
Translate this page into:
Role of bipolar hemiarthroplasty and total hip arthroplasty in unstable intertrochanteric fracture femur
Address for correspondence: Dr. Chandra Prakash Pal, Department of Orthopaedics, S. N. Medical College, Agra, Uttar Pradesh, India. E-mail: drcportho@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Pal CP, Dinkar KS, Mittal V, Goyal A, Singh M, Hussain A. Role of bipolar hemiarthroplasty and total hip arthroplasty in unstable intertrochanteric fracture femur. J Orthop Allied Sci 2016;4:69-74.
Abstract
Introduction:
Intertrochanteric femur fracture incidence has increased due to increased life expectancy and osteoporosis. Management of these fractures in elderly is challenging due to difficult anatomical reduction, poor bone quality and osteoporosis. Internal fixation in these cases usually involves prolonged bed rest to prevent implant failure which leads higher complication such as deep vein thrombosis, pneumonia pulmonary embolism, bed sores, increased morbidity.
Materials and Methods:
We have done a prospective study in 18 cases of unstable intertrochanteric fracture where 12 (not associated hip arthritis) patients are operated by bipolar hemiarthroplasty and 6 (associated hip arthritis) patients operated by total hip arthroplasty (THA).
Results:
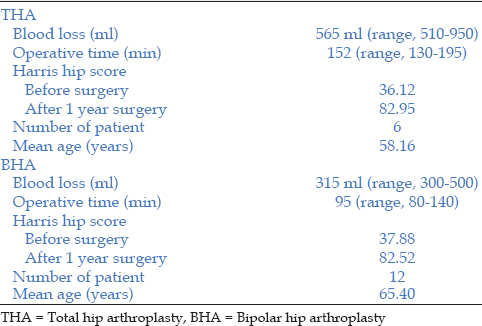
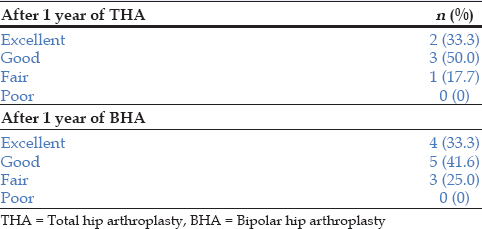
Patients were followed for an average of 12 months duration (9-15 months). Patients treated by bipolar hemiarthroplasty group (Group 1) have an average surgery duration of 95 min and blood loss of 315 ml. While patients treated with THA (Group 2) has average surgery duration of 152 min, blood loss of 565 ml. About 91% of 1st group and 100% of 2nd group has an excellent to fair outcome.
Conclusion:
Bipolar hemiarthroplasty for unstable intertrochanteric fracture femur without hip arthritis, and THA for intertrochanteric fracture with hip arthritis in elderly patient results in early ambulation and good functional outcome. However, as our study group is small, so further large randomized trail required before reaching conclusion.
Keywords
Hemiarthroplasty
osteoporosis
total hip arthroplasty
unstable intertrochanteric fracture

Introduction
Intertrochanteric fracture is common fracture in elderly people. Their incidence has increased due to the increased life expectancy and osteoporosis.[1] Earlier, these fractures were managed conservatively by traction or external splinting which resulted in higher morbidity and complication.[2] Hence, trends for operative intervention increased with time.[3,4,5] Stable intertrochanteric fractures can be easily treated by osteosynthesis with predictable good result[6,7] whereas the management of unstable intertrochanteric fracture are challenging because of poor bone quality, osteoporosis, and other underlying diseases.[8,9] In past, fixed nail plate devices used for the fixation of these fracture, had high rates of cut-out and fracture displacement,[10,11] subsequently, a sliding hip screw was used with much success and became the predominant method of fixation of these fractures.[12,13,14] Intramedullary interlocking devices have shown reduced tendency for cut-outs in osteoporotic bone[15] and also have better results in cases of unstable intertrochanteric fractures.[15,16] Complications such as head perforations, excessive sliding leading to shortening, plate pull-out, and plate breakage continued to be a problem, especially with the unstable type of fractures.[17,18] Osteoporosis and instability are most important factors leading to unsatisfactory results.[19,20] In internal fixation, a period of restricted mobilization is suggested,[21] which may lead complications such as atelectasis, bed sores, pneumonia, and deep vein thrombosis. Despite advances in internal fixation techniques, the failure rate of the dynamic hip screw is 6.8% to 9.8% while failure rate of the proximal femoral nail is between 7.1% and 12.5% in unstable fractures. There have been various reports of successful outcomes after the use of hemiarthroplasty and total hip arthroplasty (THA).[22] Endoprosthetic replacements have also been shown to achieve early rehabilitation of the patient and good long-term result. Many author reported that primary cemented endoprosthesis brought better results than compression hip screw in unstable intertrochanteric fractures in elderly osteoporotic patients who were eligible for early mobilization.[23] In failed intertrochanteric treatment cases, two main treatment options are available, either revision of internal fixation or salvage treatment with hip arthroplasty.[24,25,26,27] Revisions of internal fixation for nonunited fractures have been reported to have good results in younger patients with good bone stock while in older patients with poor bone quality and degenerative acetabular changes; hip arthroplasty has been advocated as a salvage procedure. However, an ideal treatment method is still rather controversial. Hence, the purpose of our study is to study the role of prosthesis replacement in this kind of intertrochanteric femur fracture.
