
Translate this page into:
Recommendations for Appropriate Use of Tranexamic Acid in Total Hip Arthroplasty
Address for correspondence: Dr. Sohael Khan, Department of Orthopedics, Jnmc, Wardha, Maharashtra, India. E-mail: sunilnikose@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Nikose SS, Jain SS, Nikose D, Saoji K, Khan S, Vijan K. Recommendations for appropriate use of tranexamic acid in total hip arthroplasty. J Orthop Spine 2020;8:91-5.
Abstract
BACKGROUND:
Tranexamic acid (TXA) has gained recent interest in orthopedics and trauma surgery because of its demonstrated benefit in several clinical trials. Prophylactic TXA is a safe, low-cost option to reduce bleeding in patients undergoing total hip replacement (THR), and its optimal dose and duration are unknown. Also, there is still no consensus as to the best form and dosages of the use of TXA. Hence the present study was carried out to determine the appropriate use of TXA, its dosage, timing, and recommendations for the best possible bleeding control in total hip arthroplasty.
AIM AND OBJECTIVES:
Present study was aimed to prove the efficacy of TXA in total hip arthroplasties when compared with a control group, to establish a criterion for the ideal use of TXA, and to identify possible complications.
MATERIAL AND METHODS:
A total of 238 adult patients receiving TXA undergoing replacement of hips since March 2015 were included in the study and divided randomly into four groups. Group one received a single dose of 500 mg TXA before the start of surgery (Preincision) over 10 minutes, group two received a 500 mg TXA 20 minutes prior to surgery in the operation room and just before the start of surgery (Preincision) over 10 minutes, group three received 500 mg TXA 20 minutes prior to surgery in the operation room and 500 mg just before the start of surgery (Preincision) over 10 minutes and then three hours post-surgery and group four (Control group) did not receive any TXA. Total blood loss was calculated using a formula considering hematocrit values and blood transfusions received.
RESULT:
Two hundred and thirty-eight adult patients were included in the study: 60 in group one, 59 in group two, 60 in group three and 59 in group four. All the groups had mean hemoglobin level above10 g/dL. Maximum benefit was observed in group three followed by group one and group two respectively with almost similar outcomes while group four did not show any benefits, thus demonstrating the beneficial effect of TXA regarding hemoglobin decrease postoperatively.
CONCLUSION:
The findings of the present study demonstrated that the use of TXA in THA reduced the incidence of perioperative bleeding and, consequently, a significant reduction in decrease in serum hemoglobin was observed in groups one, two, and three when compared to the group four control. Therefore, there was a reduction in the need for blood transfusion. Thus the maximum beneficial effect of TXA was observed in group three followed by group one and group two which had a similar outcome while group four did not show any benefits.
Keywords
Blood transfusions
hematocrit values
precision
total blood loss
total hip replacement
tranexamic acid

Introduction
Total hip arthroplasty (THA) is an excellent surgical procedure for patients with end-stage hip diseases.[1,2] By 2030, the demand for primary total hip arthroplasties is estimated to grow by 174% to 572,000.[3] However, it is always accompanied by considerable blood loss (BL), which may lead to acute anemia and a series of complications. Bleeding complications may hinder the success of any surgery.[4] Perioperative BL is often treated with blood transfusion, with reported transfusion rates ranging from 11% to 67%.[5,6] Both autologous and allogeneic blood transfusions result in increased costs, carry the risks of disease transmission and transfusion reaction, and have been associated with increased rates of periprosthetic infection.[7]
Numerous approaches have been used to minimize transfusion requirements, including blood salvage, controlled hypotension, hemodilution, and stimulation of erythropoiesis with epoetin alfa, with varying degrees of success reported along with the increased cost. Recently, the use of pharmacologic agents, such as antifibrinolytic tranexamic acid (TXA), to minimize perioperative BL associated with total joint arthroplasty (TJA) has been investigated.
TXA is a type of synthetic amino acid analog, which could block the lysine binding sites on plasminogen to inhibit the activation of plasminogen and interfere with fibrinolysis.[8] TXA is available in intravenous (IV), topical, and oral form. However, it has gained recent interest in orthopedics and trauma surgery because of its demonstrated benefit in several clinical trials. It is inexpensive and effective at reducing BL and blood transfusion requirements without a significant increase in morbidity or mortality. The optimal timing, dosing, and route of administration in orthopedics are yet to be elucidated. Significant investigation of TXA use in joint replacement and spine surgery has promoted its incorporation into the everyday practice of many of these surgeons. The paucity of studies regarding its use in orthopedic trauma has limited its integration into a field that may stand to benefit most from the drug.[9] Therefore, the present study was aimed to prove the efficacy of TXA in total hip arthroplasties when compared with a control group to establish a criterion for the ideal use of TXA and to identify possible complications.
