
Translate this page into:
Surgical treatment of recalcitrant lateral epicondylitis using a minimal incision technique
Address for correspondence: Dr. Nissar Ahmad Shah, Department of Orthopaedics, District Hospital Baramulla, Baramulla, Jammu and Kashmir, India. E-mail: shahnisar01@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Dar NA, Shah NA, Shah IA, Iqbal W. Surgical treatment of recalcitrant lateral epicondylitis using a minimal incision technique. J Orthop Allied Sci 2018;6:64-8.
Abstract
BACKGROUND:
Lateral epicondylitis responds well to conservative methods of treatment such as drugs, braces and local infiltration of steroids, autologous blood, and platelet-rich plasma. The patients who do not respond to conservative methods become candidates for surgical intervention. In our study, we have performed the Nirschl procedure through a smaller incision.
MATERIALS AND METHODS:
Our study included 18 patients having lateral epicondylitis treated with an open debridement of extensor carpi radialis brevis using a small incision. In our study, we had six males and 12 females, with 14 patients having involvement on the right side and four patients on the left side. Patients were followed up for a mean period of 28.8 months, and the final outcome was assessed using the QuickDASH score, visual analog scale (VAS), and the Nirschl and Pettrone's grading system.
RESULTS:
According to the QuickDASH scoring scale, the preoperative mean score improved from 74.4 to 49.7 postoperatively, which is statically significant (P < 0.05). According to the Nirschl and Pettrone's grading system, 14 (77.7%) cases were excellent, 3 (16.7%) were good, and 1 (5.6%) was fair and none had a failure. The mean VAS score for pain at rest improved from 4.7 (range from 3 to 6) preoperatively to 0.7 (range from 0 to 2) at the last follow-up (P < 0.05)). The mean VAS score during daily activities improved from 6.9 (range from 4 to 8) preoperatively to 1.2 (range from 0 to 2) at the last follow-up (P < 0.05).
CONCLUSION:
Surgical intervention via the Nirschl operative technique is ideal for recalcitrant lateral epicondylitis.
Keywords
Extensor Carpi Radialis Brevis
lateral epicondylitis
nirschl procedure

Introduction
Tennis elbow or lateral epicondylitis of the elbow is a common upper extremity disorder, which is characterized by degenerative changes in the musculotendinous region of the epicondyle, resulting from the repetitive stress of flexion and extension movements of the wrist joint.[1] The term epicondylitis is a misnomer, as there is little evidence to suggest that there is an inflammatory process. There are various treatment options for the condition including rest, physical therapy, drugs, braces, steroid injection therapy, and injection of autologous blood or platelet-rich plasma. However, the optimal treatment method remains an open question. Surgical treatment is required when conservative management has failed.[2,3]
Materials and Methods
The present study was conducted on 18 patients from 2012 to 2017 in the Department of Orthopedics of our hospital, who had recalcitrant lateral epicondylitis. All the patients were initially managed with conservatively with nonsteroidal anti-inflammatory drug, braces, and steroid injections. All patients were examined preoperatively. A detailed history and physical examination including a thorough neurological examination was done. The neurological examination was aimed to rule out any signs of nerve compression. The diagnosis was confirmed by resisted extension of the middle finger and pinch grip with the wrist in extension provoking pain over the common extensor region. The patients having acute infection in the surgical area, cervical radiculopathy involving C5, C6, and C7 nerve root, thoracic outlet syndrome, Frohse Arcade syndrome elbow instability, or any features of elbow arthritis were excluded from the study. There were 6 males and 12 females, with a mean age of 42 to 3 years (range from 28 to 55 years) and the mean duration of the symptoms was 17.6 months (range from 12 to 26 months). The right side (dominant) was involved in 14 patients and left side (nondominant) side in 4 patients. Statistical analysis was performed using paired t-test. P < 0.05 was considered statistically significant.
