
Translate this page into:
Study of biochemical profile and 25-hydroxy Vitamin D association with disease activity in rheumatoid arthritis patients
Address for correspondence: Dr. Regupathy Annamalai, Department of Orthopedics, Karpaga Vinayaga Institute of Medical Sciences and Research Center, Madhurantagam, Kancheepuram, Tamil Nadu, India. E-mail: annuregu@yahoo.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Annamalai R, Kumar AN. Study of biochemical profile and 25-hydroxy Vitamin D association with disease activity in rheumatoid arthritis patients. J Orthop Allied Sci 2018;6:17-21.
Abstract
BACKGROUND:
Vitamin D deficiency has been implicated in the pathogenesis of autoimmune diseases. Reduced Vitamin D intake has been linked to increased susceptibility to the development of rheumatoid arthritis (RA). The objective was to evaluate 25-hydroxy (25-OH) Vitamin D status in patients with RA and to assess the relationship between Vitamin D level and RA disease activity.
MATERIALS AND METHODS:
The study consists of 50 RA patients as cases and 50 age- and body mass index matched healthy individuals as controls. All study participants (both controls and cases) underwent biochemical profile such as RA factor, serum uric acid (UA), calcium, phosphorous, alkaline phosphatase, and 25-OH Vitamin D levels. Disease activity was evaluated by calculating the 28-joint count as disease activity score. All the results were expressed as mean and standard deviation (SD).
RESULTS:
Mean and SD values of serum UA (mg/dl), calcium (mg/dl), and phosphorous levels (mg/dl) in RA cases are as follows 7.2 ± 1.3, 7.5 ± 0.5, and 6.9 ± 1.5, respectively. Serum UA, calcium, and phosphorous levels in RA cases were found to be elevated when compared to controls (P < 0.0001). Mean erythrocyte sedimentation rate was 58.4 ± 14.7 mm/h in the group of patients with RA. Levels of 25-OH Vitamin D were found to be negatively correlated to the DAS28, the correlation coefficient being r = −0.51 (P < 0.05). Levels of 25-OH Vitamin D were found to be positively correlated to serum calcium levels, the correlation coefficient being r = 0.82 (P < 0.01).
CONCLUSION:
RA patients had lower Vitamin D values than healthy controls. There was a negative correlation between serum Vitamin D and RA disease activity.
Keywords
Alkaline phosphatase
autoimmune disorder
calcium
disease activity score 28
inflammation
phosphorous
rheumatoid arthritis
uric acid
Vitamin D

Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disorder characterized by systemic features and joint involvement which affects 1% of the world's adults.[1,2] It can lead to significant morbidity and mortality. Initially, the diagnosis of RA was mostly based on clinical manifestations. However, it is often difficult to diagnose RA in very early phases of the disease and in many cases, irreversible damage has occurred by the time diagnosis was confirmed.[2-4] Therefore, laboratory tests which are sensitive and specific for RA and can identify early in the disease course are required for diagnosis and intervention. Vitamin D might be one of the environmental factors relevant with RA.[3-5]
Etiology of RA is not known clearly.[6] Role of Vitamin D deficiency in the pathogenesis of RA was the interest of the study. The aim of the present study was to estimate serum calcium, phosphorus, alkaline phosphatase (ALP), and 25-hydroxy (25-OH) Vitamin D levels in RA patients and also to find the association between Vitamin D and RA, as well as the relationship of Vitamin D with disease activity score (DAS) in RA patients.
Materials and Methods
The present case–control study was conducted at tertiary medical center. The study includes 50 newly diagnosed RA cases along with 50 age- and body mass index-matched controls. The patients with age range of 32–56 years were selected for this study. Patients with known history of diabetes, hypertension, liver, kidney, thyroid dysfunction, any previous or current cardiac illness or hyperuricemia, or with coexisting disease associated with high uric acid (UA) levels, for example, malignancy, chronic renal failure, active chronic infections, for example, tuberculosis were excluded from the study. Diagnosis of RA was done according to the revised criteria formulated by the American College of Rheumatology.[7] About 5 ml of venous blood was collected from anticubetal vein. Serum was separated by centrifuging at 3500 rpm for 15 min. All the study participants (both cases and controls) underwent biochemical analysis for serum RA factor, serum UA, calcium, phosphorus, serum ALP, and erythrocyte sedimentation rate (ESR). Besides biochemical investigations mentioned above, the DAS based on 28 joint counts (such as swollen joint count + tender joint count + patient's global activity) was also considered at the time of RA disease diagnosis.[5,7] The same biochemical investigations were done in healthy controls as well. For all the 50 cases, RA factor test is positive, and the test was done by qualitative slide method. The study was approved by the Institutional Ethics Committee. Written and informed consent was obtained from all the participants.
