
Study of functional outcome of displaced intra-articular fractures of the calcaneum treated with open reduction, bone grafting, and plate fixation
Address for correspondence: Dr. Nikhil Dilip Palange, Assistant Professor, Grant Government Medical College, Room No. 201, High Rise Building, Gokuldas Tejpal Hospital, Fort, CST, Mumbai - 400 001, Maharashtra, India. E-mail: npalange@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Palange ND, Prasannakumar GS, Shah N, Pawar E. Study of functional outcome of displaced intra-articular fractures of the calcaneum treated with open reduction, bone grafting, and plate fixation. J Orthop Allied Sci 2019;7:22-7.
Abstract
BACKGROUND:
Calcaneal fractures are one of the most difficult and challenging fractures to treat by the orthopedic surgeon. Most of these fractures (i.e., almost 75%) are intra-articular. Furthermore, majority of these fractures are highly comminuted. Hence, open reduction and internal fixation (ORIF) with anatomical plate gives the best possible opportunity to bring about near-anatomical joint surface reduction and prevention of subsequent arthritis. This article studies the functional outcome after ORIF of such fractures.
METHODS:
Thirty patients, having intra-articular displaced calcaneum fractures, were admitted and included in the study after obtaining valid consent and permission from the ethical committee. All the patients were investigated with X-ray and computed tomography scan and classified according to the Sanders classification system. The functional outcome after surgery was measured using the American Orthopaedic Foot and Ankle Society (AOFAS) score.
RESULTS:
All patients had joint depression-type fractures with a similar history of trauma due to fall from height. Out of the 30 patients, 26 were male and 4 were female. After surgery, 20 patients out of 30 had good results with a mean AOFAS score of 82.6, 7 patients had fair results with a mean AOFAS score of 70.4, while the remaining 3 patients had poor results with a mean score of 50. Postoperatively, wound complications were seen in 2 patients which settled after debridement and medications. No other complication was encountered.
CONCLUSION:
Open reduction and rigid internal fixation of calcaneum fractures allows anatomical reduction of fracture, restoration of joint surface, and prevention of subtalar joint arthritis and helps in early mobilization after surgery.
Keywords
Calcaneum
fracture
intra-articular
plate

Introduction
Calcaneum fractures account for 2% of all adult fractures and are the most commonly fractured tarsal bone (60%). About 75% of these fractures are intra-articular.[1-3] These fractures result due to axial loading of the calcaneum, that is, fall from height, and therefore, many of these are bilateral or associated with pelvic or vertebral fractures.[1,3,4] Most calcaneum fractures are comminuted and intra-articular. Hence, these are difficult to treat. Conservative management of these fractures almost always leads to continuing disabling pain and stiffness. Consequently, many operative procedures are preferred for the treatment of calcaneal fractures, including percutaneous screw fixation, open reduction, and plating with reconstruction plates as well as fixation with locking anatomical plates. Studies have shown that operative management gives a better outcome than conservative management.
Calcaneum fractures are classified into intra-articular and extra-articular fractures based on the involvement of the subtalar joint. The intra-articular fractures, based on plain radiograph, are further classified by Essex-Lopresti (1952) into joint depression- and tongue-type fractures. On plain radiograph, when the fracture line exits behind the posterior facet and anterior to attachment of Achilles tendon, it is called joint depression-type fracture. Tongue-type fracture is one in which there is a secondary fracture line which exits distal to Achilles tendon attachment, and the articular fragment remains attached to the tuberosity fragment.[5,6] A further detailed descriptive classification was given by Sanders[7,8] based on axial view computed tomography (CT) scan. According to this classification, undisplaced fractures are classified as Type I. Type II is further classified into IIA, IIB, and IIC based on the location of the primary fracture line. Type III is classified into IIIAB, IIIBC, and IIIAC. Comminuted fractures are classified as Type IV.
The present study aims at evaluating the functional outcome of displaced intra-articular calcaneum fractures, operated with open reduction and internal fixation (ORIF) with locking plate with bone graft.
