
Translate this page into:
The influence of referencing system on PCO and PCOR in primary total knee arthroplasty and its effect on postoperative range of motion and functional scores
Address for correspondence: Dr. Aditya P. Apte, Sunshine Hospitals, Hyderabad, Telangana, India. E-mail: dradityaapte@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Vecham R, Apte AP, Annapareddy A, Govinde Gowda SK, Chiranjeevi T, Reddy G. The influence of referencing system on PCO and PCOR in primary total knee arthroplasty and its effect on postoperative range of motion and functional scores. J Orthop Spine 2021;9:68-72.
Abstract
OBJECTIVE:
The restoration of native posterior condylar offset (PCO) is considered to be an integral component of a successful total knee arthroplasty (TKA). Its effect on postoperative flexion is still not clear. The two referencing systems viz. anterior and posterior differ in their basic philosophy for selecting the appropriately sized femoral component. In this study, we aimed to evaluate their effect on the PCO, posterior condylar offset ratio (PCOR), notching, and anterior flange bone contact ratio. We also evaluated the influence of referencing system on postoperative flexion and functional scores at 2-year follow-up.
MATERIALS AND METHODS:
This was a retrospective single-center, single-surgeon study. Total 200 primary TKA (100––anterior referencing [AR]; 100––posterior referencing [PR]) were evaluated. The PCO and PCOR were measured pre- and postoperatively. In addition, if the femoral component was not seated properly, anterior flange–bone contact ratio and the incidence of notching were documented as well.
RESULTS:
Postoperatively, the mean PCO increased to 3.24 and 3.04 from 2.90 and 2.85 in the PR and AR groups, respectively. The comparative increase in PR group was significant (P < 0.001). Likewise, the PCOR increased postoperatively in both the groups and the comparative increase in PR was significant (P < 0.00). However, the comparative increase in flexion was not significant (P = 0.72)
CONCLUSION:
PR system provides better contact between anterior flange and anterior cortex of the femur. It also led to a significant increase in PCO and PCOR postoperatively. However, this does not significantly influence the ROM and Oxford knee scores at 2-year follow-up.
Keywords
Notching
oxford knee scores
posterior condylar offset
posterior condylar offset ratio
referencing

Introduction
Accurate positioning of the femoral implant forms one of the cornerstones of total knee arthroplasty (TKA).[1] It influences the patellofemoral and tibiofemoral kinematics, which will influence postoperative stability, range of motion, and patellar tracking.[2]
Femur component sizing is determined by its native dimensions and balancing of the gaps. The ultimate goal is to match native dimensions as accurately as possible while gaining symmetrical flexion and extension gaps.[3]
The two referencing systems differ in their basic philosophy to achieve this goal. The anterior referencing (AR) system focuses on the anterior femoral cortex to prevent notching but can lead to inconsistent flexion gaps.[4] The posterior referencing (PR) system cuts a constant posterior femoral condyle to gain much more predictable flexion gaps. However, if not appropriately sized it can lead to notching.[4]
The primary aim of this study was to analyze how the posterior condylar offset (PCO) changed with both referencing systems. We also assessed each patient at the end of 2 years to calculate clinical improvement and functional scores.
Materials and Methods
This was a retrospective single-center, single-surgeon study. Total 200 primary cemented TKA (100––AR; 100––PR) performed from January 2016 to January 2018 were evaluated. This study was approved by the hospital Human Research and Ethics Committee.
Inclusion criteria
Patients with end-stage osteoarthritis requiring TKA with less than 20 degrees of deformity
Exclusion criteria
Complex TKA with extra-articular deformity
TKA done for inflammatory etiology
Surgical technique
Identical surgical technique except for the use of referencing system was used in all cases. The Depuy PFC sigma was used for AR and Smith and Nephew Genesis II was used for PR. Apart from standard medial soft tissue release none of the patients required any additional releases.
The following parameters were calculated pre- and postoperatively:
Posterior condylar offset
It is the distance between two tangents, which were drawn along the posterior cortex of the femur, and the posterior-most point of the condyles of the femur [Figure 1].