Materials and Methods
A total of 238 adult patients who received TXA and undergoing replacement of hips since March 2015 were enrolled in the study. Inclusion criteria were patients who are undergoing THA. Evidence is lacking for the safe and effective use of TXA in joint revision surgery or use in hip fracture surgery; therefore, the risk/benefit of TXA in these settings is unknown. Avoid IV administration in high-risk patients. Exclusion criteria were patients with hypersensitivity to TXA, coronary or vascular stent placed within the past 6 months (maybe extended to 1 year if appropriate), deep venous thrombosis (DVT), pulmonary embolus (PE), myocardial infarction (MI) or ischemic stroke within the past 6 months (maybe extended to 1 year if appropriate), subarachnoid hemorrhage, bleeding disorders, hypercoagulable state/disorder, retinal vein or artery occlusion, active intravascular clotting, concomitant use of clotting factor concentrates, or anti-inhibitor coagulant concentrates.
The patients were randomly allocated into four groups. Group 1 received a single dose of 500 mg TXA before the start of surgery (preincision) over 10 min. Group 2 received a 500 mg TXA 20 min before surgery in the operation room and just before the start of surgery (preincision) over 10 min. Group 3 received 500 mg TXA 20 min before surgery in the operation room and 500 mg just before the start of surgery (preincision) over 10 min and then 3 h postsurgery. Group 4: Control group did not receive TXA. The primary outcome of the study was total BL and it was calculated using a formula considering hematocrit values and blood transfusions received. Laboratory measurements, including hematocrit and Hb levels, were determined from venous blood samples collected at admission and postoperatively. The mean peri- and postoperative bleeding, hemoglobin decrease, and need for blood transfusion were compared among the four groups.
Statistical analysis
Results were expressed as means ± standard deviations. One-way analysis of variance was used for comparing the means, as this was a comparison of four independent groups. The normality assumptions were verified with the Shapiro–Wilk test, and variance homogeneity was assessed using the Levene test. Finally, the Tukey test was used to assess which differences were statistically significant. Results were considered to be statistically significant when P < 0.05. The statistical analyses were performed with IBM Statistics SPSS version 19 (company IBM, Chicago, Illinois, USA).
Results
Two hundred and thirty-eight adult patients were included in the study: 60 in Group 1, 59 in Group 2, 60 in Group 3 and 59 in Group 4. As shown in Table 1, demographic data and operative variables were comparable between the groups with regard to sex, age, weight, length of incision, and duration of the operation.

All the groups had a mean hemoglobin level >10 g/dL. There was no statistically significant difference observed among groups with respect to preoperative hemoglobin levels, which reduced the chance of interference due to discrepant preoperative hemoglobin values [Table 2]. While after the THA procedure, there was diseased in mean hemoglobin level observed in all the groups, greatest in Group 4 as shown in Table 2. These data reveal a statistically significant hemoglobin decrease in Group 4 in relation to Groups 1, 2, and 3, demonstrating the beneficial effect of TXA regarding hemoglobin decreased postoperatively.

Figure 1 and Table 3 show the comparison of mean total BL over perioperative period among groups. Group 4 presented statistically significant higher BL, while Group 3 had significantly lower BL followed by Group 1 and 2. It suggests a beneficial effect of TXA regarding decreased bleeding. There was no statistically significant difference observed between Groups 1 and 2. Thus, maximum benefit was observed in Group 3 followed by Group 1 and Group 2, which had a similar outcome. Group 4 did not show any benefits. No patient had reported blood transfusion at 1-year follow-up.
