
Translate this page into:
Tracheoesophageal fistula in a case of Pott’s spine: Unusual presentation amid COVID pandemic
Address for correspondence: Dr. Samruddhi Dhanaji Chougale, Plot No. 14, Kashid Colony, Rajopadhyenagar, Kolhapur, Maharashtra 4160102, India. E-mail: samru.c1990@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Anokar AT, Chougale SD, Bargaje M, Deoskar RB, Dhotre A, Prasad A, et al. Tracheoesophageal fistula in a case of Pott's spine: Unusual presentation amid COVID pandemic. J Orthop Spine 2022;10:44-8.
Abstract
Acquired tracheoesophageal fistula (TOF) is a rare entity. We present a case of a 49-year male, non-smoker, with no known comorbidities admitted with acute respiratory symptoms and desaturation to a COVID hospital during the first peak of the pandemic. Initial workup showed all raised inflammatory markers, deranged liver function, and poor ejection fraction of 20%. COVID RT-PCR was negative. Early high-resolution computed tomography done as COVID suspect, peaked up the tracheoesophageal fistula with aspiration pneumonia. On magnetic resonance imaging spine, paradiscal, prevertebral involvement at the D1-D2 level suggesting Pott’s spine, with mediastinal irregular cavity formation, ruptured in trachea and esophagus. A detailed history revealed neck pain for 3 months and increased cough while swallowing for 10 days. Neck pain was not evaluated due to fear of COVID and lockdown. On esophagoscopy, anterior wall of the upper esophagus had fistula with smooth clear margins. Diagnosis of tubercular TOF confirmed on endotracheal inflamed fistulous track secretions. The patient was treated conservatively with initial nasogastric tube feeding and antitubercular treatment achieving complete resolution.
Keywords
Acquired tracheoesophageal fistula
mediastinal TB cavitation
Pott’s spine

Introduction
COVID-19 pandemic had sidelined the access to essential health services affecting outcomes secondary to delayed presentations. As per the Global Tuberculosis Report 2021, this pandemic has affected tuberculosis from both supply and demand side.[1] Here we report a case of an unusual presentation of tuberculosis during COVID pandemic.
Case Report
A 49-year-old male, engineer, immunocompetent, no addictions, was taken to a busy fever clinic during the first wave of the COVID-19 pandemic with complaints of cough, minimal whitish expectoration for 10 days, fever, and breathlessness for 2 days. No chest pain. Oxygen saturation on admission was 93% at room air and blood pressure was 100/68 mmHg. The patient was admitted in the COVID suspect ward. Initial investigations revealed a gross increase in all inflammatory markers [Table 1] and poor ejection fraction (EF). Chest X-ray [Figure 1a] showed right lung inhomogeneous opacity with cardiomegaly. Antibiotics, low-molecular weight heparin, and diuretics were added. COVID RT-PCR was negative on two different occasions. High-resolution computed tomography (HRCT) thorax [Figure 1b and c] showed middle lobe few patchy subtle ground glass opacities (GGOs) with left lower lobe centrilobular nodular GGOs with right sided mild pleural effusion and a fistulous tract connecting the mid trachea to the esophagus. Parenchymal opacities could be viral plus secondary to aspiration in tracheoesophageal fistula (TOF). Sputum culture grew Pseudomonas aeruginosa. Patient was kept nil by mouth and deisolated to the non-COVID side. On detailed history, he had mild increase in cough while swallowing for 10 days. No dysphagia or odynophagia noted. Neck pain and weight loss of around 10 kgs over 3 months were noted. The patient was working from home and had visited a local doctor for neck pain 3 months back but did not consult further due to fear of contracting COVID, isolation, and restrictions imposed during lockdown. No known comorbidities. No past history of tuberculosis or anti-tuberculosis treatment (ATT).