Materials and Methods
A prospective study was conducted from June 2014 to July 2018 in the Department of Orthopaedics, Grant Government Medical College, after getting permission of the ethical committee. Thirty patients with a history of fall from height, having closed intra-articular calcaneum fractures, were admitted and included in the study, after obtaining proper valid written informed consent. All patients with displaced, intra-articular calcaneum fractures aged 18–60 years were included, whereas patients with paraplegia/paraparesis, long-bone fractures in ipsilateral limb, open fractures, fractures of other tarsal bones, and arthritis of the ankle or subtalar joint were excluded from the study.
Patients with a history of fall from height were evaluated clinically. All patients had swelling and tenderness in the ankle with loss of range of motion (ROM) at presentation. Distal neurovascular deficit was ruled out, and patients were subjected to plain radiographs of the ankle in anteroposterior, lateral, and axial views (if possible) to note the type of fracture and intra-articular extension. CT scan of the calcaneum was also done in all patients to further delineate the type and pattern of fractures, and fracture was classified by the Sanders classification system. All patients were given primary treatment in the form of below-knee Plaster of Paris(POP) slab, analgesic anti-inflammatory medications, and strict bed rest and limb elevation until a patient is posted for surgery.
All patients were posted for surgery only once swelling subsided and wrinkles over the local skin began to be visible. Patients were operated under spinal anesthesia in the lateral position. After careful scrubbing, painting, and draping of the fractured side ankle, tourniquet was raised after exsanguination. Curved incision was taken on the lateral side, running parallel to tendoachilles, curved slightly just below lateral malleolus, and then parallel to the fifth metatarsal shaft. Full-thickness flap is raised subperiosteally to avoid flap necrosis and to expose the subtalar joint, calcaneum, lateral malleolus, cuboid, and lateral navicular. Three smooth k-wires are inserted each into the lateral malleolus, talus, and cuboid. These wires were bent so as to retract the flap upward [Figure 1]. A wet mop was kept between the flap and k-wires to keep the flap moist at all time during surgery. Fracture site was cleared off all calluses. Essex-Lopresti maneuver was used to elevate the depressed joint, under C-arm vision. After ensuring proper reduction of joint line and restoration of Bohler's and Gissane's angles in lateral fluoroscopic vision, temporary fixation was done with k-wires. Locking anatomical plate was prebent according to the contour of the calcaneum and fixed with locking screws of appropriate sizes [Figure 2]. Corticocancellous bone graft retrieved from iliac crest was used to fill the defect in all patients. Wound was closed in layers under vacuum drain.
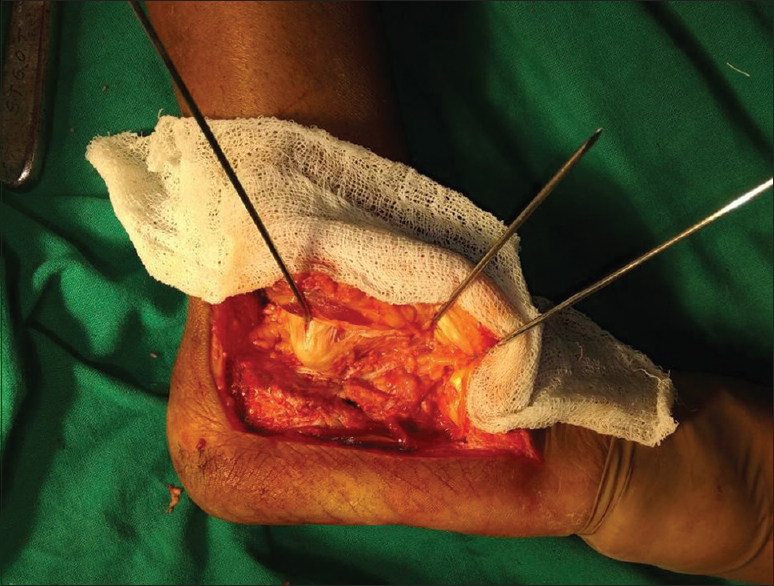
- Intraoperative photograph showing retracted flap with k-wires through lateral malleolus, talus, and cuboid, exposing the calcaneum
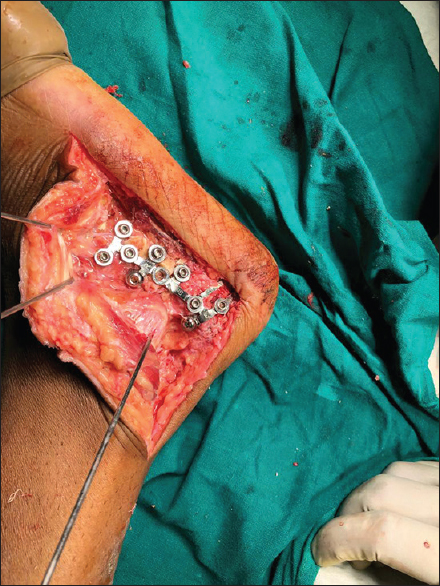
- Intraoperative photograph showing final fixation of fracture with contoured locking calcaneal plate
Postoperative care
Wound was dressed on the 3rd postoperative day, and sutures were removed after 10–14 days. Short leg splint was given for 5–7 days after surgery followed by active ROM exercises. Full weight bearing was started after 12 weeks. A patient was followed up at 12 weeks, 6 months, and 12 months. At each follow-up, plain radiograph was taken, and functional outcome and ankle ROM was measured. Functional outcome was measured with the American Orthopaedic Foot and Ankle Society (AOFAS) score[9] which includes pain, function, and alignment. Radiological outcome was assessed by the angle of Bohler, angle of Gissane, and assessing union of fracture.
