
Translate this page into:
To Compare the results of anterior cruciate ligament reconstruction with preservation versus total removal of torn anterior cruciate ligament stump
Address for correspondence: Dr. S. K. Rai, Department of Orthopaedics, Basishtha Hospital, Guwahati - 781 029, Assam, India. E-mail: skrai47@yahoo.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Gupta TP, Rai SK, Kashid M. To compare the results of anterior cruciate ligament reconstruction with preservation versus total removal of torn anterior cruciate ligament stump. J Orthop Spine 2020;8:96-102.
Abstract
PURPOSE:
Reconstruction of anterior cruciate ligament (ACL) with torn ligament remnant preservation is done with the aim to improve the proprioceptive function and vascularization of new graft. In our study, we compared the results of ACL reconstruction with and without preservation of femoral and tibial ACL torn stumps.
MATERIALS AND METHODS:
This is a prospective study consisting of 100 patients distributed into two groups. Group A (n = 50) underwent reconstruction of ACL with remnant stump preservation and Group B (n = 50) underwent reconstruction of ACL with total removal of ACL remnant from the femur and tibia.
RESULTS:
The present study did not show any significant differences in terms of stability and ACL laxity in the study groups. However, a remarkable difference was noted in proprioception and functional results in both the groups, with Group A (>20%) showing better results.
CONCLUSION:
Based on our study, we can conclude that it is judicious to keep ACL stump as much as possible, and it is advisable to wait till 4 weeks to get inflammatory phase subsided. Preservation of remnant should not interfere with ACL footprint visualization. Remnant preservation improves proprioception of the knee and functional outcome.
Keywords
Anterior cruciate ligament footprint
anterior cruciate ligament remnant
anterior cruciate ligament reconstruction
proprioception knee

Introduction
Anterior cruciate ligament (ACL) injury is the most common ligament injury around the knee joint. It is better treated by reconstruction nowadays. However, there is existing controversy with respect to the preservation of torn ACL remnants during reconstruction. Few studies have reported the benefits of stump preservation for better graft incorporation and postoperative function, although no agreement has been reached.[1,2] To date, in the present literature, there is not sufficient scientific evidence to support the value of preserving the remnant. Few published studies mentioned about enhancing the vascularization as well as the proprioceptive function of the graft after its reconstruction.[1,2,3] Remnant preservation is a little difficult because it obstructs the visualization of the femoral footprint and placement of guide pine for making a tunnel.[1] When the remnant is torn from the femoral ACL footprint, the tibial stump may be preserved if present.
With improved surgical and arthroscopy instrumentation and technology, the outcome of ACL reconstruction is variable. The knee laxity and stability of the grafted ACL has poorly correlated functional outcome and patient satisfaction.[4] There are varying consequences after ACL reconstruction in the present literature, and we thought that it could be due to anatomic factors such as thickness and length of the graft, fixation device, femoral and tibial tunnels. The new concept of functionality as mechanoreceptors, proprioception, and counterbalancing mechanisms has recently attracted attention. Whether they play any significant role in postoperative stability is under evaluation. Zimny et al. in their study have shown better results because the proprioceptive feedback might be responsible as they presumed.[5]
Keeping in mind the ideology of preservation of tibial and femoral stumps, we divided our study into two groups: one group had ACL reconstruction with both stumps' preservation and the other group had ACL reconstruction without preservation of stump. With the torn remnant, it is difficult to locate the exact site of ACL footprint on lateral femoral condyle unless it is removed by shaver.