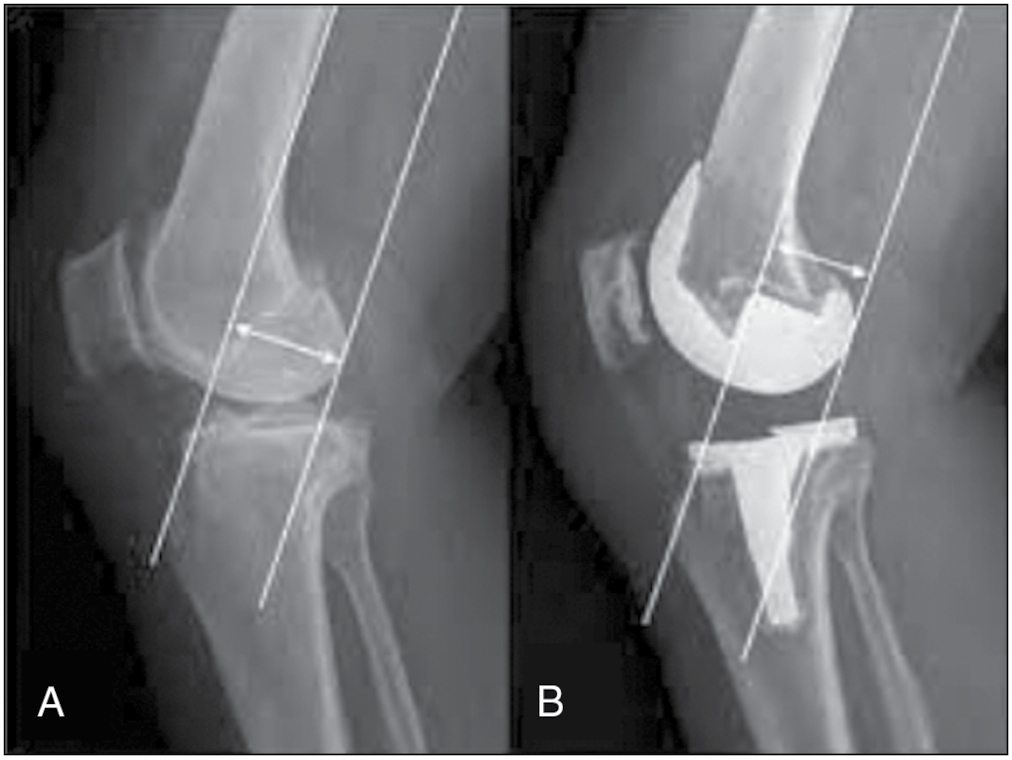
- Posterior condylar offset: Preoperative (A) and postoperative (B)
Posterior condylar offset ratio
It is the ratio of PCO (B) and the distance between tangent along the posterior condylar border and tangent of the anterior femoral cortex (A) [Figure 2].
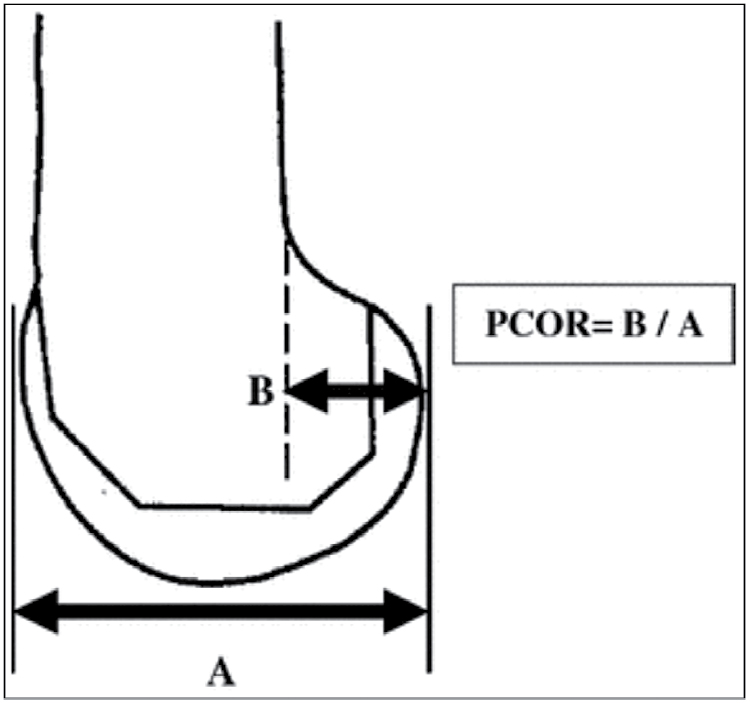
- Posterior condylar offset ratio
Notching
On the lateral radiographs, if the anterior femoral cortex breach is more than 1 mm.
Anterior flange bone contact ratio
It is the ratio of total anterior flange length and the length of contact of anterior flange with the anterior femoral cortex.
