
Translate this page into:
The role of 3-D printed models in planning and resection of heterotopic ossification around the elbow: A case series
Address for correspondence: Dr. Praharsha Mulpur, PG Road, Opposite Parsi Dharamsala, Paradise, Secunderabad - 500 003, Telangana, India. E-mail: praharshamulpur9@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Maryada VR, Mulpur P, Joseph VM, Guravareddy AV. The role of 3-D printed models in planning and resection of heterotopic ossification around the elbow: A case series. J Orthop Spine 2021;9:46-50.
Abstract
BACKGROUND:
Heterotopic ossification (HO) is a concern after elbow trauma and is associated with significant limitation of movement. Although complete restoration of elbow movement is seldom possible even by surgical resection, it improves functional range of movement and quality of life. Surgical excision of HO requires meticulous preoperative planning to minimize complications such as inadequate resection, and neurovascular complications. Life size models printed with three-dimensional (3D) printing technology help in understanding the complex HO mass and its relation to neurovascular structures, thereby helping in better preoperative planning.
AIM:
The aim is to study the usefulness of 3D-printed patient-specific models in resection of heterotrophic ossification around elbow
MATERIALS AND METHODS:
The 3D models are printed using computed tomography scans by FDM technology. Surgical approaches were planned based on the dimensions and extent of the HO mass in the 3D model. Resection was performed as planned and the sterilized 3D model was also used during surgery as anatomical reference. All patients had a minimum follow-up of 1 year. They were evaluated for improvement in elbow range of motion and complications.
RESULTS:
Six patients underwent surgical excision of HO of the elbow, with preoperative planning using 3D-printed models. A functional range of movement was achieved in all patients. There were neurovascular complications in this case series.
CONCLUSION:
3D-printed models are accurate and provide a replica of the patient-specific abnormal heterotopic ossification. 3D models provide excellent anatomical reference in planning excision by providing good orientation of the mass, dimensions, extent, and relation to neurovascular structures.
Keywords
Elbow trauma
excision
heterotopic ossification
planning
stiffness
three-dimensional printing
trauma

Introduction
Heterotopic ossification (HO) refers to mature lamellar bone formation in extraosseous tissue. There are various factors believed to be the cause of HO including direct injury, thermal burns, or head injury.[1] The elbow is a common site for HO and is associated with stiffness which significantly affects the activities of daily living.
The actual incidence may be under-reported as it is a self-limiting pathology.[2] The surgical treatment is based on the severity of stiffness and loss of function. Due to altered anatomy and impingement of HO mass on local neurovascular structures, there is an increased possibility of neurovascular injury during surgery.[3] Although the complete restoration of elbow movement is not possible even by surgical resection, it has been proven to give modest improvement in range of motion (ROM) and better functional outcome scores.[3,4,5]
Each of these cases is challenge to surgeon due to patient-specific abnormal anatomy. Appreciation of this abnormality on plain radiographs and even three-dimensional (3D) computed tomography (CT) images is incomplete as these 3D renderings are still seen on a 2D screen. Anatomically, accurate 3D-printed models provide both visual and tactile reproduction of the abnormal bony mass and its anatomic relations thereby helps in better preoperative planning. In addition, these life size models offer the advantage of reference during all stages of excision as HO has to be meticulously resected piece by piece checking the range of movements and avoiding neurovascular injury.
Contrary to popular belief, the cost of 3D printing is not prohibitive and since the CT scan with 3D reconstruction is almost routinely done in preoperative planning, it does not add up significantly on the expenditure. Our literature search yielded very few published articles on surgical management of HO and only one report on the use of stereolithographic 3D polymer models for heterotopic mass excision.[6] This small case series reports the benefits of a 3D-printed model in planning the surgical excision of HO of the elbow.
Materials and Methods
This study was a prospective observational study to assess the accuracy of 3D-printed models of elbows with HO mass, with 3D models used in preoperative planning of the excision procedure. All patients were consented prior to usage of radiological data. There was no requirement of certification from the institutional ethics board.
A total of 6 cases of HO of the elbow were treated at a tertiary center, with preoperative planning with 3D-printed models of the elbow. All patients had HO of more than 1-year duration and were clinically quiescent. All patients had CT scan of elbow with 0.625 mm thick slices using Siemens SomatomTM PerspectiveTM (Siemens Healthineers) 64-slice CT scan system.