Operative technique
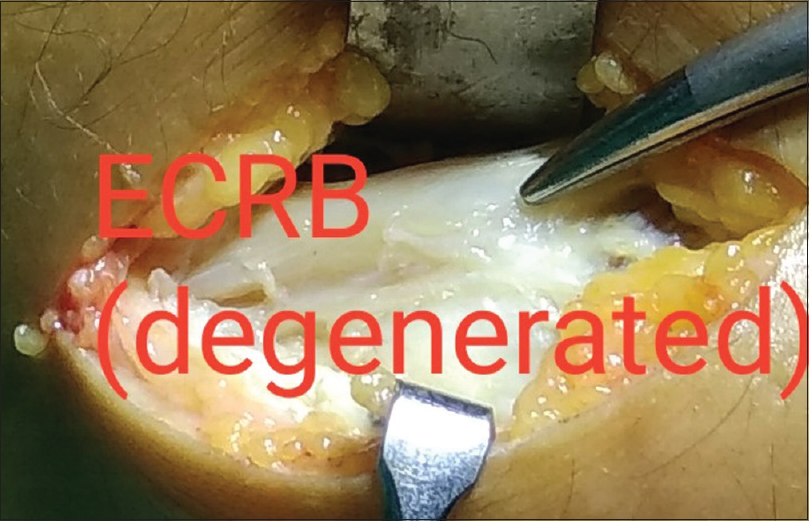
The procedures were all carried out under general anesthesia and tourniquet control by a single surgeon. The surgeon used the technique described by Nirschl[4] and Nirschl and Pettrone[5] but using a smaller(4–5 cm) incision [Figure 1]. The incision is centered over the common extensor origin, and extensor carpi radialis longus (ECRL) is reflected to expose the origin of extensor carpi radialis brevis (ECRB), and the damaged portion of the tendon is removed [Figures 2-5]. This is commonly found to be white and edematous. Few small drill holes are made in the lateral epicondyle. The ECRL, extensor digitorum communis, and edge of the ECRB are attached to the periosteum, followed by the closure of fascia and the skin [Figure 6]. The wound was dressed and the plaster slab was put for 2 weeks' duration, followed by the range of motion and strengthening exercises of the elbow joints along with wrist and shoulder joints.

- Incision for lateral epicondylitis (4 cm)
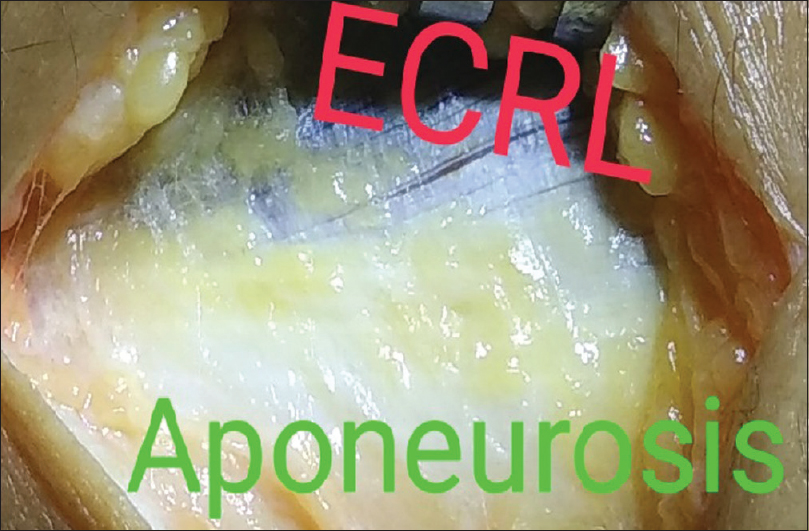
- Extensor carpi radialis longus and extensor aponeurosis exposed
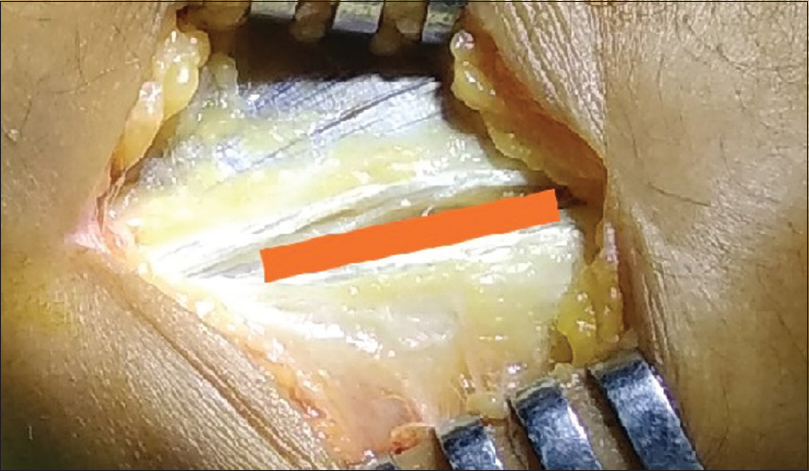
- Split between the extensor carpi radialis longus and aponeurosis