It is now well known from many reports that many mechanoreceptors are distributed in the ACL tissue, and remnant tissue contributes to the proprioceptive function of the knee.[6] Intact as well as torn ACL has mechanoreceptors, but when torn remnant is completely removed during surgery, these receptors are lost. Georgoulis et al., in their study, reported the presence of mechanoreceptors in torn ACL remnant even after 3 years after a rupture which was attached to the posterior cruciate ligament (PCL) as examined arthroscopically.[7] They also noted that mechanoreceptors and proprioceptive fibers in ACL were stained positively with monoclonal antibody for neurofilament protein in 50% of torn ACL remnants. They also noted the differences among mechanoreceptors in intact and torn ACLs and their clinical importance. Lee et al. found mechanoreceptors in about one-third of cases of ACL remnants, which was fewer than predicted. There is a reduction in some mechanoreceptors in the remnant of ACL stump after an injury usually in 2–14 days.[8]
Many studies have noted the presence of mechanoreceptors in the normal knee joint, normal ACL as well as in torn ACL, however, its existence in injured and grafted ACLs is less than normal and correlated negatively with the duration since the initial injury. After injury, mechanoreceptors do appear in the torn ACL remnant as well as in the newly grafted tendons but of different morphology. Therefore, remnant-preserving surgery may be performed as far as possible and as early as possible after the injury to gain maximum of remnant function which might help in reinforcing ACL reconstruction. As far as regeneration of mechanoreceptor on reconstructed ACL is concerned, it is a subject of research.
Materials and Methods
The study was conducted between January 2012 to December 2014 in the Department of Orthopaedics, Basishtha Hospital, Guwahati, Assam, India. All included patients completed follow-up till 5 years in February 2019.
A total of 131 patients underwent surgery of an isolated unilateral ACL injury after fulfill of inclusion criteria. Of the 131 patients, 31 could not be considered for remnant preservation because there was no identifiable ACL remnant tissue left. Finally, 100 patients were included in the study and completed the follow-up for 5 years. These 100 patients were divided into two groups. Group A (n = 50) underwent ACL reconstruction with remnant preservation and Group B (n = 50) underwent the same surgery with total removal of ACL remnant from the femur and tibia. There were 46 males and 4 females in Group A and 41 males and 9 females in Group B.
Inclusion criteria
range 19–40 year
Recent (<6 months) ACL injury with or without minor meniscus injury (does not require excision or repair).
Exclusion criteria
Age above 40 year
Old (more than 6 months) ACL injury with a major meniscus tear
Associated PCL injury
Associated medial collateral ligament/lateral collateral ligament injury
Osteochondral lesion/defect in magnetic resonance imaging (MRI)
Previous surgery on ACL injured knee.
Surgical technique
All patients were operated under spinal anesthesia and in supine with the knee flexed at about 90°–100°. The standard anterolateral and anteromedial portals are created in the usual way. Initial diagnostic arthroscopy was performed to confirm the diagnosis. During diagnostic arthroscopy, continuous ACL stump was present in 31 patients and 19 had a stump in discontinuity. Both torn ACL stumps were assessed and preserved, and unwanted tissue was removed with an arthroscopic shaver or punch to visualize ACL footprint on the tibia and femur. If ACL remnant was attached to the PCL, only partial remnant was removed with a shaver. However, the remaining ACL stump from tibial and femoral attachments was not removed. Instead, this tissue was elevated gently as a flap using a sharp periosteum elevator by the knee kept at 110° of flexion. A femoral ACL 7 mm offset guide was placed and a pin was placed through the guide and drilled into the femur, and the tunnel was made according to graft diameter. The length of the femoral tunnel was measured. The tunnel for the tibia is prepared next, using ACL tibial guide. The sharp end of the guide was placed in the middle of ACL remnant on the tibia and the wire was placed, and a tibial tunnel was made using standard methods. We used quadrupled semitendinosus graft and fixation for the femur was done using ACL TightRope (Arthrex), and at the tibial end, biointerference screws were used. After fixation of ACL, graft impingement was checked [Figures 1-3]. The second Group B was operated in the same manner, but all ACL stumps from the tibia and the femur were completely removed with a punch and a shaver. ACL rehabilitation was instituted using standard protocols.
