
Translate this page into:
Rapidly progressive hip disease masquerading as Gorham′s syndrome of the femoral head
Address for correspondence: Dr. Atul Mahajan, G-22, Bali Nagar, New Delhi - 110 015, India. E-mail: dratulmahajan84@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Mahajan A, Kataria H. Rapidly progressive hip disease masquerading as Gorham's syndrome of the femoral head. J Orthop Allied Sci 2016;4:95-7.
Abstract
Rapidly destructive hip disease (RDHD) is a rare syndrome of unknown etiology, resulting in rapid deterioration of both the femoral and acetabular aspects of the hip joint with disappearance of the femoral head. Differential diagnosis should include those conditions known to potentially lead to rapid hip destruction, such as septic arthritis, metabolic bone diseases, autoimmune inflammatory arthritis, malignancy, and classical osteonecrosis. Sequential X-rays in patients with fast worsening of hip symptoms and a high degree of clinical suspicion seem mandatory to avoid extensive joint destruction and facilitate better arthroplasty outcomes in these patients. Because of the degree of joint deformity and the patient's level of disability, the typical treatment of rapidly destructive arthropathy is total hip arthroplasty. In this report, we present a clinical case of left RDHD offering a useful review for the diagnosis and management of this condition.
Keywords
Chondrolysis
Gorham′s disease
osteoarthritis
osteonecrosis
rapidly destructive hip disease
total hip replacement

Introduction
Rapidly destructive hip disease is a rare syndrome of unknown etiology and distinct from ischemic necrosis of the femoral head, resulting in rapid deterioration of both the femoral and acetabular aspects of the hip joint with disappearance of the femoral head. We report a case where there was disappearance of the femoral head within 10 weeks and after excluding all the possible causes clinically and radiologically, it was considered to be a case of Gorham's syndrome of the femoral head, and diagnosis of RDHD was made based on histological findings.
Case Report
A 66-year-old male presented with right groin and lateral thigh pain of 10 weeks duration. He was limping because of pain and his daily activities were restricted. The patient was unable to walk for long distances, unable to squat and sit cross-legged. He had tried multiple nonsteroidal anti-inflammatory drugs with only partial relief of his pain. Medical history was notable for hypertension and Type 2 diabetes mellitus on treatment. He had no other risk factors for osteonecrosis. At his initial presentation, he ambulated with an antalgic gait with short stance on the right side. He had limited range of motion right hip with flexion, abduction, and internal rotation more severely affected. Mild trochanteric tenderness was present on the right side. There was 3 cm shortening on the right side. He had no spinous tenderness and a negative straight leg raise bilaterally. Neurologic examination revealed 5/5 strength and intact sensation in lower extremities, with 2+ knee and ankle jerk reflexes bilaterally. Laboratory studies, including a complete blood count with differential, erythrocyte sedimentation rate, C-reactive protein, and human leukocyte antigen-B27, were done which were normal. Aspiration of the right hip was done which was negative. Blood cultures were also negative. An anteroposterior pelvis radiograph obtained [Figure 1] showed nonvisualization of the femoral head with mild superior subluxation of the femoral neck on the right side. Triple-phase bone scan using 20 mci of 99 mTc-MDP was done which showed increased vascularity and bony uptake in the region of right hip involving acetabulum and head, neck, and proximal shaft of right femur. Computerized tomography scan of the right hip [Figure 2] showed complete destruction of the right femoral head. Femoral neck was articulating with acetabular roof. Femoral articular surface was irregular and sclerosed with sclerosis and mild flattening of the right acetabular roof. Based on the radiographic findings and laboratory studies, a diagnosis of rapidly destructive arthropathy was made. The patient underwent reverse hybrid total hip replacement of the right side [Figure 3] using posterior moore's approach, and BIOMET implant was used (Type-1 7.5 × 135 mm uncemented stem, size #48 cemented cup, and size #21 acetabular liner). Intraoperatively, total destruction of the femoral head was noted. Acetabulum also showed degenerative cartilage changes, though not in proportion with changes in the femoral head. Cultures and microscopic evaluation of the fluid obtained during surgery were negative. Biopsy showed features of ischemic necrosis and hemorrhage within necrotic areas and bony trabeculae. Postoperative course was uneventful. At the last follow-up, there were no clinical or radiological signs of progression or recurrence of the disease.