Serum UA, calcium, phosphorus, and ALP were measured using semi-automated biochemistry analyzer with the commercial kits available in the market. ESR was determined by Westergren method in whole blood with ethylenediaminetetraacetic acid. Serum 25-OH Vitamin D was measured by enzyme-linked immunofluorescent assay using kits (Biomerieux, France) available for mini-vidas fully automated analyzer.
Results obtained were tabulated and expressed as mean ± standard deviation (SD). Pearson correlation was done to find out the association of biochemical parameters with DAS28. Associations between continuous variables were examined using Pearson correlation coefficients. Differences were considered statistically significant at P < 0.05. Statistical analysis was done by SPSS software version 16.0 (IBM, USA).
Results
The study consists of 50 RA patients and 50 apparently healthy individuals as control. Mean age of the controls is 43.2 ± 6.6 years and that of RA cases is 42.7 ± 6.7 years [Table 1]. All the RA patients included in the present study had positive RA factor.
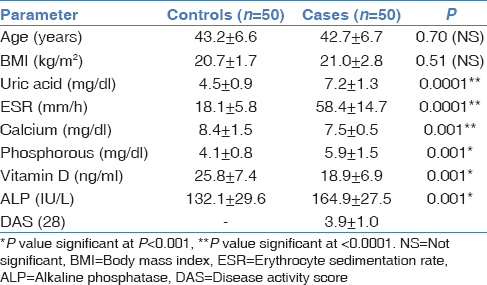
In the present study, it is found that there is a significant increase in the UA level in RA patients when compared to the healthy controls (P < 0.001) [Table 1 and Figure 1]. Mean serum uric level of controls is 4.5 ± 0.9 and that of RA cases is 7.2 ± 1.3. The normal value of calcium 9–11 mg/dl; however, in this study, calcium levels were found to be decreased with mean serum calcium level in RA patients was 7.5 ± 0.5 and that of controls is 8.4 ± 0.5 (with minimum of 6.9 mg/dl and maximum of 8.3 mg/dl) [Figure 1]. Serum phosphorus values were found to be increased in RA cases when compared to that of controls. Mean values of phosphorous in controls are 4.1 ± 0.8 and that of controls is 5.9 ± 1.5 [Table 1 and Figure 1]. Serum ALP normal range in adults is 20–140 IU/L. In this study, the mean and SD of serum ALP level was 164.9 ± 27.5 (minimum of 138 IU/L and maximum of 289 IU/L) and that of controls was 132.1 ± 29.6 clearly indicates significant raise (P < 0.001) [Table 1]. On comparison with controls, serum ALP levels were found to be increased [Figure 2], and calcium levels were decreased in RA patients. This clearly suggests that an increase of ALP in serum can provide valuable diagnostic information about RA. Serum calcium levels were significantly decreased (P < 0.001) in RA patients as compared to controls, while serum ALP levels were increased significantly (P < 0.001) than controls. The serum phosphorus levels were increased significantly (P > 0.05) than controls, whereas there was a significant increase (P < 0.001) in serum UA levels than controls [Table 1].