- Split between the extensor carpi radialis longus and aponeurosis

- Degenerated extensor carpi radialis brevis exposed
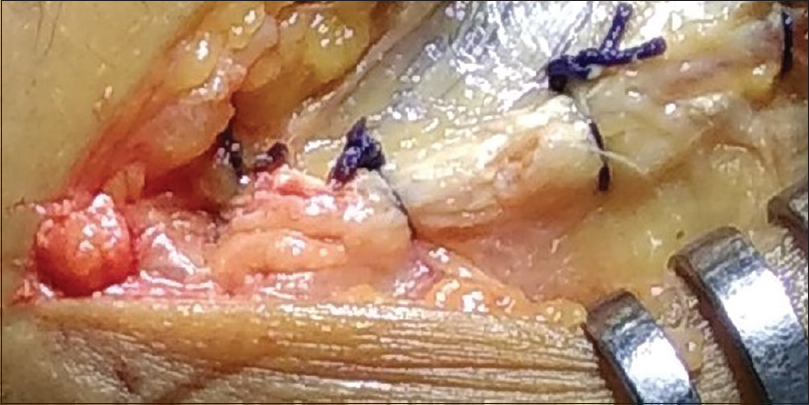
- Closure of the extensor carpi radialis longus and aponeurosis
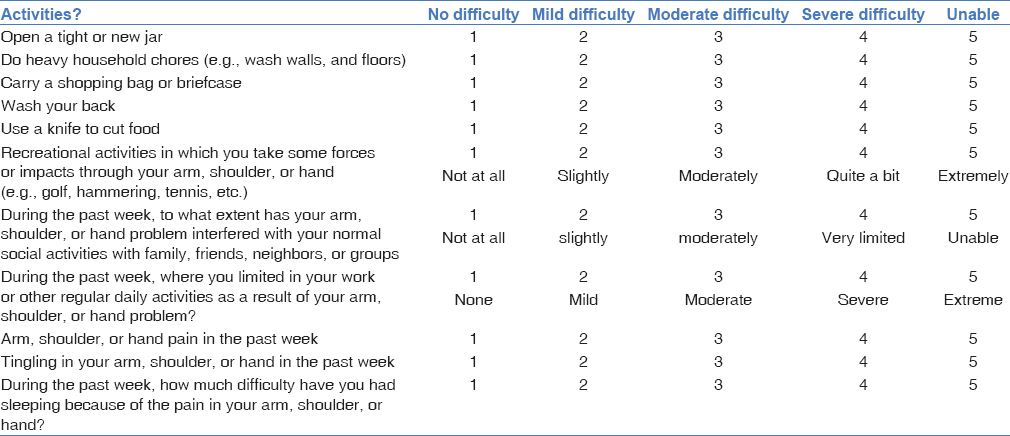
Clinical assessment
The pain and the function of the elbow joint before the treatment and after the treatment were assessed and recorded using the Quick Disabilities of the Arm, Shoulder, and Hand questionnaire (QuickDASH)[6] [Table 1], the Nirschl and Pettrone's grading system[5] [Table 2], and the visual analog scale (VAS) for pain. According to the Nirschl and Pettrone's grading system, excellent was defined as a full return to all activities without pain, good as a full return to all activities with occasional mild pain, fair as normal activity without pain, significant pain with heavy activity but an overall improvement in pain, and failure as no improvement in symptoms. Excellent and good results were considered satisfactory. VAS was utilized to record pain scores. If there was no pain, the score was 0 point and the most severe pain was recorded as 10 points. VAS was taken at rest and during routine activities.