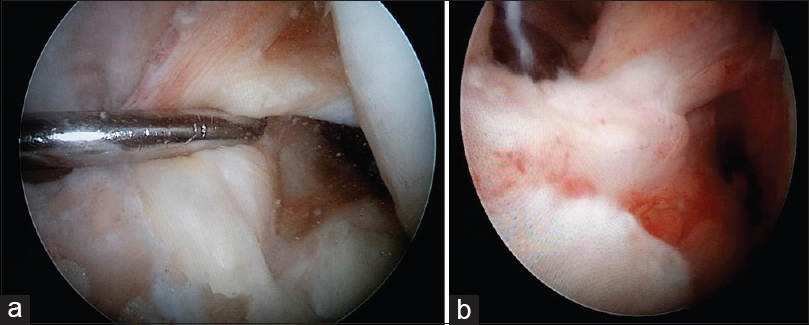
- (a and b) Old anterior cruciate ligament stump before reconstruction
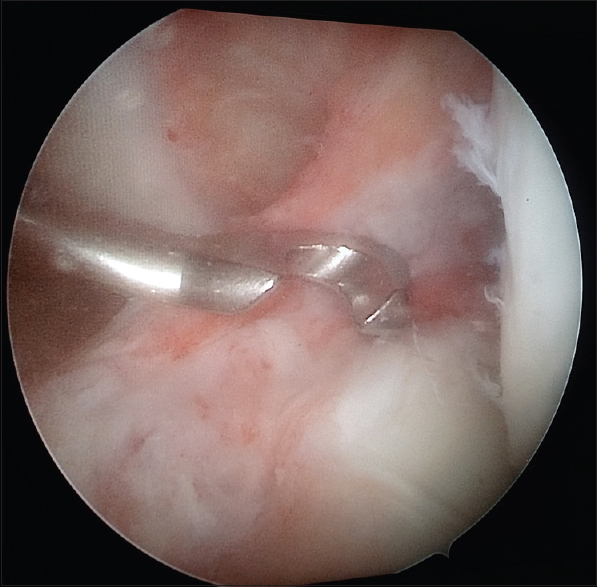
- Anterior cruciate ligament guide in place alongside torn anterior cruciate ligament stump
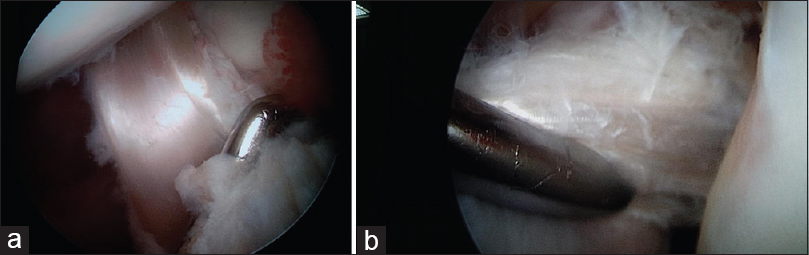
- (a and b) Newly reconstructed anterior cruciate ligament graft along with old anterior cruciate ligament stump
Postoperative clinical evaluation
An independent surgeons who were not a part of study have evaluated postoperative cases. The surgeon who operated on patients has not allowed for postoperative evaluation of the same patients in order to avoid biasness. Each surgeon has evaluated the postoperative knee joint stability using a KT-2000 arthrometer (MEDmetric Corporation, San Diego, CA, USA) by performing Lachman test, pivot-shift test, and tibial femoral displacement test. Side-to-side differences between affected and normal knees were recorded. We also noted a change in the Tegner scale before injury and from surgery to return to sports.[9] Patients who sustained ACL graft rupture or contralateral ACL rupture subsequently after surgery were examined by the same author. We also recorded postoperative data before the revision of ACL reconstruction and were consider as final follow-up data.
Statistical analysis
All statistical analyses were done using SPSS for Windows software version 19.0 (IBM, New York, USA). Both Groups A and B were compared by the Mann–Whitney U-test, with significance level at P < 0.05. To compare the ACL graft tear rates and other variables between both the groups, the Chi-square test was used. We also apply a binary logistic regression test to evaluate the association between each variable and the risk of ACL graft rupture, with significance at the 95% confidence interval (CI) level.