All data were collected and analyzed by the Epi Info 7 software, developed by Centers for Disease Control and Prevention (CDC) in Atlanta, Georgia (United States of America) and using Chi-square test. P < 0.005 was considered to be statistically significant.
Results
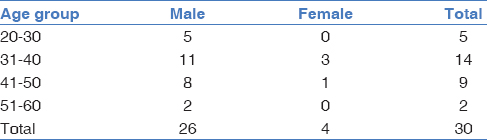
A prospective study of 30 consecutive patients having joint depression type of calcaneal fractures was carried out in Grant Government Medical College and Sir JJ Group of Hospitals. All patients were operated with open reduction, bone grafting, and fixation with locking anatomical plate [Figures 3 and 4]. The mean follow-up period was 28.4 weeks. Of the 30 patients, 26 were male and 4 were female [Table 1]. Patients were between the age groups of 20–60 years with an average age being 32 years [Table 1]. Out of the 30 patients, 19 (63.33%) had Sanders type II fracture while 11 (36.67%) had Sanders type III fracture. Seventeen (56.67%) patients had left-sided fracture and 13 (43.33%) had right-sided fracture.

- Anteroposterior (a) and lateral (b) views of ankle in a 45-year-old male having intra-articular calcaneum fracture. Patient was operated with open reduction and fixation with locking calcaneal plate. Immediate post-operative lateral (c) and axial (d) views of calcaneum of the same patient

- Follow up X-rays (lateral and axial views) of the patient showing progressive union at 4 months following surgery (a and b) and solid union of the fracture at postoperative 8 months (c and d)
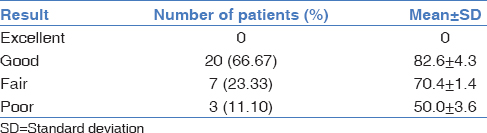
Twenty patients out of 30 had good results with a mean AOFAS score of 82.6, 7 patients had fair results with a mean AOFAS score of 70.4 while the remaining 3 patients had poor results with a mean score of 50 [Table 2].
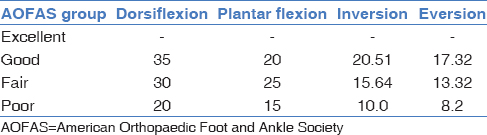
Among the patients with good results, the mean ankle dorsiflexion and plantar flexion were 35 and 20, respectively, whereas the mean inversion and eversion at the subtalar joint were 20.51 and 17.32, respectively. For the group of fair results, the mean ankle dorsiflexion and plantar flexion were 30 and 25, respectively, whereas the mean inversion and eversion at the subtalar joint were 15.64 and 13.32, respectively. Patients having poor AOFAS score had mean ankle dorsiflexion and plantar flexion of 20° and 15°, respectively, and mean inversion and eversion were 10° and 8.2°, respectively [Table 3 and Figure 5]. The mean time of fracture union was 23.5 weeks [Figure 4].

- (a) wound healed without complications and (b and c) postoperative ankle dorsiflexion and plantar flexion
Postoperative wound complication was noted in 4 patients, who had wound dehiscence up to subcutaneous tissue. None of the patients had infection of the wound. Donor-site morbidity in the form of mild discomfort was seen in three patients.