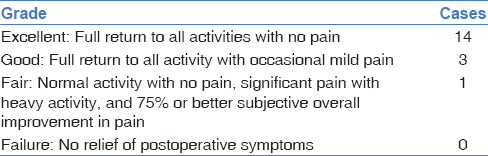
Results
The mean final follow-up of the 18 patients in our study was at 28.8 months (range from 8 to 54 months). According to the QuickDASH scoring scale, the preoperative mean score improved from 74.4 to 49.7 postoperatively, which is statistically significant (P < 0.05). According to the Nirschl and Pettrone's grading system, 14 (77.7%) cases were excellent, 3 (16.7%) were good, and 1 (5.6%) was fair and none had a failure. No postoperative complication such as instability was found. The mean VAS score for pain at rest improved from 4.7 (range from 3 to 6) preoperatively to 0.7 (range from 0 to 2) at the last follow-up (P < 0.05)). The mean VAS score during daily activities improved from 6.9 (range from 4 to 8) preoperatively to 1.2 (range from 0 to 2) at the last follow-up (P < 0.05).
Discussion
The condition was first reported in the literature in 1873 by Runge.[7] The term tennis elbow is not too apt since this disorder is commoner in occupations which involve repetitive forearm rotational activities. It has been estimated that only 5%–10% of cases occur in tennis players.[8] Lateral epicondylitis is characterized by local pain and tenderness over the lateral aspect of the elbow, which is the origin of the tendons that move the wrist and fingers. The condition causes a lot of discomfort even during routine activities. It may be caused by repeated microtrauma to the origin of ECRB, but the precise etiology and pathology remain unclear.[9,10] With regard to the pathophysiology of lateral epicondylitis, Cyriax[11] reported that tendinous changes occurred after the pathological healing of microscopic tears caused by repetitive and severe overuse, and Nirschl[4] described it as ultimate ruptures of the tissues already affected by a circulation disturbance, nutritional changes, and overuse. It is believed that the overuse of degenerative tissues results in ruptures, as Nirschl[4] stated, and that the high morbidity among housewives in their 40s and 50s can be explained by this theory. The differential diagnosis can include radial tunnel syndrome, lateral compartment arthritis, and osteochondritis of the capitellum. The initial treatment is with rest, modification of activity, local splints, and steroid injection, and 90% of patients respond to conservative treatment.[10] Steroid injections may provide relief of symptoms in up to 40% of patients. Patients who fail to respond to conservative measures may require surgery. Boyd and McLeod, Posch, Goldberg, and Larrey4 reported that up to 8% of patients require surgery.[12,13] Open ECRB excision, percutaneous extensor tenotomy, and arthroscopic ECRB release are currently the most preferred procedures with an (80%–97%) success rate.[14,15] Percutaneous extensor tenotomy can be effective in dealing with the downsides of open ECRB. However, it also increases the risk of recurrence due to the incomplete removal of a lesion and disrupts the concomitant treatment of an intraarticular lesion because of the limited visualization of the inside of a joint. With regard to arthroscopic ECRB release, it is difficult to suture the ruptured ECRB, to avoid the risk of injuring the lateral collateral ligament during debridement, and to become comfortable with the surgical technique in a short period.