Digital Imaging and Communication in Medicine files were imported and 3D representation of the bone models was generated using InVesaliusTM Software, (version 3.0.0. beta 5 software, Centre for Information Technology Renato Archer, Campinas, SP, Brazil). The data were then converted to STL (standard tessellation language) file format. The STL files were cleaned using Mesh Laboratory Software – advanced 3D mesh processing software, (MeshLab version 1.1.0, ISTI-CNR) and individual STL files were made. From STL files 3D models were printed using FlashForgeTM Dreamer 3D printer (FlashForgeDreamer-Dual Extruder) with 1.75 mm acrylonitrile butadiene styrene plastic filament. Slic3r slice engine (Open Source 3D printing Software) was used with standard resolution (layer height 0.2 mm, shells 3, infill 20%, print speed 60 mm/s, travel speed 80 mm/s, extruder temperature 230°C, and platform temperature 110°C).
All the patients were operated by a single Consultant Upper Extremity surgeon. The 3D-printed models were used preoperatively to understand the amount of HO and its relationship of important neurovascular structures around the elbow, to plan the amount of excision. The 3D model was sterilized with ethylene oxide and was used as an anatomical reference during surgery [Figure 1].
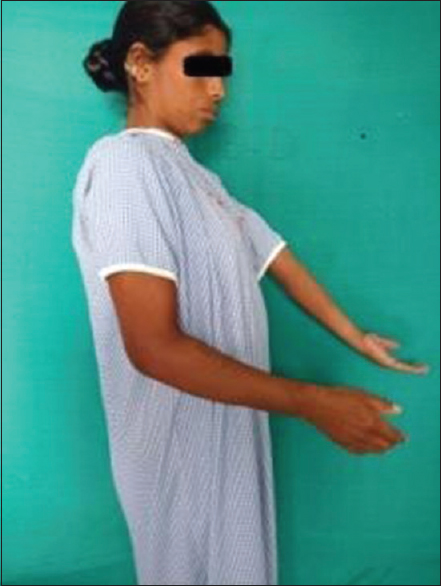
- Preoperative clinical Image of patient with ankylosed elbow
Case example
The illustrated case [Figures 1–4] is a 40-year-old homemaker, who met with a road traffic accident, resulting in direct injury to her elbow. The initial trauma was managed conservatively with closed reduction and casting. The plaster cast was removed after 6 weeks and ROM exercises were started. She complained of painful and progressive reduction in ROM over a period of 1 year. When she presented to us, her main complaint was painless restriction of ROM, with the elbow ankylosed in 30° of flexion [Figure 1]. On clinical examination, there were no signs of inflammation, diffuse swelling without tenderness, irregular and widened metaphyseal margins. She was evaluated with plain radiography of the elbow, which revealed HO mass around the elbow [Figure 2]. She was further evaluated with CT scans and an anatomical model of the affected elbow was printed using 3D printing technology [Figure 3a and Figure 3b].

- Preoperative radiograph showing heterotopic ossification around the elbow
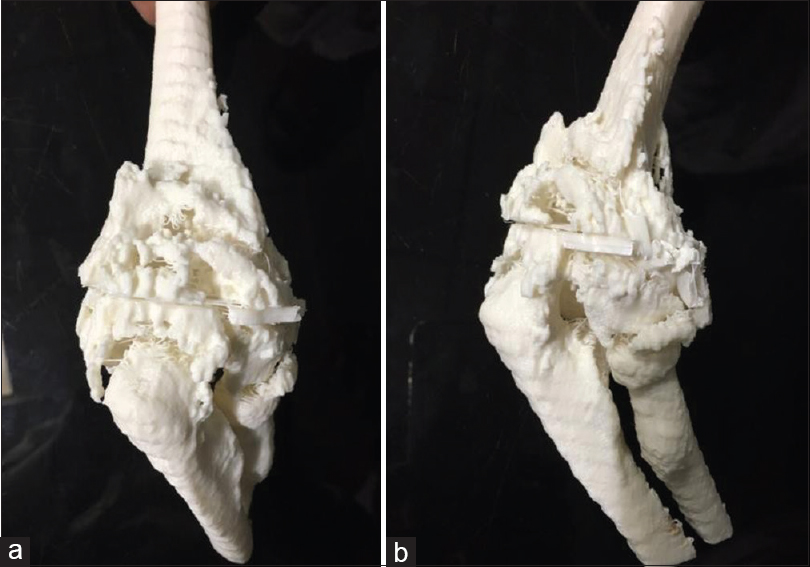
- (a) Computed tomography -scan based three-dimensional-printed model of elbow with heterotopic ossification mass (viewed from front). (b) Computed tomography-scan-based three-dimensional-printed model of elbow with heterotopic ossification mass (viewed from the side)
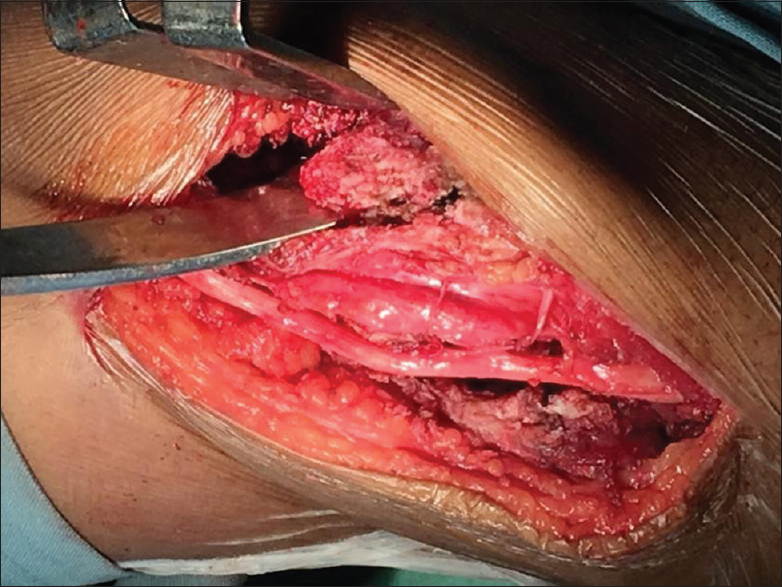
- Intraoperative photograph showing resection of mass with the ulnar nerve protected