Discussion
Calcaneal fractures are one of the most difficult fractures to treat owing to the complicated fracture pattern and comminution. Conservative treatment in the form of cast is effective only in extra-articular fractures and in some undisplaced intra-articular fractures. For displaced intra-articular fractures, conservative treatment may lead to deformity, posttraumatic arthritis, and severe stiffness of the ankle and subtalar joint. Thordarson and Krieger, in their randomized control trial, have indicated the superiority of operative management over conservative management in displaced intra-articular calcaneum fractures.[10] Surgery for calcaneum fractures should be delayed by 10–14 days so that the soft-tissue swelling subsides, and there is no risk of wound problems after surgery. Operative techniques include both closed pinning or screw fixation as well as open reduction and plate fixation.[11-13] Both techniques have merits and demerits. Closed techniques offer advantages of less tissue dissection, less wound problems, and better cosmetic results.[14] However, it may be difficult to achieve anatomic reduction with these techniques. On the other hand, open reduction allows the surgeon to have direct visualization of the fragments and articular surface and hence achieve anatomical reduction of fracture. Plate fixation also provides rigid fixation as compared to screw fixation.[15]
In our study, we operated intra-articular fractures Sanders Type II, III, and IV using a lateral approach[16] and used locking anatomical plate for achieving anatomical reduction and rigid fixation. The goals of fixation were to achieve anatomical reduction of articular surface, restoration of calcaneal width, decompression of subfibular space available for peroneal tendons, and reduction of the calcaneocuboid joint in some cases.[11,17] Stress was laid on adequate restoration of articular surface and angles of Bohler and Gissane. Bone graft was inserted in fracture site in all cases to maintain the calcaneal height and width, to prevent the collapse of the articular cartilage, and to promote earlier fracture healing.
Buckley et al.[18] conducted a prospective cohort study of 95 patients in 1999 to compare nonoperative treatment of calcaneum fractures to open reduction and fixation. They found that operative management which enables anatomic reduction has a better outcome than nonoperative treatment, in selected group of patients. A similar study conducted by Paul et al.[19] in 2004 concluded the superiority of operative management, especially in those cases where the anatomic reduction of articular surface and restoration of Bohler's angle was achieved. Previously, calcaneal fractures were mostly treated conservatively leading to increased risk of malunion, stiffness, and arthritis. Palmer[20] published studies regarding open reduction, subtalar joint reduction, bone grafting of defects, and plate fixation, and after this, the importance of open reduction and plate fixation of these fractures gained popularity.
Majority of the authors described a lateral L-shaped exposure to most of the calcaneal fractures.[5,21,22] We have used the extended L-shaped approach in all our cases which gave good exposure of the fracture site, the subtalar and calcaneocuboid joints. However, this novel approach despite being easy has its demerits. If the soft-tissue flap is not deep, there may be wound healing problems and skin necrosis. Other problems related to the exposure are sural nerve injury and Complex Regional Pain Syndrome(CRPS). The wound problems can be prevented by raising deep subperiosteal flap, avoiding subcutaneous flaps, avoiding rash handling, or retracting of incision edges and constant irrigation of edges during surgery. Furthermore, avoiding surgery till the soft-tissue swelling settles aids in minimizing the risk of postoperative wound complications. Sural nerve injury can be prevented by raising subperiosteal flaps and dissecting the nerve at the proximal and distal edges of the incision.
In our study, out of 30 patients, 20 had good results with a mean AOFAS score of 82.6, 7 patients had fair results with a mean AOFAS score of 70.4, while the remaining 3 patients had poor results with a mean score of 50. The range of ankle and subtalar joints was better in the patients with good score and worst in those with poor scores. Four patients had wound complications, which were managed with daily dressing and debridement. The findings in our study were comparable to those of other studies.
The limitations in our study were the small number of cases and the shorter time of follow-up. Large multicentric trials may further show the efficacy of open reduction of calcaneal fractures and fixation with plates. Furthermore, comparison with cases who are treated conservatively may aid in better understanding of the management of these fractures.