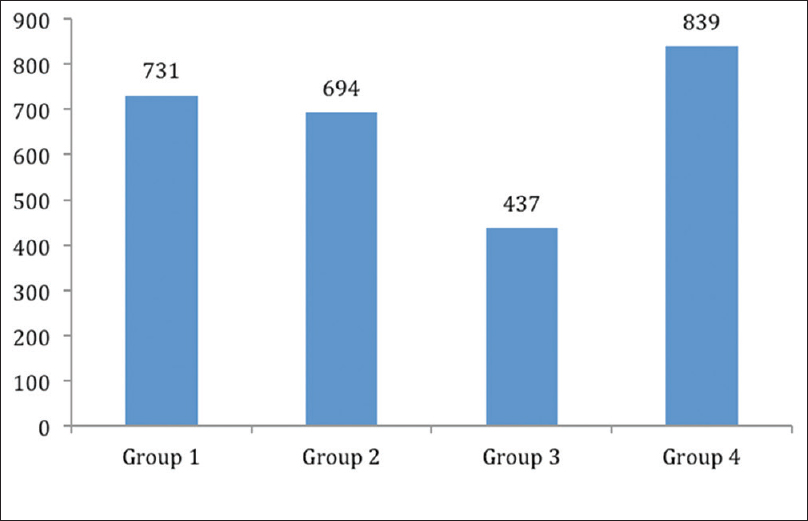
- Mean total blood loss over perioperative period (ml)

Discussion
Major joint arthroplasty and spinal surgery are associated with the potential for significant BL. It is postulated that increased fibrinolysis may contribute to bleeding, in orthopedic surgery, and particularly where tourniquet use is prevalent. Meta-analyses of total hip and knee arthroplasty surgery concluded that TXA reduces both BL and transfusion requirements and is not associated with an increase in thromboembolic events.[10] Evidence exists for the use of IV, intra-articular (IA) or topical irrigation of joint with TXA for reducing total BL and transfusion requirements in orthopedic surgery. Most of the trials used IV bolus dosing (single or repeated) or continuous infusion of TXA as opposed to IA or topical use. Topical irrigation doses of TXA range from 500 mg to 3 g in 50-ml saline. IA doses range from 250 mg to 2 g in 20–50 ml saline.[11] Evidence is insufficient to identify the optimal dose, route of administration, and proper timing of dose. In several of the meta-analyses, a trend towards greater benefit was noted with higher doses of TXA. However, very high doses of TXA have rarely been associated with seizures.[12]
When comparing the route of administration, topically applied TXA was initially investigated to circumvent the theoretically increased risk of thromboembolic events with IV systemic delivery.
In large prospective studies and meta-analyses, topical application decreases BL, transfusion requirements, postoperative drainage, and decline in hemoglobin without increasing the risk for DVT or pulmonary embolism.[13] Another study safely added dilute epinephrine to topical TXA and found an additive effect that was superior to TXA alone.[14] In the present study, we selected the topical dose (single or repeated) of TXA was 500 mg. The timing of the TXA dose appears to play a role in its effect on BL in patients undergoing TJA. Furthermore, the value of re-dosing TXA is more apparent than is the dose required for optimal benefit. Furthermore, with regard to timing, convincing evidence exists for the use of an initial dose given before the beginning of the procedure, with at least one repeated dose. This recommendation is also consistent with published pharmacokinetics.
The most important finding of the present study was that there were significant differences in efficacy between the single-dose of TXA (Group 1) and the multiple-dose regimen (Group 3). Our finding conflicts with the traditional view that a single dose application of TXA is not as effective as a multiple-dose regime to reduce allogeneic transfusions in total hip replacement.[15] In a study of patients who underwent noncemented primary THA with a variety of dosing regimens, Imai et al.[16] reported that a TXA dose administered 10 min before surgery rather than 10 min before closure substantially reduced intraoperative BL. Furthermore, in groups that received a preoperative TXA dose, estimated actual BL, drain output, hemoglobin reduction on the postoperative day 1, and maximum hemoglobin reduction were all substantially lower than in the control group. Postoperative BL was also lower in the group that received a preoperative dose and a second dose 6 h later than in the group that received a dose 10 min before closure and another dose 6 h later.
In the current study, there was a statistically significant hemoglobin decrease in group 4 in relation to Groups 1, 2, and 3, demonstrating the beneficial effect of TXA regarding hemoglobin decreased postoperatively. The total BL was significantly lower in Group 3 that received a dose 20 min before surgery in the operation room and just before the start of surgery over 10 min and then 3 h postsurgery. Group 1 that received a single-dose of TXA before the start of surgery over 10 min, and Group 2 that received TXA 20 min before surgery and just before the start of surgery over 10 min had nearly similar amount of BL but higher as compared to Group 3 and lower than Group 4 (Group 4 that not receive TXA). Hence, it suggests a beneficial effect of TXA regarding decreased bleeding. Zhou et al.[17] have shown that TXA reduced BL and transfusion requirements in patients undergoing THA.