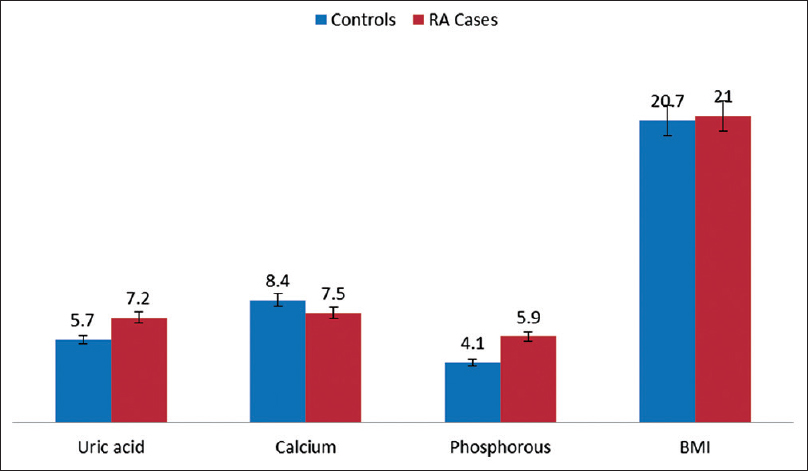
- Comparison of mean values uric acid, calcium phosphorous, and body mass index in controls and cases
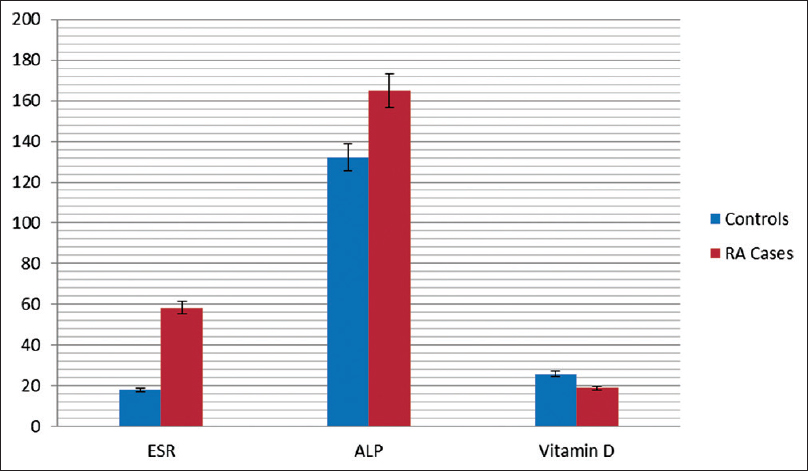
- Comparison of erythrocyte sedimentation rate, alkaline phosphatase, and Vitamin D between controls and cases
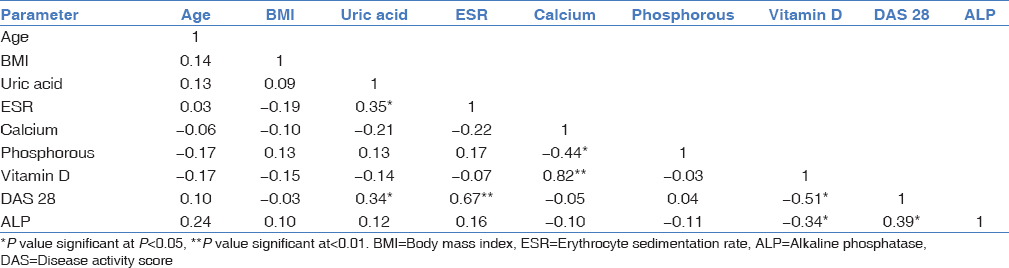
In Table 2, Pearson correlation of all studied parameters among RA patients was shown. From Table 2, it is evident that UA has a positive correlation with ESR and DAS28. Similarly, it can be observed that there is a positive correlation of ESR with DAS. In the present study, DAS28 score is 3.9 ± 1.0. DAS28 and adenosine deaminase, C-reactive protein, and ESR (r = 0.41, P < 0.05; r = 0.59, P < 0.05; r = 0.67, P < 0.01). In this study, negative correlation is observed between calcium and phosphorous (r = −0.44, P < 0.05) of RA patients and serum Vitamin D levels with DAS (r = −0.51, P < 0.01); serum Vitamin D levels with serum ALP (r = −0.34, P < 0.05). There is a positive correlation of serum ALP level with DAS28 (r = 0.39, P < 0.05), similarly positive correlation was observed between calcium and phosphorous (r = 0.82, P < 0.001) [Table 2].