Conclusion
Our study shows that ORIF with bone graft insertion of displaced intra-articular calcaneum fractures is an effective method for treatment as it enables anatomical reduction of fracture and articular surface, restoration of Bohler's angle, and early union by the bone graft. However, care must be taken to avoid wound problems by meticulous dissection and soft-tissue handling.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Fractures and dislocations of the calcaneus. In: Bucholz RW, Heckman JD, eds. Rockwood and Green's Factures in Adults Vol 3. (5th). Philadelphia: Lippincott Williams & Wilkins; 2001. p. :2133-79.
- [Google Scholar]
- Fractures and dislocations of foot. In: Canale ST, ed. Campbell's Operative Orthopaedics Vol 4. (10th). Philadelphia: Mosby Inc.; 2003. p. :4231-83.
- [Google Scholar]
- Outcome after open reduction and internal fixation of intraarticular fractures of the calcaneum without the use of bone grafts. Indian J Orthop. 2006;40:111-4.
- [CrossRef] [Google Scholar]
- Results after operative treatment of intra-articular calcaneal fractures with a minimum follow-up of 2 years. Injury. 1998;29:593-9.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical treatment of displaced intra-articular calcaneal fracture using a single small lateral approach. Strategies Trauma Limb Reconstr. 2010;5:87-95.
- [CrossRef] [PubMed] [Google Scholar]
- Fracture blisters: Clinical and pathological aspects. J Orthop Trauma. 1993;7:417-27.
- [CrossRef] [PubMed] [Google Scholar]
- Operative treatment in 120 displaced intraarticular calcaneal fractures. Results using a prognostic computed tomography scan classification. Clin Orthop Relat Res (290):87-95.
- [CrossRef] [Google Scholar]
- Intra-articular fractures of the calcaneus: Present state of the art. J Orthop Trauma. 1992;6:252-65.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994;15:349-53.
- [CrossRef] [PubMed] [Google Scholar]
- Operative vs. nonoperative treatment of intra-articular fractures of the calcaneus: A prospective randomized trial. Foot Ankle Int. 1996;17:2-9.
- [CrossRef] [PubMed] [Google Scholar]
- Operative treatment of displaced intra-articular fractures of the calcaneum. Medium-term results. J Bone Joint Surg Br. 1993;75:196-201.
- [CrossRef] [PubMed] [Google Scholar]
- Open reduction and internal fixation for displaced intra-articular fractures of the os calcis. Injury. 1995;26:111-5.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of os calcis fractures by open reduction and internal fixation. Foot Ankle Int. 1994;15:225-32.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical treatment of calcaneal fractures of sanders type II and III by a minimally invasive technique using a locking plate. J Foot Ankle Surg. 2015;54:76-81.
- [CrossRef] [PubMed] [Google Scholar]
- Radiographic and functional outcomes after displaced intra-articular calcaneal fractures: A comparative cohort study among the traditional open technique (ORIF) and percutaneous surgical procedures (PS) J Orthop Surg Res. 2016;11:92..
- [CrossRef] [PubMed] [Google Scholar]
- Surgical treatment of intra-articular calcaneal fractures. Clin Podiatr Med Surg. 2014;31:539-46.
- [CrossRef] [PubMed] [Google Scholar]
- Open reduction and internal fixation of type II intra-articular calcaneus fractures. Foot Ankle Int. 1996;17:253-8.
- [CrossRef] [PubMed] [Google Scholar]
- Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002:1733-44.:84-44.
- [CrossRef] [PubMed] [Google Scholar]
- Fractures of the calcaneum. A review of 70 patients. J Bone Joint Surg Br. 2004;86:1142-5.
- [CrossRef] [PubMed] [Google Scholar]
- The mechanism and treatment of fractures of the calcaneus; open reduction with the use of cancellous grafts. J Bone Joint Surg Am. 1948;30A:2-8.
- [CrossRef] [Google Scholar]
- Long-term results of calcaneal fracture treatment by open reduction and internal fixation using a calcaneal locking compression plate from an extended lateral approach. Acta Chir Orthop Traumatol Cech. 2008;75:457-64.
- [CrossRef] [Google Scholar]
- Intra-articular fractures of the calcaneum. Part II: Open reduction and internal fixation by the extended lateral transcalcaneal approach. J Bone Joint Surg Br. 1993;75:189-95.
- [CrossRef] [PubMed] [Google Scholar]