Surgical technique
Based on the anatomical 3D model, meticulous planning was done keeping the neurovascular structures in mind. Approaches used were the direct posterior, posterolateral, and posteromedial to the elbow. The choice of incision and approach were decided based on which approach gave maximal exposure and allowed maximal excision of the HO mass. Whenever necessary, the models were used as reference during surgery to avoid injury to neurovascular structure and to correlate with our findings on the image intensifier. Resection of the mass was done as planned preoperatively on the model, avoiding the ulnar nerve [Figure 4]. After mass excision, under anesthesia, all elbow movements were assessed and the improvement in the ROM was noted. The active and assisted ROM exercises were started on the first postoperative day with appropriate analgesia. Adjuvant Medical management including indomethacin prophylaxis against recurrence and celecoxib was given to all the patients postoperatively.
Results
A functional range of elbow motion was achieved in all 6 patients who underwent HO mass excision. A case example with preoperative [Figure 1] and postoperative clinical picture at 1-year of follow-up [Figure 5] are illustrated. Functional ROM of the elbow was defined as 75°-–120° of flexion by Vasen et al.[7] The patients were able to perform all the activities of daily life including overhead activities with regular physical therapy [Figure 5].

- Clinical photograph on follow-up showing functional elbow range of motion
Patients were followed up at 3 months, 6 months, and 1 year from surgery to assess active pain-free ROM at elbow and serial radiographs to rule out HO recurrence. In 3 patients at 3-months' follow-up, there was a mild decrease in ROM as compared to the gains noted intraoperatively. However, these reductions were nonprogressive. Two patients had restriction of supination, which was achieved intraoperatively. Two of the three patients with mild reduction in ROM at 3 months of follow-up had radiographic evidence of recurrence of ectopic bone formation around the elbow at 3 months' postsurgery [Table 1].
| Patient number | Preoperative ROM (degrees) | Intraoperative ROM achieved (degrees) | 3 months follow-up (degrees) | 6 months follow-up (degrees) | 12 months follow-up (degrees) |
|---|---|---|---|---|---|
| 1 | 20-40 | 20-90 | 20-90 | 30-90 | 30-90 |
| 2 | Ankylosed at 30 | 0-90 | 0-90 | 10-90 | 10-90 |
| 3 | 10-35 | 10-90 | 10-90 | 30-90 | 30-90 |
| 4 | 30-45 | 10-100 | 10-100 | 10-90 | 10-90 |
| 5 | 10-30 | 10-90 | 10-90 | 10-90 | 10-90 |
| 6 | Ankylosed at 30 | 10-90 | 10-90 | 10-80 | 10-80 |
ROM: Range of motion
In all cases, the 3D-printed model of HO mass was identical to the intraoperative findings after complete exposure, and dimensions calculated from bony landmarks was accurate and same.