Materials and Methods
In our study, at S.N. Medical College, Agra, 18 cases of intertrochanteric fractures were treated with bipolar hemiarthroplasty or THA between April 2013 and November 2014 were studied prospectively, and subjected to study the role of these surgeries in the intertrochanteric fracture femur.
The inclusion criteria were as follows:
Unstable intertrochanteric fractures in elderly patient (three or more part intertrochanteric fractures with a loss of posteromedial cortical buttress and reverse obliquity fractures)
Nonunion of intertrochanteric fracture in old patient
Malunion of intertrochanteric fracture with arthritis of hip joint
Elderly patient of intertrochanteric fracture with coexisting hip arthritis.
Exclusion criteria were as follows:
Preinjury status nonambulatory
Open fractures
Severely moribund patients
Senile dementia
Any evidence of previous infection.
Among these 18 patients, 12 patients were treated by bipolar hemiarthroplasty whereas 6 patients were treated by THA. In bipolar hemiarthroplasty, Group 5 patients were treated by uncemented and rest seven by cemented hemiarthroplasty, whereas in total arthroplasty, Group 4 patients treated by uncemented while two were by cemented THA. Out of 18 patients, 8 were failed cases of internal fixation. The decision to perform a hemiarthroplasty or a THA was made based on functional demands of the patient and the condition of the acetabular articular cartilage at the time of surgery. Meticulous preoperative templating and careful surgical planning was done. Anteroposterior and lateral radiographs of the femur including the pelvis were taken for all patients. The fractures were classified according to Evans classification. Templates were used to predict the necessary length and diameter of the implant, optimal site of cortical fixation, and proximal femur stem options best suited to reestablish the desired offset and neck length. Assessment of limb length was done using the inter teardrop line and the distance to lesser trochanter.
Operative technique
Patient satisfying above mentioned inclusion criteria were treated by THA if arthritis was present, and by bipolar hemiarthroplasty if arthritis was absent. Exact surgical technique was varied based on whether the reason for performing the arthroplasty was an acute fracture, a neglected fracture, or a nonunion with failed hardware. However, many surgical principles were common place regardless of the preoperative diagnosis. All patients were operated in lateral decubitus position by the posterolateral approach under spinal or general anesthesia. The fibers of the gluteus maximus were split and retracted to expose the short external rotator muscles of the hip. These were divided close to their insertion and an inverted T-shaped incision was made on the joint capsule. In some cases, abundant posterior fracture callus may need to be removed with a saw to gain access to the joint. The femoral head was dislocated out before hardware removal in cases where the fracture had united in failed cases. In cases of nonunion and implant cutout, the internal fixation device was removed first, and the head-neck fragment was extracted. In THA group, a cemented or uncemented acetabular component was implanted after proper preparation and attention were then turned to the femur. The fragments of the greater trochanter were repositioned and temporarily fixed, femoral canal was carefully prepared by graduated reaming using rasps. Because previous fracture and surgery can lead to distortion of the proximal femoral anatomy, medullary canal obstruction, and stress-riser formation, the femoral canal was reamed under C-arm image intensifier guidance. Optimal distal fixation into the normal diaphyseal bone is the goal, so as to allow load transfer and unrestricted weight bearing, trial stem was used to decide the appropriate length of the extramedullary portion of the femoral component. Second-generation cementing technique was used, fractured greater trochanter was attached to the prosthesis with two to four 16-gauge stainless steel wires. Isolated displaced fragments of the lesser trochanter were not reduced and fixed. Finally, reduction was done, range of motion and stability were checked after reduction. The capsule was repaired followed by reattachment of the short external rotators to the femur. Routine closure was performed, and vacuum drainage was placed in both groups. All patients underwent a routine postoperative physiotherapy protocol starting 2nd day of post-op. Prophylaxis against deep venous thrombosis using low molecular weight heparin was started 12 h prior to the operation and continued for 35 days postoperatively.