Results
Statistical analysis
The data were collected and compiled using Microsoft Excel. The analysis was done using Epi info, version 7.2 (CDC, Atlanta, Georgia). The qualitative variables were expressed in terms of percentages. The normality of the data was tested using the Kolmogorov–Smirnov test. Normal quantitative data were expressed in terms of mean and standard deviation. Nonnormal data were expressed in terms of median and interquartile range. To test the difference between the two means, Student's t test was used. To test the difference between two medians, Mann–Whitney U test was used, d. All the analysis was two-tailed and the significance level was set at 0.05 [Table 1].
| Depuy PFC(AR) | S/N genesis II(PR) | P Value (Btw groups) | |||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| PCO | |||||
| Preoperative | 2.85 | 0.27 | 2.90 | 0.29 | 0.1897 |
| Postoperative | 3.04 | 0.28 | 3.24 | 0.26 | <0.001 |
| PCOR | |||||
| Preoperative | 0.49 | 0.05 | 0.51 | 0.05 | 0.0261 |
| Postoperative | 0.54 | 0.04 | 0.57 | 0.06 | <0.00 |
Postoperatively, the mean PCO increased to 3.24 and 3.04 from 2.90 and 2.85 in the PR and AR groups, respectively. The comparative increase in PR group was significant (P < 0.001). Likewise, the PCOR increased postoperatively in both the groups and the comparative increase in PR was significant (P < 0.00) [Table 2].
| Depuy PFC (AR) | S/N genesis II (PR) | P Value (Btw groups) | |||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| AFBC ratio | 0.83 | 0.19 | 0.92 | 0.14 | 0.0001 |
The mean anterior flange–bone contact ratio was better in PR group and the difference was statistically significant [Table 3].
| Depuy PFC (AR) | S/N genesis II (PR) | P Value (Btw groups) | |||
|---|---|---|---|---|---|
| Mean/median | SD/IQR | Mean/median | SD/IQR | ||
| Change in flexion (%) | 5.26 | 4.76 to 8.24 | 5.26 | 2.19 to 10.00 | 0.7654 |
| Change in flexion (points) | 5 | 5 to 8 | 5 | 2 to 9.50 | 0.7290 |
At 2-year follow-up, the postoperative flexion in AR group increased by 5.26 ± 4.76(SD)%, whereas that in PR group increased by 5.26 ± 2.19 (SD)%. The comparative increase in flexion was not significant (P = 0.72) [Table 4].
| Depuy PFC (AR) | S/N genesis II (PR) | P Value (Btw groups) | |||
|---|---|---|---|---|---|
| Mean/median | SD/IQR | Mean/median | SD/IQR | ||
| Change in OKS (%) | 249.49 | 2720 | 24738 | 31.12 | 0.6098 |
| Change in OKS (Points) | 31.58 | 1.58 | 31.42 | 1.74 | 0.4960 |
Oxford knee scores were evaluated at 2-year follow-up. Although the scores increased in both the groups, the comparative analysis was nonsignificant (P = 0.60) [Table 5].
| Notching | Depuy PFC (AR) | S/N genesis II (PR) | P Value (Btw groups) | ||
|---|---|---|---|---|---|
| Nor | % | Nor | % | ||
| Yes | 1 | 1.00 | 3 | 3.00 | 0.7645 |
| No | 99 | 99 | 97 | 97 | |
One patient had notching in the AR group, whereas three had notching in the PR group. This difference was nonsignificant too (P = 0.76).
Discussion
The restoration of native PCO is considered an integral component of a successful TKA.[5] Its effect on postoperative flexion is still not clear. Bellemans et al.[5] proved that restoration of PCO was important to gain near-normal flexion. Inadequate PCO leads to impingement of the femoral component on the posterior part of polyethylene, restricting flexion.[6] Han and Kang[7] further cemented this theory and described the role of medial PCO in gaining knee flexion. Since then, multiple studies have been published to this effect and some of them have challenged this concept. Bauer et al.[8] published their case series of 410 knees where they reported an average increase in PCO postoperatively. However, this increase did not significantly affect the flexion range. Ishii et al.[9] similarly proved no correlation between PCO and knee flexion in their study.
We believe that the dynamics of PCO and PCOR are still not completely understood. The aim of this study was to further that cause. In this study, we observed a mean increase in postoperative PCO and PCOR in both the groups. The comparative analysis among the groups was significant proving that PR provided with a better PCO and PCOR postoperatively. These findings are consistent with the studies by Bauer et al..[8]
While using the AR system we tend to undersize the femur to get an optimal contact between anterior flange and anterior femoral cortex. This can lead to cutting additional bone on the posterior aspect. Thus, restoring the PCO becomes difficult.[9,10] In the PR system, we sometimes tend to oversize the femur to prevent notching. When the implant seated correctly on the anterior cortex, PR restores the PCO better.[10] This further reflected in the statistically significant increase in PCOR postoperatively. This increase in PCO, PCOR however did not correlate with flexion achieved and functional scores (OKS) at 2 years.
Multiple factors determine the postoperative flexion.[11] Preoperative range of flexion is the most important determinant of postoperative flexion.[12] Lower tibiofemoral deformity also correlates with a better range of motion.[13] Other factors affecting postoperative flexion are tibial slope, BMI, demographics, comorbidities, preoperative physiotherapy.[14,15,16,17,18] Degree of hip motion also has an effect on knee motion post arthroplasty.[19]
In our study, we did not find a correlation between increase in PCO, PCOR, and postoperative flexion and functional scores. Thus, proving that postoperative flexion is determined by an interplay of multiple factors.