Discussion
The incidence of HO around the elbow following trauma can be as high as 49%.[8] The normal functional arc of movement of the elbow is 100 degrees and any impairment in this can result in difficulty in performing daily activities.[9] Starting from the pathophysiology, there is no clarity regarding treatment and the various causes of complications or poor functional outcomes.[10,11] This makes the decision of surgical management challenging. Although complete recovery of range of movement is seldom possible surgical resection gives functional range of movement and best a functional outcome. Surgical management is not without complications such as recurrence, neurovascular injury, stiffness, or even complete ankylosis.[12,13]
Meticulous preoperative planning is essential for successful outcomes. No two cases of HO are similar and the abnormal bone mass is patient specific. Patient-specific treatment plans have to be devised based on the heterotopic mass and its relation to important neurovascular structures. Although CT scan and 3D CT images are helpful in understanding the abnormal bone anatomy, they are still 2D representations of a 3D pathology. 3D printing is a promising technology that offers benefits in planning surgery in cases with altered anatomy. Life-size OR anatomical 3D models printed by 3D printing have been widely used in complex THR, revision THR, and complex acetabular fractures. The aim of our study was to assess the benefits of this novel technology in the planning of surgical resection of HO of the elbow. All patients had preoperative clinical examination and radiographs and CT scan to know the extent of heterotopic mass. 3D model was made in all cases and excision was planned based on the model. The models are also used as intraoperative reference guide while excising the mass, rather than the usual trial and error method of excising the mass. All the six patients included in our study attained a painless functional range of movement with negligible complications and the attained movement was retained in up to 1 year of follow-up. The use of 3D printing was useful for surgical planning and also served as a motivation for the patients in physical therapy.
We were able to plan the procedure and account for the spatial orientation of neurovascular structures in proximity to the HO mass. There were no neurovascular complications in any patient. Fleming et al.[6] also reported increased surgeon orientation and comfort in performing the surgery with the help of stereolithographic polymer models, which helped guide the surgical approach and tissue dissection.
Our study has some limitations. First, this is a case series and the sample size is small. A larger sample size with varying pathologies of the elbow is required to understand the benefits of 3D printing technology. Second, this was not a randomized study. A prospective comparison study can be done in the future with and without the use of 3D printing technology, to evaluate differences in parameters such as surgeon comfort, operative time, blood loss, and functional outcomes. Third, this is only a case series and we cannot attribute outcomes to the use of 3D models in the preoperative planning stage.
Conclusion
3D models are helpful in preoperative planning and can also be used as reference during surgery. HO is patient specific and understanding the ossification in 3 dimensions and its relation to neurovascular structures is important in planning excision. 3D-printed models are accurate and provide a replica of the patient-specific abnormal heterotrophic ossification. In this case series, we found that preoperative 3D models provide excellent anatomical reference in planning excision by providing good orientation of the mass, dimensions, extent, and relation to neurovascular structures.
Informed consent
Informed consent was obtained from all participants of the study. All patient data were anonymized.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understand that name and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Risk factors for development of heterotopic ossification of the elbow after fracture fixation. J Shoulder Elbow Surg. 2012;21:1550-4.
- [CrossRef] [PubMed] [Google Scholar]
- Heterotopic ossification of the elbow. J Shoulder Elbow Surg. 1997;6:321-32.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical resection of heterotopic bone about the elbow: An institutional experience with traumatic and neurologic etiologies. J Hand Surg Am. 2011;36:798-803.
- [CrossRef] [PubMed] [Google Scholar]
- Resection of heterotopic ossification of the elbow: A comparison of ankylosis and partial restriction. J Hand Surg Am. 2010;35:1115-9.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical approaches for nonneurogenic elbow heterotopic ossification with ulnar neuropathy. J Trauma. 2002;53:928-33.
- [CrossRef] [PubMed] [Google Scholar]
- Use of 3-dimensional stereolithographic polymer models for heterotopic ossification surgical excision. Orthopedics. 2013;36:282-6.
- [CrossRef] [PubMed] [Google Scholar]
- Functional range of motion of the elbow. J Hand Surg Am. 1995;20:288-92.
- [CrossRef] [PubMed] [Google Scholar]
- Incidence and risk factors of heterotopic ossification following major elbow trauma. Orthopedics. 2012;35:e815-22.
- [CrossRef] [PubMed] [Google Scholar]
- A biomechanical study of normal functional elbow motion. J Bone Joint Surg Am. 1981;63:872-7.
- [CrossRef] [Google Scholar]
- Early excision and late excision of heterotopic ossification after traumatic brain injury are equivalent: A systematic review of the literature. J Neurotrauma. 2007;24:1675-86.
- [CrossRef] [PubMed] [Google Scholar]
- The time point in surgical excision of heterotopic ossification of post-traumatic stiff elbow: Recommendation for early excision followed by early exercise. J Shoulder Elbow Surg. 2015;24:1165-71.
- [CrossRef] [PubMed] [Google Scholar]
- Heterotopic ossification following combat-related trauma. J Bone Joint Surg Am (92 Suppl 2):74-89.
- [CrossRef] [PubMed] [Google Scholar]
- Heterotopic ossification of the elbow treated with surgical resection: Risk factors, bony ankylosis, and complications. Clin Orthop Relat Res. 2014;472:2269-75.
- [CrossRef] [PubMed] [Google Scholar]