In elective surgery, TXA reduces the need for blood transfusion by approximately 30%, without affecting mortality or increasing postoperative complications. We did not observe any serious adverse events directly related to TXA administration. No major bleeding complications emerged in the immediate postoperative period. No patient returned to the operating room for evacuation and debridement of hematoma. Furthermore, no patients died, and there were no occurrences of major TE, including proximal DVT, PE, MI, and cerebrovascular accident, in either group. No deep periprosthetic infections had been identified by 1-year follow-up. There are little data regarding the adverse effects of this drug. It rarely causes hypotension and retinal alteration. Its prolonged systemic use increases the risk of thromboembolic phenomena; it is contraindicated in acute thrombopathies and should be used with caution in patients with a known tendency for thrombosis.[18] Studies on the use of TXA showed interesting results, but its benefits in THA have not been well established.[19]
Conclusion
The findings of the present study demonstrated that the use of TXA in THA reduced the rates of perioperative bleeding, and consequently, significant decreased in serum hemoglobin was observed in Groups 1, 2, and 3 when compared to Group 4 (control: did not receive TXA). Therefore, there was a reduction in the need for blood transfusion. Thus the maximum beneficial effect of TXA was observed in Group 3 followed by Group 1 and Group 2, which had similar outcome, while Group 4 did not show any benefits.
The study suggested that TXA has become a significant tool in reducing perioperative BL, transfusion requirements, and morbidity in patients across multiple specialties. Its indications have continued to expand as its effectiveness and safety endure the growing list of applications, particularly in orthopedic surgery. Although questions remain about optimal timing, dosing, patient limitations, and route of administration, overwhelming evidence supports its use as a cost-effective measure in blood management, and routine use is likely in the future.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Orthopaedic surgeon workforce and volume assessment for total hip and knee replacement in the United States: Preparing for an epidemic. J Bone Joint Surg Am. 2008;90:1598-605.
- [CrossRef] [PubMed] [Google Scholar]
- Mortality, cost, and downstream disease of total hip arthroplasty patients in the medicare population. J Arthroplasty. 2014;29:242-6.
- [CrossRef] [PubMed] [Google Scholar]
- Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89:780-5.
- [CrossRef] [PubMed] [Google Scholar]
- Prophylactic use of tranexamic acid in cardiac surgery performed with the aid of extracorporeal circulation. 2000:97. Dissertation (master's degree) - State University of Campinas, Faculty of Medical Sciences, Campinas, SP
- [Google Scholar]
- An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am. 1999;81:2-10.
- [CrossRef] [PubMed] [Google Scholar]
- Predicting need for allogeneic transfusion after total knee arthroplasty. J Arthroplasty. 2012;27:961-7.
- [CrossRef] [PubMed] [Google Scholar]
- Allogeneic blood transfusions and postoperative infections after total hip or knee arthroplasty. J Bone Joint Surg Am. 2014;96:272-8.
- [CrossRef] [PubMed] [Google Scholar]
- Antifibrinolytics in major orthopaedic surgery. J Am Acad Orthop Surg. 2010;18:132-8.
- [CrossRef] [PubMed] [Google Scholar]
- Application of tranexamic acid in trauma and orthopedic surgery. Orthop Clin North Am. 2016;47:137-43.
- [CrossRef] [PubMed] [Google Scholar]
- Low risk of thromboembolic complications with tranexamic acid after primary total hip and knee arthroplasty. Clin Orthop Relat Res. 2013;471:150-4.
- [CrossRef] [PubMed] [Google Scholar]
- Use of topical tranexamic acid or aminocaproic acid to prevent bleeding after major surgical procedures. Ann Pharmacother. 2012;46:97-107.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2013/019281s031lbl.pdf. (accessed )
- Topical application of tranexamic acid in primary total hip arthroplasty: A systemic review and meta-analysis. Int J Surg. 2015;15:134-9.
- [CrossRef] [PubMed] [Google Scholar]
- Topical application of tranexamic acid plus diluted epinephrine reduces postoperative hidden blood loss in total hip arthroplasty. J Arthroplasty. 2015;30:2196-200.
- [CrossRef] [PubMed] [Google Scholar]
- Do antifibrinolytics reduce allogeneic blood transfusion in orthopedic surgery? Anesthesiology. 2006;105:1034-46.
- [CrossRef] [PubMed] [Google Scholar]
- Tranexamic acid for reduction of blood loss during total hip arthroplasty. J Arthroplasty. 2012;27:1838-43.
- [CrossRef] [PubMed] [Google Scholar]
- Do we really need tranexamic acid in total hip arthroplasty? A meta-analysis of nineteen randomized controlled trials. Arch Orthop Trauma Surg. 2013;133:1017-27.
- [CrossRef] [PubMed] [Google Scholar]
- Hereditary hemorrhagic telangiectasia: tranexamic acid in the treatment of plantar ulcers. Brazilian annals of dermatology.. 2005;80:S373-5.
- [CrossRef] [Google Scholar]
- Tranexamic acid in total hip arthroplasty saves blood and money: A randomized, double-blind study in 100 patients. Acta Orthop. 2005;76:314-9.
- [CrossRef] [PubMed] [Google Scholar]