The contact between anterior flange and anterior cortex is important as that determines strength of implant bone interface.[19] Inadequate contact between component and anterior cortex predisposes to anterior knee pain postoperatively as it overstuffs the patellofemoral joint space.[20] PR system provides better contact between anterior part of the component and anterior cortex.[21] We found similar results in our study.
One limitation of our study is that as no MRI studies were carried out; cartilage thickness was not determined. This could influence preoperative PCO measurements.[22] The use of different implants for AR and PR systems could influence PCO postoperatively.
PR system theoretically increases the risk of notching.[23] Although the incidence of notching in our study was more with PR, the difference was statistically nonsignificant.
Conclusion
PR system leads to a significant increase in PCO and PCOR as compared to its counterpart. This however did not influence flexion range and functional scores at 2-year follow-up.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- The effect of femoral component position on the kinematics of total knee arthroplasty. Clin Orthop Relat Res. 1993;286:122-9.
- [CrossRef] [Google Scholar]
- The effect of femoral component position on patellar tracking after total knee arthroplasty. Clin Orthop Relat Res. 1990;260:43-51.
- [CrossRef] [Google Scholar]
- Gap balancing in total knee arthroplasty. J Arthroplasty. 2006;21:11-5.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior referencing versus posterior referencing in total knee arthroplasty. J Knee Surg. 2014;27:303-8.
- [CrossRef] [PubMed] [Google Scholar]
- Fluoroscopic analysis of the kinematics of deep flexion in total knee arthroplasty. Influence of posterior condylar offset. J Bone Joint Surg Br. 2002;84:50-3.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanical effects of posterior condylar offset and posterior tibial slope on quadriceps force and joint contact forces in posterior-stabilized total knee arthroplasty. BioMed Res Int. 2017;2017:4908639.
- [CrossRef] [PubMed] [Google Scholar]
- Interactive effect of femoral posterior condylar offset and tibial posterior slope on knee flexion in posterior cruciate ligament-substituting total knee arthroplasty. Knee. 2018;25:335-40.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of posterior condylar offset on knee flexion after cruciate-sacrificing mobile-bearing total knee replacement: A prospective analysis of 410 consecutive cases. Knee. 2010;17:375-80.
- [CrossRef] [PubMed] [Google Scholar]
- Posterior condylar offset does not correlate with knee flexion after Tka. Clin Orthop Relat Res. 2013;471:2995-3001.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior referencing versus posterior referencing in total knee arthroplasty. J Knee Surg. 2014;27:303-8.
- [CrossRef] [PubMed] [Google Scholar]
- Factors affecting range of flexion after total knee arthroplasty. J Orthop Sci. 2001;6:248-52.
- [CrossRef] [PubMed] [Google Scholar]
- Does pre-operative flexion factor influence the postoperative range of motion in total knee arthroplasty. J Orthop Traumatol Rehabil. 2014;7:78-83.
- [CrossRef] [Google Scholar]
- Factors influencing range of motion after total knee arthroplasty. Iran Red Crescent Med J. 2012;14:417-21.
- [Google Scholar]
- Factors affecting postoperative flexion in total knee arthroplasty. Orthopedics. 1990;13:643-9.
- [CrossRef] [PubMed] [Google Scholar]
- Knee flexion after total knee arthroplasty. J Orthop Surg. 2002;10:194-202.
- [CrossRef] [PubMed] [Google Scholar]
- Factors affecting range of motion in total knee arthroplasty using high flexion prosthesis: A prospective study. Indian J Orthop. 2013;47:50-6.
- [CrossRef] [PubMed] [Google Scholar]
- The influence of tibial slope on maximal flexion after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2005;13:193-6.
- [CrossRef] [PubMed] [Google Scholar]
- Significant effect of the posterior tibial slope and medial/lateral ligament balance on knee flexion in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2013;21:2704-12.
- [CrossRef] [PubMed] [Google Scholar]
- Influence of preparation techniques to the strength of the bone-cement interface behind the flange in total knee arthroplasty. Knee. 2013;20:186-90.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior knee pain following primary total knee arthroplasty. World J Orthop. 2015;6:795-803.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of the referencing system on the posterior condylar offset and anterior flange-bone contact in posterior cruciate-substituting total knee arthroplasty. J Arthroplasty. 2018;33:1069-75.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis of tibiofemoral cartilage deformation in the posterior cruciate ligament-deficient knee. J Bone Joint Surg Am. 2009;91:167-75.
- [CrossRef] [PubMed] [Google Scholar]
- Notching of the anterior femoral cortex during total knee arthroplasty characteristics that increase local stresses. J Arthroplasty. 2006;21:737-43.
- [CrossRef] [PubMed] [Google Scholar]