Follow-up
All patients were followed up clinically and radiographically at 2 weeks, 6 weeks, 3 months, 6 months, 1 year, and annually thereafter. The clinical status at the time of last follow-up was calculated using the Harris hip score (HHP), WOMAC score, and SF 12 score. Loosening of uncemented acetabular components was defined as implant migration, a complete radiolucent line at the implant-bone interface or fixation-screw breakage. At each follow-up visit, a clinic radiological examination was done, and the patient was evaluated using the HHS and was graded as <70 poor, 70-79 fair, 80-89 good, and 90-100 excellent. Anteroposterior radiographs of the hip were analyzed at each follow-up to note evidence of loosening.
Results
In our study, 18 patients were included. Among these, 12 patients were treated by bipolar hemiarthroplasty (8 cemented and 4 uncemented) whereas 6 patients were treated by total hip replacement (4 cemented and 2 uncemented). In this study, patients were 40-80 years of age, average period of follow-up was 12 months. After 12 months follow-up, the mean HHP for hips having bipolar prosthesis was 82.52 points and for the hips having total hip prosthesis, it was 82.95 points. Mean WOMAC score for preoperative patients in bipolar and THA series was 84.02 and 86.66, respectively, which improved to 42.58 and 47.46, respectively, at 1-year of follow-up [Table 1]. In our study, two patients have superficial wound infection which was cured with dressing and antibiotic treatment. In bipolar hemiarthroplasty group, average surgery duration was 95 min, blood loss of 315 ml, and mean hospital stay 14.2 days. While in THA group, average surgery duration of 152 min, mean hospital stay 16.5 days, and blood loss of 565 ml [Table 2]. After 12 months, 100% of cemented THA group has good outcome, 75% of uncemented THA group have excellent to good result, 71.5% of cemented bipolar group have good to excellent outcome whereas 80% of uncemented bipolar group have good to excellent outcome [Table 3]. No intraoperative fractures occurred, and there were no cases of nerve palsy seen. Deep vein thrombosis found in one uncemented bipolar hemiarthroplasty group cases, which managed successfully. At last follow-up, 12 patients were walking without any aid, three patients had a limp and used a stick for walking, and one patient used a walker. Seven patients had shortening of the operated limb with an average shortening of 1.5 cm (range, 5-20 mm) which was well compensated by giving a shoe raise. Three patients have lengthening of operative limb of 1.0 cm. All patients' demonstrated clinically significant pain relief and return to ambulation after the surgery, there were no dislocation, loosening, or late infection seen.