| Investigation Results |
|---|
| On admission |
| • Hb/total leukocyte count/platelet count: 13.8/19,900/173,000 • Total bilirubin/direct bilirubin: 3.4/1.3 • SGOT/PT: 4460/3160 • CRP: 42.2 • D-dimer: 6,915-- 993 – 2,650 • Ferritin: 12,196-- 492 -- 856 • Procalcitonin: 0.98 • BNP: 570 • Urea/creatinine: 75/1.3 |
| Sputum AFB, GM stain smear: epithelial cells >25/LPF. Pus cells 20–25/LPF. Occasional Gram-positive Cocci in pairs, short chains, and clusters seen. Few Gram-negative bacilli seen KOH” No fungal element seen AFB not seen Culture: P. aeruginosa |
| 2D ECHO: LV dilated. Normal sized other cardiac chambers Septum, anterior wall akinetic, thickness preserved. LVEF 15–20% Mild pulmonary hypertension |
| Bronchoscopy samples |
| • BAL CBNAAT: MTB detected very low. R resistance not detected • TO fistula track secretions CBNAAT: MTB detected low. R resistance not detected BAL + TO fistula track secretions • Cytology: No malignant cells seen • AFB culture: No growth after 8 weeks |
| Endotracheal fistula track biopsy HPE: Acute on chronic necroinflammation |
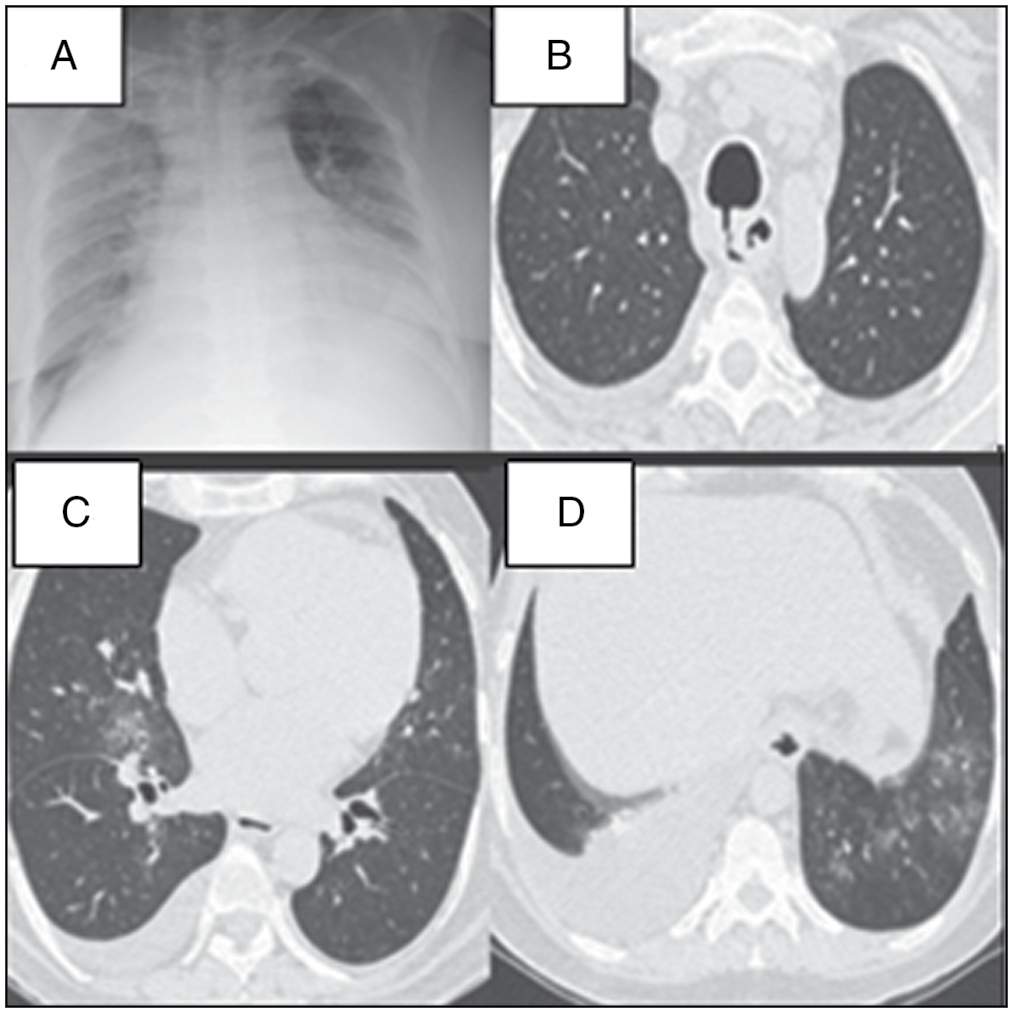
- (a) Chest X-ray on admission-AP film right lung diffuse haziness apparent cardiomegaly. (b-d): HRCT plain: Middle lobe, left LL patchy infiltrates with right pleural effusion, and TOF
Chest ultrasound showed mild right-sided pleural effusion. On diagnostic thoracocentesis, it was transudate.