Results
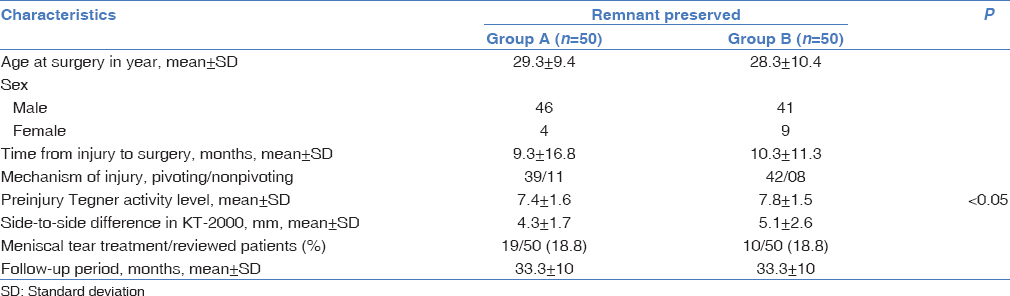
The mean interval between ACL injury and reconstruction was not significant (4.3 ± 9.8 vs. 4.3 ± 7.3 months, P < 0.265), and preinjury Tegner activity was significantly higher (7.4 ± 1.6 vs. 7.8 ± 1.5, P < 0.05; 95% CI, 1.2–13.7) in Group A than in Group B. There were no differences between the groups in the ratio of mechanism of injury (pivoting and nonpivoting), in the incidence of meniscus injury, or in treatment methods [Table 1].
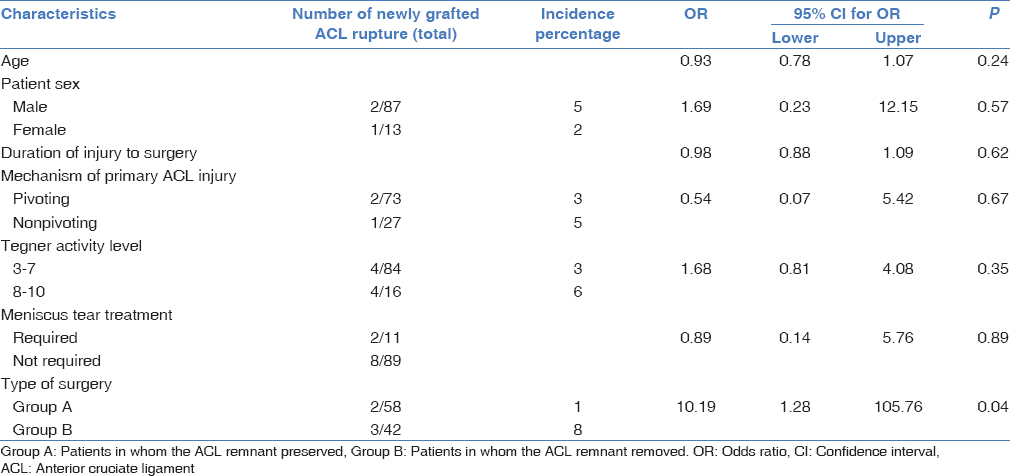
During knee arthroscopy, ACL remnant was noted in 100 of 131 (76%) patients, with the ACL site of femoral attachment that was entirely empty in the other 26 patients (19%). The remnant was preserved as much as possible, but it was not possible in all patients, and incomplete preservation was achieved in 31 of 131 patients (23%). In the present study, none of the patients had a major cartilage injury requiring an additional surgical procedure. After ACL reconstruction, there were no remarkable differences in either group with regard to Tegner score change on return to sports activity (0.21 ± 0.6 vs. 0.24 ± 0.6 points) and negative ratio on the pivot-shift test (85% vs. 89%). Anterior laxity of the knee, as measured by the KT-2000 arthrometer, was significantly better in Group A than in Group B (1.0 ± 0.7 vs. 1.4 ± 1.2 mm, P <.05). In Groups A and B, a side-to-side difference of ≥3 mm was observed in 3% and 5% of patients, respectively. The difference was ≥5 mm in 1% of the patients in Group B compared with none in Group A. In the present study, 6 of the 100 patients (6%) sustained an ACL graft rupture during follow-up, including 2 of 50 patients (4%) in Group A and 4 of 50 (8%) in Group B (P < 0.05). In contralateral knee, ACL ruptures occurred in 9 patients (18%) in Group A and 7 (14%) in Group B (P > 0.05) [Table 2]. Finally, regression analysis was done, which showed that the presence of the remnant was an important and significant predictor of nonrupture of a graft (odds ratio, 11.4; 95% CI, 1.2–99.6). Other variables, such as age, sex, time since injury to surgery, mechanism of ACL tear, meniscal tear and its management, and postoperative Tegner activity level, were not important indicators of ACL graft rupture [Table 3].