Discussion
Increased serum UA levels are associated with decreased kidney function[8] and gouty arthritis.[9,10] Further, increased UA level also causes endothelial dysfunction which in turn aggravates the risk of developing diseases such as cardiovascular disease,[11,12] or insulin resistance with its antioxidant property, high level of UA was found to increase bone mineral density for all sites and thus decreased the odds of fractures,[13] decreased risk of dementia[14] and Parkinson's disease. Serum UA which is a prooxidant, particularly effective in quenching hydroxyl, superoxide, and peroxynitryl radical, thereby preventing lipid peroxidation.[15,16] In the present study, it is found that there is a significant increase in the UA level in the RA patients when compared to the healthy controls. This is in accordance with the previous studies reported by Panoulas et al.[17] and Lippi et al.[18]
Calcium and phosphorous are important constituent of bone; ultimately bone metabolism is altered in RA, observed by many researchers.[19] In the present study, calcium levels are significantly decreased in rheumatoid patients, whereas ALP levels are significantly increased as compared to controls. Serum phosphorus levels are increased significantly than controls. The previous studies reported that the concentrations of serum calcium and phosphorus are usually reduced, and serum ALP activity was elevated in RA patients.[20,21] A significantly decreased calcium/phosphorus ratio in RA patients as compared to controls in our study clearly indicates that there is altered calcium and phosphorous metabolism in RA. Our study reports are correlating with patient's signs and symptoms, such as low serum calcium levels associated with muscle spasm in the hands, feet, throat, and bone pains in the upper and lower limbs. As bone softness, weight bearing may lead to bowing of the legs, weakened bones, osteoporosis which can lead to increased susceptibility to fractures in patients with RA.[20-22]
Our study is supporting the general concept of elevated ALP levels in adults over the age of fifty. In the present study, there is a significant increase in serum ALP levels in RA patients when compared to controls. Causes of high ALP levels in patients with RA is because of the disease affects in the wrist and small joints of the hand and also other parts of the body besides the joints. Previous studies reported that the concentrations of serum calcium and phosphorus are usually reduced, and the serum ALP activity was elevated.[20-22] Hence, our reports also strengthening that the serum calcium levels were reduced and serum ALP were increased in these patients.
In the present study, an inverse association was observed between Vitamin D levels and RA DAS). Several studies have evaluated the association between Vitamin D levels and RA activity. In a study involving 1191 patients with RA and 1019 controls, Rossini et al. found an inverse association between Vitamin D levels and disease activity in RA.[23] Welsh et al., and Kerr et al., found that Vitamin D deficiency is linked with disease activity in RA.[24,25] In addition, Kerr G et al. and Haque and Bartlett found an inverse relationship between Vitamin D levels and disease activity in RA.[5,7,26] Vitamin D is known to induce immunologic tolerance.[27] Thus, Vitamin D deficiency may perturb immune tolerance and induce the[6,23] development of autoimmune diseases, such as RA. Vitamin D has immunomodulatory properties, acting on the immune system both in an endocrine and in a paracrine manner.[28,29] It appears to regulate the immune response by a variety of mechanisms, such as decreasing antigen presentation,[6,23] inhibiting the proinflammatory T helper type 1 profile,[30] and inducing regulatory T cells.[23,30] 25-OH Vitamin D suppresses proliferation and immunoglobulin production and retards differentiation of B-cell precursors into plasma cells.[30] These data support a role for Vitamin D deficiency in the development and progression of autoimmune inflammatory conditions in general and in particular RA. In the present study, Vitamin D levels were found to be low in a group of patients with RA. Vitamin D levels were found to be negatively correlated with disease activity in RA [Table 2].
Conclusion
The present study showed that high-UA level was directly associated with the DAS28 in RA patients. Serum calcium is decreased and serum phosphorous and serum ALP is increased in RA patients when compared with controls. This study will provide awareness in using serum ALP activity to assess the disease activity, to understand response to therapy and prevent deformities of RA. Supplementation of Vitamin D along with calcium may be recommended for the pain relief in patients with RA.
Financial support and sponsorship
Nil.
Acknowledgment
The authors would like to sincerely thank the patients who participated in the study.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Epidemiology of adult rheumatoid arthritis. Autoimmun Rev. 2005;4:130-6.
- [CrossRef] [PubMed] [Google Scholar]
- Relationship between vitamin D and rheumatoid arthritis disease. Pak J Nutr. 2012;11:293-300.
- [CrossRef] [Google Scholar]
- Role of vitamin D in flare ups of rheumatoid arthritis. Z Rheumatol. 2014;73:461-4.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D deficiency and risk for rheumatic diseases: An update. Curr Opin Rheumatol. 2013;25:184-91.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D level: Is it related to disease activity in inflammatory joint disease? Rheumatol Int. 2011;31:493-9.
- [CrossRef] [PubMed] [Google Scholar]
- Modulatory effects of 1,25-dihydroxyvitamin D3 on human B cell differentiation. J Immunol. 2007;179:1634-47.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison between DAS28, CDAI and HAQ-DI as tools to monitor early rheumatoid arthritis patients in Eastern India. Indian J Rheumatol. 2011;6:116-22.