Contrast-enhanced computed tomography (CECT) after 1 week [Figure 2a,b, c] showed clearing of left lower lobe opacities. A relatively well-defined, peripherally enhancing, cavitary soft tissue inflammatory mass in right paraesophageal and prevertebral location, communicating with trachea and esophagus and asymmetrical circumferential thickening involving the adjacent esophagus; D1-D2 lytic vertebral bodies. No pulmonary embolism. Only few subcentimetric mediastinal lymph nodes seen.
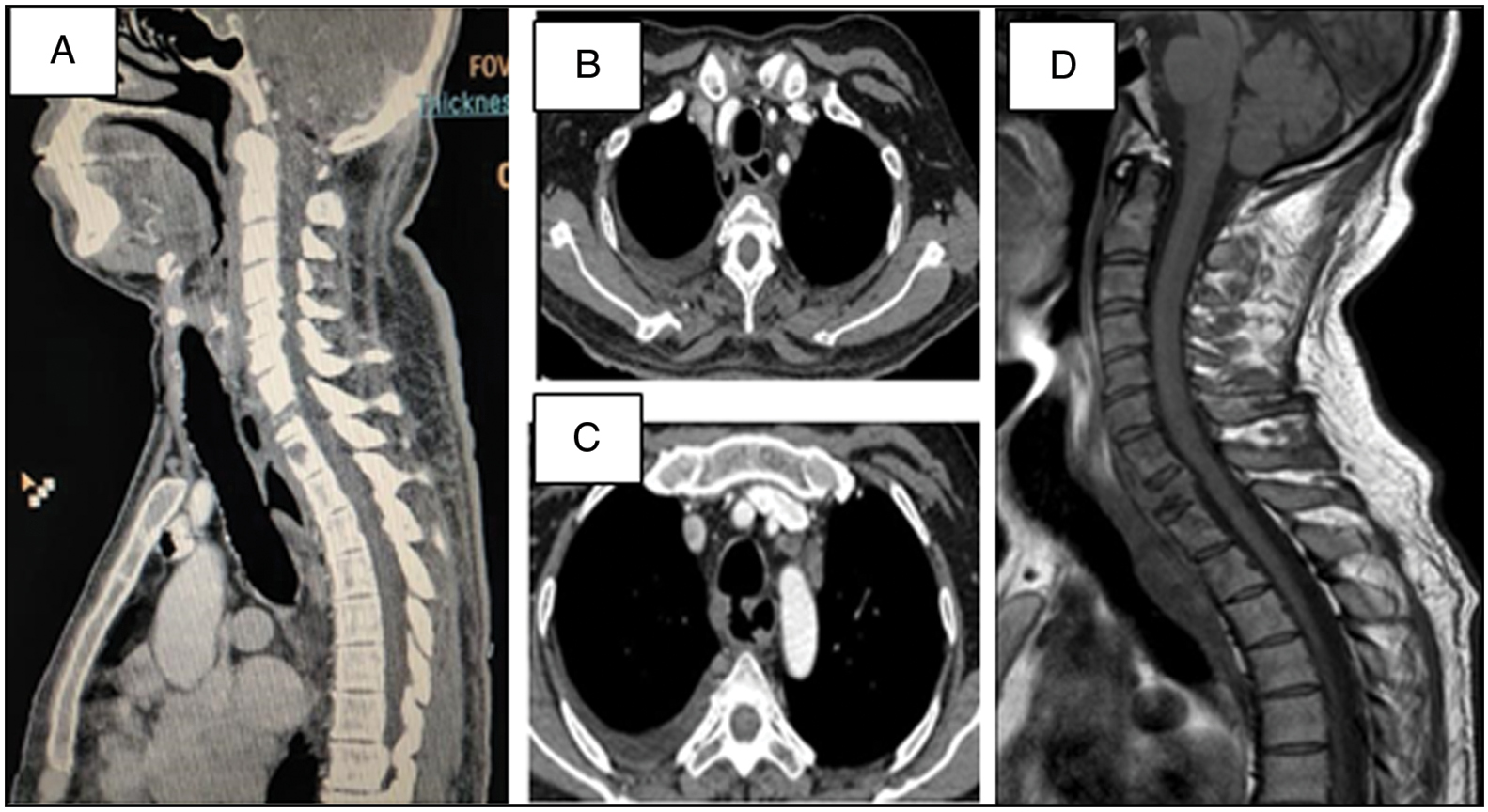
- (a-c): CECT thorax: Relatively well-defined peripherally enhancing cavitatory soft tissue inflammatory mass in paraesophageal and prevertebral location communicating with trachea and esophagus with tracheoesophageal fistula formation and asymmetrical circumferential thickening involving the adjacent esophagus. (d) MRI spine showing prevertebral abscess with destruction of D2-D3 vertebrae
UGI endoscopy [Figure 3a] showed anterior wall esophageal fistula of 22 cm length, clear margins with no ulcers or growth. On bronchoscopy [Figure 3b and c], fistulous tract in mid-trachea, posterior wall, around 7 mm in diameter, with inflammed everted border. A bronchoscope passed through fistulous opening and showed purulent secretions lining the irregular tract and smooth posterior wall mucosa. No active bleeding. Biopsy from the irregular wall surface was obtained along with separate washings from the tract.