Out of 100 patients, 1 patient developed postoperative infection which was managed by arthroscopic debridement and antibiotics that subsided after 3 weeks. Two patients developed DVT after 7 postoperative days which was treated with subcutaneous LMWH and was recovered. Ninety-seven out of 100 patients improved without any complication and showed negative Lachman, anterior drawer, and pivot-shift tests at the end of 2, 4, and finally at 5 years. However, Group B patients still had the feeling of giving way at the end of 1 year even though there was no ACL laxity and also had 1–2 cm wasting of the quadriceps muscle despite supervised physiotherapy.
Discussion
ACL reconstruction with ACL remnant preservation has been found to give good results. However, the amount and requirement to preserve remnant tissues at the time of reconstruction were not evaluated, and not much data are available in the present literature because little is known about the quantity and quality of the remnant after surgery.
In our study, we treated ACL tear using standard methods of ACL reconstruction with and without preservation of the femoral and tibial ACL stumps. Many clinical studies have proved the benefit of remnant preservation in ACL reconstruction. Recently published data from two different authors indicate that there is no sufficient evidence to support the additional advantage of remnant-preserving reconstruction techniques as compared with total removal of the stump.[10,11] Wu et al., in their study, noted that the importance of continuous ACL remnant when present, its preservation improves many things like vascularization of the grafted ACL, ligamentization, tendon-to-bone attachment, integration, and proprioceptive function.[11] Many authors also noted such improvement with isolated tibial stump preservation in cases where no continuous remnant was present.[2,3] Bali et al. showed that the normal mechanoreceptors are present in both femoral and tibial ACL stumps which were confirmed by histopathological examination during ACL reconstruction.[12] In the year 2013, Sun et al., in an animal, showed that the ACL stump on the tibial side helps in vascularization and blood flow in the ACL graft.[13] Another study done by the same author showed that the ACL stump has potential to increase tendon-to-bone integration, ligamentization and gives biomechanical strength to the new graft as compared to complete removal in a rabbit model. In today's era of tissue preservation, it has been discussed time and again to preserves the tissue as much possible whether it is bone, cartilage, or meniscus. Keeping the same view, we thought whether preservation of ACL stump could help after ACL reconstruction in any way. At this point in time, we are not accepting or refuting its role. To reach on definite conclusion, we need large randomized control trials on this subject.