Discussion
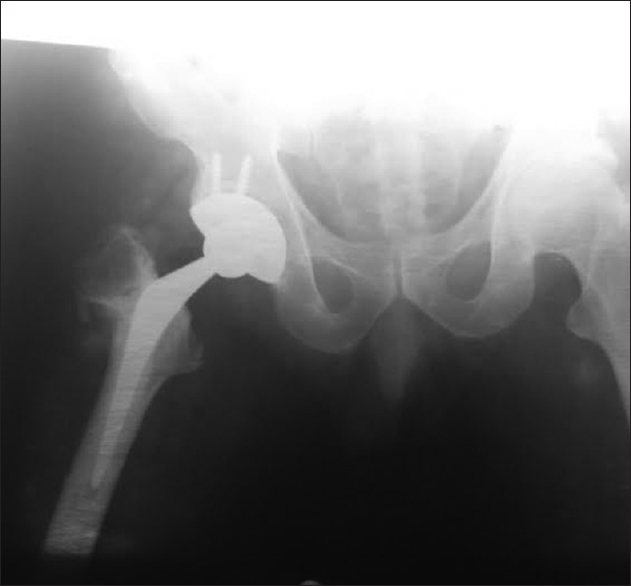
Hip fractures are associated with notable morbidity and mortality in elderly patients. About 35-40% of all intertrochanteric hip fractures are unstable three- and/or four-part configurations with displacement of the posterior medial cortex.[4] The dynamic hip screw and proximal femoral nail have been commonly used for internal fixation of intertrochanteric fractures with good or excellent results.[28] The failure rate of unstable intertrochanteric fractures with osteoporosis has been reported to be between 4% and 16.5%.[4,5,29] The failure rate of the dynamic hip screw is 6.8-9.8%[30] while failure rate of the proximal femoral nail is between 7.1% and 12.5%.[31,32] The incidence of general complications as pulmonary embolism, deep venous thrombosis, and pneumonia ranges from 22% to 50%[33] Comminution, osteoporosis, and instability often preclude the early resumption of full weight-bearing and worsen the prognosis. Use of primary THA and hemiarthroplasty is documented to treat unstable intertrochanteric fractures in an effort to mobilize the patients more rapidly and avoid complications of hip screw migration and general complication.[34,35,36,37] Tronzo claimed to be the first to use long, straight-stemmed prosthesis for the primary treatment of intertrochanteric fractures.[38] Rosenfeld and Schwartz reported good results with the use of the Leinbach prosthesis. Rodop et al.,[39] in a study of primary bipolar hemiprosthesis for unstable intertrochanteric fractures in 37 elderly patients, obtained 17 excellent (45%) and 14 good (37%) results after 12 months according to the HHP-scoring system. Faldini et al. reported the use of hemiarthroplasty and THA in 54 patients[40] and the finding that hip replacement permits a more rapid recovery with immediate weight-bearing and facilitates nursing care better than other fixation techniques. Haentjens et al.[37] reported on a series of 100 patients, 75 years of age or older, who were treated with either a cemented bipolar arthroplasty (91 patient) or THA (9 patients) for an unstable intertrochanteric or subtrochanteric fracture. Good to excellent results were noted in 78% of patients; however, 45% of THA patients sustained a hip dislocation, compared with 3% in the bipolar group. Other complications included loss of greater trochanteric fixation in four cases, one fracture distal to femoral component, and one femoral nonunion. In our study, 12 patients of unstable intertrochanteric fracture [Figure 1] were operated by bipolar hemiarthroplasty [Figure 2]. According to HHP, 75% of bipolar hemiarthroplasty group had excellent to good outcome (mean HHP 82.52). No any chest infection, fat embolism, dislocation, and no any fracture around the stem noted whereas one case of bed sore and two cases of superficial surgical wound infection occurred which were managed successfully with dressing and antibiotic treatment.