- (a) Upper GI endoscopy showing fistulous track in anterior esophagus with smooth margins. (b) Bronchoscopy showing fistula in posterior tracheal wall at the time of diagnosis. (c) Bronchoscopy after 3 months showing healing of the fistula
Magnetic resonance imaging (MRI) spine [Figure 2d] showed enhancing marrow signal intensity in the body of C7-D3 vertebra with partial lytic destruction of D1, involvement of D1-D2 intervertebral disc, and associated prevertebral, paravertebral soft tissue enhancement suggestive of Pott’s spine.
Diagnosis of tuberculosis was confirmed by cartridge-based nucleic acid amplification test (CBNAAT) on TOF secretions and bronchoalveolar lavage (BAL). The patient was started on non-hepatotoxic antitubercular drugs, initially ethambutol, levofloxacin, and streptomycin, later in the course full dose antitubercular drugs (HRZ) were added sequentially as liver function normalized.
For TOF, considering inflammatory mediastinal tract secondary to active TB, a decision to manage conservatively was taken and the patient was discharged on antitubercular treatment (ATT) with nasogastric tube (NGT) feeding. The patient was positively gaining weight on NGT feeding without any aspirations so percutaneous endoscopic gastrostomy (PEG) was not done. The patient was a high-risk surgical candidate and throughout the course, he had no signs of any spinal nerve root compression and hence he was managed conservatively.