Many studies have reported that human ACL remnants have a cellular and vascular capacity for healing provided by the synovial layer histologically.[14,15,16] In vitro studies done by Deie et al.[16] have reported that there is the intrinsic healing potential in ACL of the human and has the ability to synthesize collagen. Many studies have shown in goats and sheep that the partial tear of ACL or complete tears has native ACL like healing capacity.[17,18,19]
Murray et al.[15] have noted in their study that tendon graft used in ACL reconstruction acts as a biological platform for synovialization and ACL healing which improved clinical results. Lee at al.[20] have reported better clinical results for patients with extensive synovial coverage over graft in a second look arthroscopy study. Ihara et al.[21] demonstrated that the presence of a ACL tibial remnant and its posttraumatic attachment (scarring) to the intercondylar roof or with the lateral wall of the femoral lateral condyle reduces anterior laxity significantly as supported by many studies.[22,23]
While attempting to preserve the femoral and tibial ACL, stumps may compromise the placement of guide at ACL footprint. In our technique, we elevated the available ACL remnant with the help of sharp periosteum elevator, shaver, and leaving it attached at the back, and then, the femoral tunnel was made. On the tibial side, the tunnel is made through the ACL remnant center itself. On the other hand, where continuous ACL remnant was present, we did not shave them off rather new ACL was placed along with them keeping in mind that there was no impingement. In our method of ACL stump, preservation on the tibial and femoral sides does not compromise the visualization of ACL footprint. A similar method of ACL stump elevation from the femoral side was used by a few authors.[24,25]
However, another important and potential concern with preserving both tibial and femoral ACL stumps is chances of graft impingement in the notch. Gohil et al.[26] observed cyclops formation in 59% cases after ACL reconstruction with marginal debridement of tissue in the notch compared to 37.5% in patients with aggressive debridement. We inspect the knee after completion of ACL reconstruction and checked for impingement through a complete range of motion. If the same was present, some parts of ACL remnant were removed. There was no patient where bony notchplasty was required to be done.
Yasuda, in 2012, reported a good result in a double-bundle reconstruction of ACL with remnant preservation, by making four tunnels at the attachment of the ACL remnant.[27] A study by Ochi et al., who noted that in a double-bundle ACL reconstruction with remnant preservation notchplasty is required to avoid impingement of the reconstructed ACL graft.[3] Ochi, in his study, recommended passage of ACL graft through the substance of ACL remnant using a curved hemostat. However, double-bundle reconstruction has been associated with a risk of damaging of the torn ACL remnant attachment and the ACL footprint.[15,16] Gohil et al. recommended very less debridement of the residual stump of the torn ACL that results in earlier revascularization of ACL reconstruction.[26]
Muneta et al. showed that the preoperative condition and postoperative outcome have been different depending on the amount of remnant left and also suggested that the amount of remnant may be an important preoperative condition and an indicator of better operative outcome.[28]
There is a constant debate in the present literature about how much ACL remnant is sufficient and how much delay between the initial injury and ACL reconstruction remains an issue. Panisset et al.[29] in their study examined the scar design of 418 ACL tears on MRI and also by arthroscopy and observed that there is a retraction of the torn ACL tibial remnant depending on the delay between injury and ACL reconstruction.
Murray et al.[15] have suggested that the few weeks postinjury will be the most suitable delay for ACL reconstruction because vascular, synovial, and cell proliferation occurs during this phase. ACL reconstruction can be delayed only if no associated significant meniscus tear.
We excluded 31 patients from the study where remnant was not present in the postoperative evaluation. Based on our study, we suggest that the remnant volume might be an important factor for better clinical outcome.
Few studies compared the clinical outcome between ACL reconstructions with and without a preservation of the remaining stump, mainly tibial remnant because mechanoreceptors reside mainly in the tibial attachment.[1,6] In the present study, we emphasized not only on the role of mechanoreceptors but also on the vascularity and continuity of the remnant tissue. Many authors reported no substantial difference in clinical laxity (Lachman and pivot-shift tests) between ACL reconstructions with and without a preserved torn remnant, but they noted a significant difference in proprioception and functional outcome.[1,2,5,12,26] Based on an arthrometer, we observed that an anterior stability of the knee was substantially improved in patients with ACL preserved remnant group.