- A 68-year-old female of unstable intertrochanteric fracture femur right sides
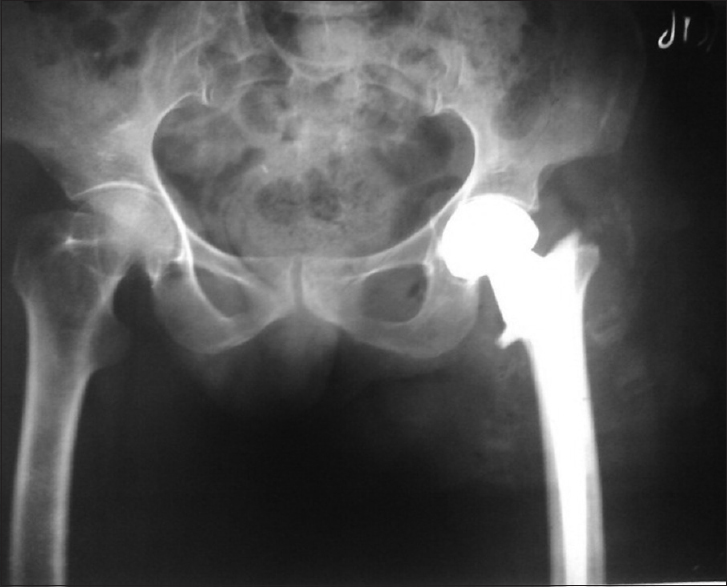
- A case of 68-year-old female of unstable intertrochanteric fracture femur treated by cemented bipolar hemiarthroplasty
In failed treatment cases, there are two treatment options available, one is reification and the other is arthroplasty such as THA and bipolar hemiarthroplasty.[4,5,41] The treatment for failed internal fixation of intertrochanteric fractures is challenging. Most surgeons prefer refixation for young patients and even for active elderly patients with adequate bone quality. However, many elderly patients have poor bone quality, osteoporosis, limb shortening, and damaged cartilage of the femoral head and acetabulum due to penetrating and scratching cartilage by the previous implant.[37,42] where salvage hip arthroplasty preferred. Some authors report excellent results with bipolar hemiarthroplasty for salvage treatment[41] while others report better outcome with THA
Hip arthroplasty for salvage has many technical challenges to be overcome.[4,5] Failed internal fixation implants with or without broken screws must be removed. Nonunion fragments must be mobilized before removal. Careful dissection of scar tissue and calcar-replacement implants or long stems are usually needed,[4,5] and complications such as intraoperative fractures and postoperative dislocations are still common. However, many authors have reported favorable results with arthroplasty. Haidukewych and Berry[4,5,41] studied the results of hip arthroplasty in sixty patients of failed internal fixation treated between 1985 and 1997. About 32 total hip arthroplasties and 27 bipolar hemiarthroplasty were performed. The 7-year survivorship of the arthroplasties free of revision for any reason was 100%; 10-year survivorship was 88%. Serious complications were uncommon, and most patients' ambulatory status and pain were markedly improved. In our study, results were comparable to above study as eight patients of failed intertrochanteric cases [Figure 3] out of which two patients were treated by cemented bipolar hemiarthroplasty and six patients were treated by cemented/uncemented THA [Figure 4]. After 12 months follow-up, all patients were ambulatory, there were no hip dislocation, loosening of implant occur, no any serious complication occurred.

- A 56-year-old male patient of failed case of intertrochanteric fracture femur treated by dynamic hip screw 1 year back
- A 56-year-old male patient of failed case of intertrochanteric fracture femur treated by dynamic hip screw 1 year back treated by uncemented total hip arthroplasty
In a study conducted by Thakur et al.,[43] patients with failed internal fixation were subsequently treated by cementless modular hip arthroplasty. They evaluated 15 elderly patients treated with a tapered, fluted, modular, distally fixing cementless stem. At an average follow-up of 2.86 years, mean HHP improved from 35.90 preoperatively to 83.01. In our study, results were comparable to above study as six patients of failed intertrochanteric fracture were operated by THA, average age of THA group was 58.16 years. Average operation time in this group was 152 min whereas average blood loss was 565 ml. All patients provided postoperative blood transfusion, mean haris hip score improved from preoperative 36.12 to 82.95 12 months postoperative follow-up. In the present study, operating time and blood loss in the THA group were slightly higher than those in the bipolar hemiarthroplasty group. Many authors report that operating time and blood loss in conversion to THA were only slightly higher than those in primary THA.[44] However, the increased blood loss and longer operating time associated with THA did not increase the mortality rate and complications.[45] On the basis of the results of our study, hip arthroplasty with either bipolar or total endoprosthesis seems to be a satisfactory salvage procedure after failed treatment of an intertrochanteric fracture or as a primary intervention in unstable intertrochanteric femur fracture.
Conclusion
Arthroplasty does provide a stable, pain-free, and mobile joint with acceptable complication rate in unstable intertrochanteric fracture femur and in failed intertrochanteric fracture femur cases as seen in our study. Limitations of our study are small number of cases and short follow-up periods, so a larger prospective randomized study with large number of cases and larger follow-up periods are needed further.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Hip fractures are an increasingly important public health problem. Clin Orthop Relat Res. 1998;348:2..