After 3 months, CECT [Figure 4a, b,c] showed reduction in mediastinal cavitatory part with small posterior tracheal wall diverticulum. Complete closure of fistulous connection was confirmed with oral + IV contrast imaging [Figure 4a, b,c] and check UGI scopy + bronchoscopy [Figure 3c]. Then the NGT was removed and the patient started on soft oral feeds without any complications. At the end of 1 year, CECT [Figure 4d,e,f] showed resolution of paraspinal and mediastinal soft tissue cavitation with reduction in size of tracheal diverticulum. ATT continued for a total of 18 months with close monitoring.
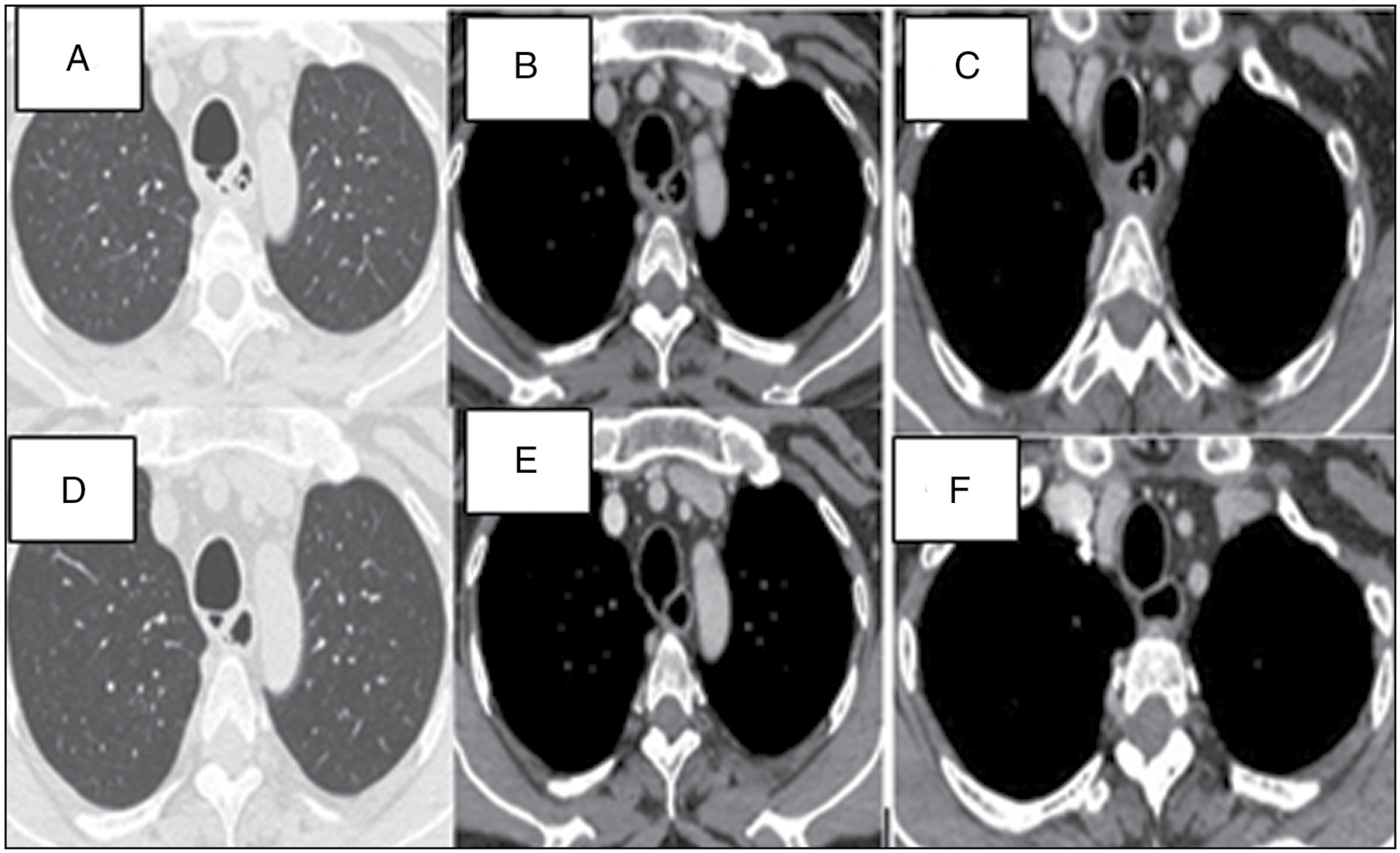
- (a-c) CECT after 3 months and (d-f) CECT after 1 year of starting ATT, showing posterior tracheal wall diverticulum and progressive clearing of mediastinal soft tissue cavitation
Discussion
Impact of COVID-19 pandemic
Peak of COVID-19 pandemic overwhelmed health care with acute respiratory symptomatics affecting initial clinical evaluation in high volume centers. HRCT use skyrocketed since COVID. In this case, having severe presentation with multiorgan dysfunction syndrome (MODS), early use of HRCT as COVID suspect helped to pick up TOF in the absence of cough while swallowing as a presenting complaint.
In COVID-19, inflammatory markers were widely used to assess severity and prognosis.[2] There is a raised level of D-dimer, and C-reactive protein is reported with pulmonary TB,[3] but rarely done in practice. Our case reveals unusually high inflammatory markers in a non-COVID TB case, in the absence of florid lung involvement, thrombo-embolism, or other features of hemophagocytic lymphohistiocytosis (HLH) syndrome.