Moreover, in our study, we usually performed ACL reconstructions after 4 weeks since injury because before 4 weeks, the ACL stump is still in the inflammatory phase and extremely soft. We also noted a bulging of the synovial sleeve at the tibial insertion of the ACL graft which can cause impingement and loss of full extension of the knee. In such situation, the stump has to be debrided or fixed to the tibial part of ACL graft. With this observation, we may suggest ACL reconstruction after 3 weeks from initial injury. This is also supported by Murray et al.[15] who described this period as Phases 2 and 3 of posttraumatic ACL inflammatory phase. However, much delay for several months after the injury leads to resorption and retraction of ACL remnant which will not qualify for preservation any more.[17,24,29] In such a case, only scarifying of ACL remnant will be required, as their preservation does not play any role.
The present study could not find whether the difference in the results in both the groups depends on the amount of remnant present. Our findings suggested that preservation of more than 75% of a remnant contributed to ACL stability.
Limitation of the study
The present study had few limitations. First, the 5-year follow-up period was relatively insufficient, although longer follow-up periods may bring out additional clinical outcome. Second, all three authors in this study performed intraoperative observations during ACL reconstruction involving remnant preservation. However, all the surgeons in this study had more than 10 years of experience in ACL reconstruction surgery. Third, the definition of preservation of the remnant was not quantitative or objective, rather it was subjective, and thus, there may be an inherent selection bias in dividing the patients into two groups.
Since it was difficult to be objectively quantified the remnant left. We need further studies based on the quality and quantity of the remnant preoperative. Finally, we did not evaluate the graft remodeling process or proprioception in analyzing the morphology and function of the remnant. Despite these limitations, however, the present study shows several benefits in preserving the ACL remnant tissue.
Conclusion
In our study, most ACL reconstructions were carried out after 2 months of initial injury, when the acute phase was over, and at that time, the quality of this soft tissue overlying the medial wall of lateral femoral condyle is thin and tends to elevate or detached easily.
Based on our study and also supported by the review of the literature, we hypothesize that the preservation of the tibial and femoral ACL stumps improves graft vascularization, and ligamentization and improved overall function of the knee as compared to those where ACL remnant has been removed completely, although there was no substantial difference in the ACL laxity in any group.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Comparison of clinical results according to amount of preserved remnant in arthroscopic anterior cruciate ligament reconstruction using quadrupled hamstring graft. Arthroscopy. 2008;24:560-8.
- [CrossRef] [PubMed] [Google Scholar]
- The anterior cruciate ligament remnant: To leave it or not? Arthroscopy. 2013;29:1253-62.
- [CrossRef] [PubMed] [Google Scholar]
- Double bundle arthroscopic anterior cruciate ligament reconstruction with remnant preserving technique using a hamstring autograft. Sports Med Arthrosc Rehabil Ther Technol. 2011;3:30.
- [CrossRef] [PubMed] [Google Scholar]
- Intra-articular cruciate reconstruction: I: Perspectives on graft strength, vascularization, and immediate motion after replacement. Clin Orthop Relat Res®. 1983;172:71-7.
- [CrossRef] [Google Scholar]
- Mechanoreceptors in the human anterior cruciate ligament. Anat Rec. 1986;214:204-9.
- [CrossRef] [PubMed] [Google Scholar]
- Neuroreceptors in the tissues of the knee joint. J Electromyogr Kinesiol. 1991;1:148-57.
- [CrossRef] [PubMed] [Google Scholar]
- The presence of proprioceptive mechanoreceptors in the remnants of the ruptured ACL as a possible source of re-innervation of the ACL autograft. Knee Surg Sports Traumatol Arthrosc. 2001;9:364-8.
- [CrossRef] [PubMed] [Google Scholar]
- Immunohistochemical study of mechanoreceptors in the tibial remnant of the ruptured anterior cruciate ligament in human knees. Knee Surg Sports Traumatol Arthrosc. 2009;17:1095-101.
- [CrossRef] [PubMed] [Google Scholar]
- Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res (198):43-9.
- [CrossRef] [Google Scholar]
- Sparing the anterior cruciate ligament remnant: Is it worth the hassle? Br Med Bull. 2012;104:91-111.