- [Google Scholar]
- The significance and a comparative analysis of the epidemiology of hip fractures. Clin Orthop Relat Res (152):35-43.
- [CrossRef] [Google Scholar]
- Unstable intertrochanteric fractures of the hip. Treatment with ender pins compared with a compression hip-screw. J Bone Joint Surg Am. 1988;70:1297-303.
- [CrossRef] [Google Scholar]
- Hip arthroplasty for salvage of failed treatment of intertrochanteric hip fractures. J Bone Joint Surg Am 2003:85-904.:899-904.
- [CrossRef] [PubMed] [Google Scholar]
- Salvage of failed internal fixation of intertrochanteric hip fractures. Clin Orthop Relat Res (412):184-8.
- [CrossRef] [PubMed] [Google Scholar]
- Primary hemiarthroplasty for unstable osteoporotic intertrochanteric fractures in the elderly: A retrospective case series. Indian J Orthop. 2010;44:428-34.
- [CrossRef] [PubMed] [Google Scholar]
- Unstable intertrochanteric hip fractures in the elderly. J Am Acad Orthop Surg. 2004;12:179-90.
- [CrossRef] [PubMed] [Google Scholar]
- Fracture and dislocation classification compendium - 2007: Orthopaedic trauma association classification, database and outcomes committee. J Orthop Trauma. 2007;21(10 Suppl):S1-133.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of osteoporotic fractures. Scand J Surg. 2002;91:140-6.
- [CrossRef] [PubMed] [Google Scholar]
- The fixation and prognosis of trochanteric fractures. A randomized prospective controlled trial. Clin Orthop Relat Res. 1990;254:242-6.
- [CrossRef] [Google Scholar]
- Fixed nail plates versus sliding hip systems for the treatment of trochanteric femoral fractures: A meta analysis of 14 studies. Injury. 1999;30:157-63.
- [CrossRef] [PubMed] [Google Scholar]
- The stability of intertrochanteric fractures treated with a sliding screw-plate. J Bone Joint Surg Br. 1990;72:37-40.
- [CrossRef] [PubMed] [Google Scholar]
- Changing methods of hip fracture osteosynthesis in Sweden. An epidemiological enquiry covering 46,900 cases. Acta Orthop Scand. 1993;64:173-4.
- [CrossRef] [PubMed] [Google Scholar]
- Trochanteric fractures. Mobility, complications, and mortality in 607 cases treated with the sliding-screw technique. Clin Orthop Relat Res. 1990;260:232-41.
- [CrossRef] [Google Scholar]
- Comparison of compression hip screw and gamma nail for treatment of peritrochanteric fractures. J South Orthop Assoc. 1997;6:173-9.
- [Google Scholar]
- The Gamma nail for peritrochanteric fractures. J Bone Joint Surg Br. 1992;74:340-4.
- [CrossRef] [PubMed] [Google Scholar]
- Intertrochanteric femoral fractures. Mechanical failure after internal fixation. J Bone Joint Surg Br. 1990;72:26-31.
- [Google Scholar]
- Failure of intertrochanteric fracture fixation with a dynamic hip screw in relation to pre-operative fracture stability and osteoporosis. Int Orthop. 2001;25:360-2.
- [CrossRef] [PubMed] [Google Scholar]
- Unstable trochanteric fractures treated with the sliding screw-plate system. A biomechanical study of unstable trochanteric fractures. III. Acta Orthop Scand. 1978;49:392-7.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis of six hundred and twenty-two intertrochanteric hip fractures. J Bone Joint Surg Am. 1979;61:216-21.
- [CrossRef] [Google Scholar]
- Comparative study of treatment of intertrochanteric fractures of femur with long-stem bipolar prosthetic replacement versus dynamic hip screw fixation. Pb Journal of Orthopaedics. 2009;XI(1)
- [Google Scholar]
- Treatment of unstable peritrochanteric fractures in elderly patients with a compression hip screw or with the Vandeputte (VDP) endoprosthesis: A prospective randomized study. J Orthop Trauma. 1995;9:292-7.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of cutout of a lag screw of a dynamic hip screw in an intertrochanteric fracture. Arch Orthop Trauma Surg. 1998;117:193-6.