[16] An improvement in the understanding of the disorder and in surgical techniques has led to the use of a smaller skin incision. Grundberg and Dobson[17] reported good or excellent results in 29 of 32 elbows and Baumguard and Schwartz[18] achieved 32 excellent and three dissatisfied patients in 35 elbows following surgery for tennis elbow. Nirschl and Pettrone[5] achieved an excellent outcome in 66 of 88 elbows using similar technique used in this study. Our study of 18 cases in patients who had not responded to various conservative modalities had undergone the similar technique involving the debridement of the degenerated ECRB tendon but using a smaller incision. Our study yielded excellent to good results of 93%. Our patients observed a significant improvement in the pain during rest and routine activities. Overall, it is believed that this procedure of minimal incision technique in recalcitrant lateral epicondylitis is an easy and effective treatment option that reduces the time and expense required for conservative treatments. Although arthroscopic ECRB release is also being performed as a minimal invasive procedure, it is difficult to suture the ruptured ECRB and to become comfortable with the arthroscopic technique in a short period, especially at secondary-level care hospitals.
Conclusion
Surgical treatment is an appropriate modality for the patients who had not responded to various conservatively methods. The important point worth mentioning here is the proper selection of patients and exclusion of various pain syndromes affecting the same region
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Tendinosis of the elbow (tennis elbow). Clinical features and findings of histo-logical, immunohistochemical, and electron microscopy studies. J Bone Joint Surg Am. 1999;81:259-78.
- [CrossRef] [Google Scholar]
- Elbow tendinosis/tennis elbow. Clin Sports Med. 1992;11:851-70.
- [CrossRef] [PubMed] [Google Scholar]
- Tennis elbow: The surgical treatment of lateral epicondylitis. J Bone Joint Surg [Am] 1979:61-9.:832-9.
- [CrossRef] [Google Scholar]
- Development of the QuickDASH: Comparison of three item-reduction approaches. Journal of Bone and Joint Surgery. 2005a;87A:1038-46.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous extensor tenotomy for chronic tennis elbow: An office procedure. Orthopaedics. 1985;8:1261-3.
- [CrossRef] [PubMed] [Google Scholar]
- The basic science of lateral epicondylosis: Update for the future. Tech Orthop. 2006;21:250-255. 10.1097/01.bto.0000252115.76643.78.
- [CrossRef] [Google Scholar]
- Percutaneous extensor tenotomy for chronic tennis elbow: An office procedure. Orthopaedics. 1985;8:1261-3.
- [Google Scholar]
- Tennis elbow: Its course, natural history, conservative and surgical management. J Bone Joint Surg [Am] 1973:1177-82.:55-82.
- [CrossRef] [Google Scholar]
- Th e pathology and treatment of tennis elbow. J Bone Joint Surg Am. 1936;18:921-40.
- [Google Scholar]
- Extensor fasciotomy for tennis elbow: A longterm follow-up study. Clin Orthop. 1978;135:179-82.
- [CrossRef] [Google Scholar]
- Surgical treatment of lateral epicondylitis: A systematic review. Clin Orthop Relat Res. 2007;463:98-106.
- [CrossRef] [PubMed] [Google Scholar]
- Tendinosis of the extensor carpi radialis brevis: An evaluation of three methods of operative treatment. J Shoulder Elbow Surg. 2006;15:721-7.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic treatment of lateral epicondylitis. J Korean Orthop Sports Med. 2007;6:105..
- [Google Scholar]
- Percutaneous release of the common extensor origin for tennis elbow. Clin Orthop. 2000;376:137-40.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous release of the epicondylar muscles for humeral epicondylitis. Am J Sports Med. 1982;10:233-6.
- [CrossRef] [PubMed] [Google Scholar]