- [CrossRef] [PubMed] [Google Scholar]
- Preservation of remnant attachment improves graft healing in a rabbit model of anterior cruciate ligament reconstruction. Arthroscopy. 2013;29:1362-71.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of immunohistological methods in detecting functionally viable mechanoreceptors in the remnant stumps of injured anterior cruciate ligaments and its clinical importance. Knee Surg Sports Traumatol Arthrosc. 2012;20:75-80.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of graft healing in anterior cruciate ligament reconstruction with and without a preserved remnant in rabbits. Knee. 2013;20:537-44.
- [CrossRef] [PubMed] [Google Scholar]
- Revascularization of a human anterior cruciate ligament graft during the first two years of implantation. Am J Sports Med. 1995;23:42-9.
- [CrossRef] [PubMed] [Google Scholar]
- Histological changes in the human anterior cruciate ligament after rupture. J Bone Joint Surg Am. 2000;82:1387-97.
- [CrossRef] [PubMed] [Google Scholar]
- High intrinsic healing potential of human anterior cruciate ligament. Organ culture experiments. Acta Orthop Scand. 1995;66:28-32.
- [CrossRef] [PubMed] [Google Scholar]
- Acutely repaired proximal anterior cruciate ligament ruptures in sheep - by augmentation improved stability and reduction of cartilage damage J Mat Sci Mater Med. 1997;8:855-9.
- [CrossRef] [PubMed]
- The long-term biomechanical and viscoelastic performance of repairing anterior cruciate ligament after hemitransection injury in a goat model Am J Sports Med. 1996;24:109-17.
- [CrossRef] [PubMed]
- Histological evaluation of the healing potential of the anterior cruciate ligament by means of augmented and non-augmented repair: An in vivo animal study. Knee Surg Sports Traumatol Arthrosc. 2008;16:1087-93.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of clinical results and second-look arthroscopy findings after arthroscopic anterior cruciate ligament reconstruction using three different types of grafts. Arthroscopy. 2010;26:41-9.
- [CrossRef] [PubMed] [Google Scholar]
- MRI of anterior cruciate ligament healing. J Comput Assist Tomogr. 1996;20:317-21.
- [CrossRef] [PubMed] [Google Scholar]
- A modeling study of partial ACL injury: Simulated KT-2000 arthrometer tests. J Biomech Eng. 2002;124:294-301.
- [CrossRef] [PubMed] [Google Scholar]
- Spontaneous healing of acute anterior cruciate ligament (ACL) injuries- conservative treatment using an extension block soft brace without anterior stabilization Arch Orthop Trauma Surg. 2002;122:212-6.
- [CrossRef] [PubMed]
- Arthroscopic identification of isolated tear of the posterolateral bundle of the anterior cruciate ligament. Arthroscopy. 2009;25:728-32.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior cruciate ligament reconstruction with preservation of femoral anterior cruciate ligament stump. Arthrosc Tech. 2014;3:e575-7.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior cruciate ligament reconstruction using autologous double hamstrings: A comparison of standard versus minimal debridement techniques using MRI to assess revascularisation. A randomised prospective study with a one-year follow-up. J Bone Joint Surg Br. 2007;89:1165-71.
- [CrossRef] [PubMed] [Google Scholar]
- A pilot study of anatomic double-bundle anterior cruciate ligament reconstruction with ligament remnant tissue preservation. Arthroscopy. 2012;28:343-53.
- [CrossRef] [PubMed] [Google Scholar]
- Remnant volume of anterior cruciate ligament correlates preoperative patients' status and postoperative outcome. Knee Surg Sports Traumatol Arthrosc. 2013;21:906-13.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical, radiological and arthroscopic analysis of the ACL tear. A prospective study of 418 cases. Rev Chir Orthop Reparatrice Appar Mot. 2008;94:362-8.
- [CrossRef] [PubMed] [Google Scholar]