- [CrossRef] [PubMed] [Google Scholar]
- Total hip arthroplasty following failed fixation of proximal hip fractures. Indian J Orthop. 2008;42:279-86.
- [CrossRef] [PubMed] [Google Scholar]
- Total hip arthroplasty following failure of dynamic hip screw fixation of fractures of the proximal femur. Acta Orthop Belg. 2008;74:788-92.
- [Google Scholar]
- Total hip arthroplasty after prior surgical treatment of hip fracture is it always challenging? J Arthroplasty. 2012;27:31-6.
- [CrossRef] [PubMed] [Google Scholar]
- Stabilisation of unstable trochanteric femoral fractures. Dynamic hip screw (DHS) with trochanteric stabilisation plate vs. proximal femur nail (PFN) Unfallchirurg. 2003;106:39-47.
- [Google Scholar]
- Better functional outcome of salvage THA than bipolar hemiarthroplasty for failed intertrochanteric femur fracture fixation. Orthopedics. 2010;33:721..
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of the compression hip screw with the Medoff sliding plate for intertrochanteric fractures. Clin Orthop Relat Res (348):79-86.
- [CrossRef] [Google Scholar]
- Prospective randomized controlled trial of an intramedullary nail versus dynamic screw and plate for intertrochanteric fractures of the femur. J Orthop Trauma. 2001;15:394-400.
- [CrossRef] [PubMed] [Google Scholar]
- The AO/ASIF-proximal femoral nail (PFN): A new device for the treatment of unstable proximal femoral fractures. Injury. 1999;30:327-32.
- [Google Scholar]
- Hip fracture mortality. Relation to age, treatment, preoperative illness, time of surgery, and complications. Clin Orthop Relat Res. 1984;186:45-56.
- [CrossRef] [Google Scholar]
- Cemented hemiarthroplasties for elderly patients with intertrochanteric fractures. Clin Orthop Relat Res. 2000;371:206-15.
- [CrossRef] [PubMed] [Google Scholar]
- Bipolar prosthetic replacement for the management of unstable intertrochanteric hip fractures in the elderly. Clin Orthop Relat Res. 1987;224:169-77.
- [CrossRef] [Google Scholar]
- Comminuted intertrochanteric fractures treated with a Leinbach prosthesis. Clin Orthop Relat Res. 1987;218:75.
- [CrossRef] [Google Scholar]
- Treatment of unstable intertrochanteric and subtrochanteric fractures in elderly patients. Primary bipolar arthroplasty compared with internal fixation. J Bone Joint Surg Am. 1989;71:1214-25.
- [CrossRef] [Google Scholar]
- The use of an endoprosthesis for severely comminuted trochanteric fractures. Orthop Clin North Am. 1974;5:679-81.
- [CrossRef] [PubMed] [Google Scholar]
- Primary bipolar hemiprosthesis for unstable intertrochanteric fractures. Int Orthop. 2002;26:233-7.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical treatment of unstable intertrochanteric fractures by bipolar hip replacement or total hip replacement in elderly osteoporotic patients. J Orthop Traumatol. 2006;7:117-21.
- [CrossRef] [Google Scholar]
- Long-term survivorship of cemented bipolar hemiarthroplasty for fracture of the femoral neck. Clin Orthop Relat Res (403):118-126.
- [CrossRef] [PubMed] [Google Scholar]
- Nonunion of intertrochanteric fractures of the femur following open reduction and internal fixation. Results of second attempts to gain union. Clin Orthop Relat Res. 1987;218:81..
- [CrossRef] [Google Scholar]
- Management of failed trochanteric fracture fixation with cementless modular hip arthroplasty using a distally fixing stem. J Arthroplasty. 2011;26:398-403.
- [CrossRef] [PubMed] [Google Scholar]
- Total hip arthroplasty following failed internal fixation of hip fractures. Clin Orthop Relat Res (269):32-7.
- [CrossRef] [Google Scholar]
- A randomised controlled trial comparing bipolar hemiarthroplasty with total hip replacement for displaced intracapsular fractures of the femoral neck in elderly patients. J Bone Joint Surg Br. 2007;89:160-5.
- [CrossRef] [PubMed] [Google Scholar]




