (a) and two orthogonal views (b and c). There is, however, area of cystic lucency surrounding fracture line and the rest of the bones appear normal
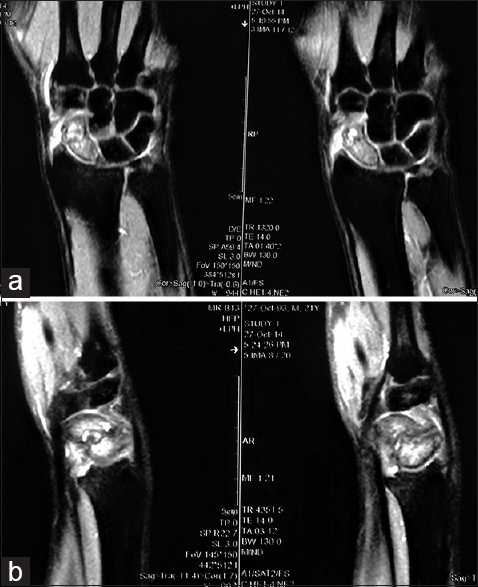
- The magnetic resonance imaging showing marrow edema and destruction of scaphoid and surrounding extensive soft-tissue edema in T1 coronal (a) and sagittal views (b)

- The same lesion is hypointense in fat-suppressed coronal (a) and sagittal T1 view showing the altered signal and destruction of scaphoid (b)
Discussion
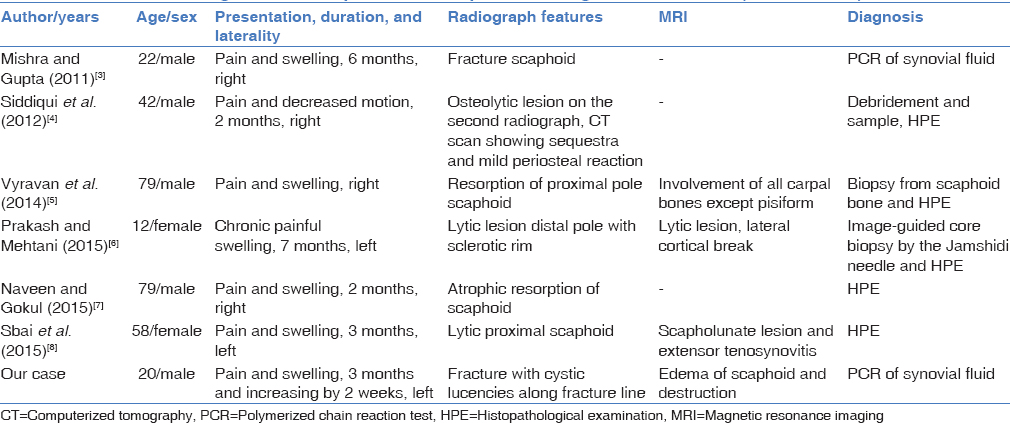
Isolated scaphoid involvement is rare in tuberculosis and even is not described in large series of wrist tuberculosis of 32 cases.[2] We could gather only six reported cases of isolated scaphoid affliction out of several with wrist monoarthritis or with multiple carpal and tenosynovial involvement. Of the reported cases with scaphoid involvement, the fracture at initial presentation is described in just one case.[3] In an another case, scaphoid cortical breach was appreciated only in the MRI and cases of tubercular scaphoid involvement (diagnosed with or without MRI) that were later confirmed by histopathological examination or PCR are very few.[3-7] One case of scapholunate ligament has been described, along with extensor tenosynovitis, without any involvement of scaphoid and that we have also included in the list [Table 1]. This case snippet highlights the importance of careful evaluation of seemingly common clinical entities to rule out significant underlying pathology by clinical and judicious investigative means.
Conclusion
The uncommon presentation of common problems in the endemic region should be acknowledged and anticipated. Fractures with conspicuous features, at times, require further evaluation to rule out sinister underlying pathology. A careful history, clinical assessment, and judicious use of imaging are critical to timely diagnosis followed by appropriate treatment.[8]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Tuberculosis of the Skeletal System (Bones, Joints, Spine and Bursal Sheaths) (3rd). New Delhi: Jaypee Brothers; 2004.
- [Google Scholar]
- Tuberculosis of the hand: Clinical presentation and functional outcome in 32 patients. J Bone Joint Surg Br. 2009;91:1054-7.
- [Google Scholar]
- Tuberculosis of wrist presenting as scaphoid fracture: A case report. Malaysian Orthop J. 2011;5:47-9.
- [CrossRef] [Google Scholar]
- Isolated tubercular scaphoid osteomyelitis: A case report. Orthop Surg. 2012;4:64-6.
- [CrossRef] [PubMed] [Google Scholar]
- Scaphoid tuberculosis difficulties of diagnosis. IOSR J Dent Med Sci. 2014;13:44-5.
- [CrossRef] [Google Scholar]
- Isolated tuberculosis of scaphoid in the skeletally immature: A rare cause of chronic wrist pain. BMJ Case Rep 2015:2015. pii:bcr2015209569
- [CrossRef] [PubMed] [Google Scholar]
- Pathological resorption of the scaphoid: A rare presentation of the TB wrist. J Clin Orthop Trauma. 2015;6:77..
- [CrossRef] [Google Scholar]
- A rare localization of tuberculosis of the wrist: The scapholunate joint. Int J Mycobacteriol. 2015;4:161-4.
- [CrossRef] [PubMed] [Google Scholar]