- [CrossRef] [Google Scholar]
- Meta-analysis identifies multiple loci associated with kidney function-related traits in East Asian populations. Nat Genet. 2012;44:904-9.
- [Google Scholar]
- The genetics of hyperuricaemia and gout. Nat Rev Rheumatol. 2012;8:610-21.
- [CrossRef] [PubMed] [Google Scholar]
- Uric acid transport and disease. J Clin Invest. 2010;120:1791-9.
- [CrossRef] [PubMed] [Google Scholar]
- Uric acid as a potential mediator of cardiovascular morbidity in obstructive sleep apnea syndrome. Eur J Intern Med. 2014;25:471-6.
- [CrossRef] [PubMed] [Google Scholar]
- Association between serum uric acid levels and cardiovascular disease in middle-aged and elderly Chinese individuals. BMC Cardiovasc Disord. 2014;14:26..
- [CrossRef] [PubMed] [Google Scholar]
- Serum uric acid is associated with bone health in older men: A cross-sectional population-based study. J Bone Miner Res. 2011;26:955-64.
- [CrossRef] [PubMed] [Google Scholar]
- Serum uric acid and cognitive function and dementia. Brain. 2009;132:377-82.
- [CrossRef] [PubMed] [Google Scholar]
- Review of concepts and controversies of uric acid as antioxidant and pro-oxidant. Arch Med Rev J. 2015;24:19-40.
- [Google Scholar]
- Antioxidant supplementation for health – A boon or a bane? J NTR Univ Health Sci. 2014;3:221-30. Available from: http://www.jdrntruhs.org/article.asp?issn=22778632;year=2014;volume=3;issue=4;spage=221;epage=230;aulast=Satyanarayana;type=0 (accessed )
- [CrossRef] [Google Scholar]
- Association of serum uric acid with cardiovascular disease in rheumatoid arthritis. Rheumatology (Oxford). 2007;46:1466-70.
- [CrossRef] [PubMed] [Google Scholar]
- Hyperuricaemia is associated with increased C-reactive protein concentrations in a large cohort of unselected outpatients. Nutr Metab Cardiovasc Dis. 2008;18:e41-2.
- [CrossRef] [PubMed] [Google Scholar]
- Alkaline phosphatase levels in rheumatoid arthritis and osteoporosis in clinical practice. J Curr Trends Clin Med Lab Biochem. 2013;1:20-3.
- [Google Scholar]
- Clinical assessment of the long-term risk of fracture in patients with rheumatoid arthritis. Arthritis Rheum. 2006;54:3104-12.
- [CrossRef] [PubMed] [Google Scholar]
- Abnormalities of bone mineral density and bone metabolism in Venezuelan patients with rheumatoid arthritis. J Clin Rheumatol. 2003;9:219-27.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D deficiency in rheumatoid arthritis: Prevalence, determinants and associations with disease activity and disability. Arthritis Res Ther. 2010;12:R216.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D deficiency is common in patients with RA and linked to disease activity, but circulating levels are unaffected by TNFα blockade: Results from a prospective cohort study. Ann Rheum Dis. 2011;70:1165-7.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of vitamin D insufficiency/deficiency in rheumatoid arthritis and associations with disease severity and activity. J Rheumatol. 2011;38:53-9.
- [CrossRef] [PubMed] [Google Scholar]
- Relationships among vitamin D, disease activity, pain and disability in rheumatoid arthritis. Clin Exp Rheumatol. 2010;28:745-7.
- [Google Scholar]
- Bacterial components plus vitamin D: The ultimate solution to the asthma (autoimmune disease) epidemic? J Allergy Clin Immunol. 2011;127:1128-30.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D and immune function: Autocrine, paracrine or endocrine? Scand J Clin Lab Invest Suppl. 2012;243:92-102.
- [Google Scholar]
- Vitamin effects on the immune system: Vitamins A and D take centre stage. Nat Rev Immunol. 2008;8:685-98.
- [CrossRef] [PubMed] [Google Scholar]
- Additive immunosuppressive effects of 1,25-dihydroxyvitamin D3 and corticosteroids on TH1, but not TH2, responses. J Allergy Clin Immunol. 2000;106:981-5.
- [CrossRef] [PubMed] [Google Scholar]
- Immunomodulatory effects of vitamin D in multiple sclerosis. Brain. 2009;132:1146-60.
- [CrossRef] [PubMed] [Google Scholar]