This case throws light on some of the factors contributing to delayed presentation with multiple severe complications in a case of TB during COVID-19 pandemic.[1]
Acquired tracheoesophageal fistula
Pathological connection between trachea and esophagus (TOF) can occur at any level secondary to malignancies, granulomatous diseases, infections, trauma, or surgery.[4,5] Acquired TOF secondary to tuberculosis is an uncommon complication with few reported cases.[6,7]
Possible mechanisms of TOF in tuberculosis are rupture of necrotic mediastinal lymph node into trachea and esophagus, erosion of endotracheal tubercular ulcer into adjacent esophagus, or primary esophageal TB eroding trachea.[4,6] Formation of tracheal or esophageal diverticulum, which gives away secondary to adhesions in mediastinal structures due to TB, is a possible mechanism in this case.[4,6]
Mechanism of TOF in Pott’s spine
TOF in a case of spinal tuberculosis is a rarest entity.[8] Spinal tuberculosis has an indolent course, usually involves lower thoracic or upper lumbar vertebrae with hematogenous spread of infection. It affects two adjacent vertebrae along with an intervertebral disc.[9] It may form paravertebral cold abscess, which tracks along paravertebral plane due to gravity and can affect vertebral column at multiple levels. This cold abscess spreads further throughout the fascial planes and is limited by longitudinal ligament. The abscess can burst open into the mediastinum under high pressure.[8,9] It can be life-threatening. Mediastinal TB abscess formation is rare.[6,8,10] Paravertebral abscess formation in spinal TB is common, and endobronchial fistulization was seen in 3 out of 178 cases.[10]
In our case, the patient was presented to a hospital 3 months after the onset of neck pain. By this time, he had developed the paravertebral abscess with irregular soft tissue cavity in the adjacent mediastinum. There was no evidence of discrete necrotic mediastinal nodes or primary pulmonary or esophageal TB.
Acquired TOF evaluation and management of tubercular TOF
Clinical history of worsening of cough while swallowing (Ono’s sign),[11] and in some cases presence of food particles in expectoration, provides important diagnostic clue to proceed with further evaluation for TOF. Chest X-ray may reveal aspiration pneumonia. CECT thorax can localize the fistula and provide etiological clue, whereas esophagoscopy and bronchoscopy will give a gross picture of the same and allow diagnostic sampling in some cases.
Treatment of TB involves ATT drugs according to sensitivity. In tubercular TOF, conservative management with NGT or PEG feeding along with ATT is shown to be effective without any intervention for TOF.[7,10,12] In another approach, for TOF with esophageal TB staplers, stents or surgical repair was done along with ATT.[6,12]
In a similar case of Pott’s spine having mediastinal abscess communicating with esophagus and trachea at different levels, surgical intervention was done for Pott’s spine to close the communication.[8]
In our patient, pulmonary TB as on BAL positivity for acid-fast bacilli (AFB) was secondary to aspiration of fistula content from mediastinal abscess. Pott’s spine usually presents with signs of spinal nerve root compression.[9,10] This is one of the rarest cases of Pott’s spine presenting as TOF, aspiration pneumonia with MODS, and having complete recovery on conservative management along with ATT.
Conclusion
TOF as a complication of Pott’s spine is rare and needs thorough clinical and radiological evaluation. Conservative management with close follow-up in TOF secondary to treatable causes needs to be primarily considered to prevent morbidity and cost associated with corrective interventions.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- https://www.who.int›global-tuberculosis-report-2021. [Last accessed on 18 Feb 2022]
- Association of inflammatory markers with the severity of COVID-19: A meta-analysis. Int J Infect Dis. 2020;96:467-74.
- [CrossRef] [PubMed] [Google Scholar]
- Plasma D-dimer levels in patients with active pulmonary tuberculosis. Turk Thorac J. 2005;6:57-61.
- [Google Scholar]
- Acquired non-malignant esophagorespiratory fistula. Am J Surg. 1957;93:321-8.
- [CrossRef] [PubMed] [Google Scholar]
- Management of tracheo-oesophageal fistula in adults. Eur Respir Rev. 2020;29
- [CrossRef] [PubMed] [Google Scholar]
- Esophageal tuberculosis associated with esophagotracheal or esophagomediastinal fistula: Report of 10 cases. Gastrointest Endosc. 2003;57:588-92. PMID: 12665778
- [CrossRef] [PubMed] [Google Scholar]
- Tuberculous broncho-esophageal fistula managed conservatively. Lung India. 2005;22:65..
- [Google Scholar]
- Simultaneous esophageal and tracheal fistulization resulting from Pott’s abscess. Ann Thorac Surg. 2016;102:e343-5.
- [CrossRef] [PubMed] [Google Scholar]
- Pediatric and adult spinal tuberculosis: Imaging and pathophysiology. Neuroimaging Clin N Am. 2015;25:209-31.
- [CrossRef] [PubMed] [Google Scholar]
- [Bronchial fistula caused by Pott’s abscesses, Report of 3 cases] Rev Pneumol Clin. 1989;45:175-8.
- [Google Scholar]
- Oesophago-bronchial fistula in the adult. Thorax. 1965;20:226-33.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical profile and management of tuberculous bronchoesophageal fistula. J Dig Endosc. 2013;4:103-6.
- [CrossRef] [Google Scholar]