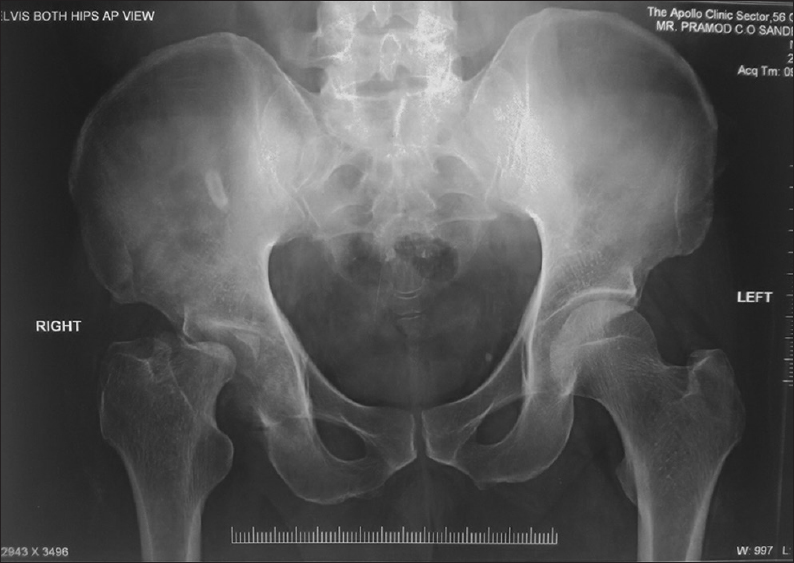
- X-ray of the pelvis with bilateral hips in anteroposterior view showing non visualization of the right femoral head with mild superior subluxation of the femoral neck
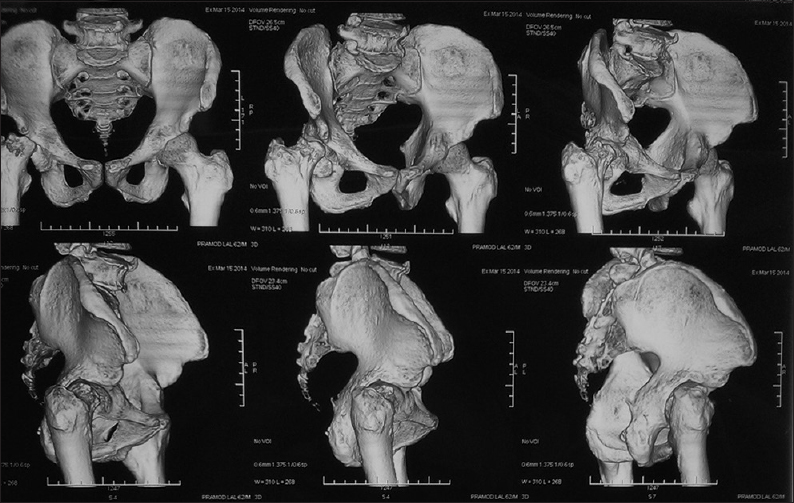
- Computed tomography scan of the pelvis with bilateral hips with three-dimensional image reconstruction showing non visualization of the right femoral head
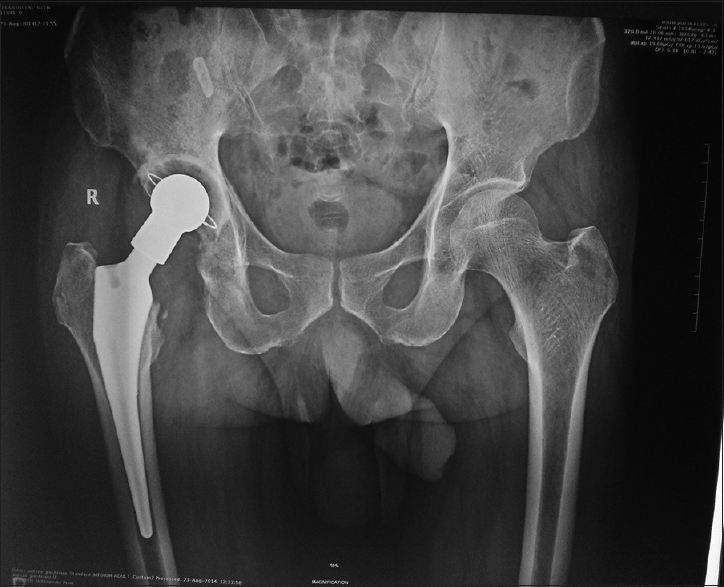
- X-ray of the pelvis with bilateral hips in anteroposterior view showing reverse hybrid total hip replacement of the right side
Discussion
RDHD is a rare disorder and was first described by Forestier in 1957.[1] It is characterized by intraoperative technical difficulty due to significant bone loss, increased blood loss during surgery with increased operating times, and need for special implants making joint reconstruction challenging in these patients. Overall results are adversely affected by any acetabular defect, and this is certainly the main technical problem with rapidly progressive cases.[2] Therefore, there is a need for early diagnosis of this rapidly destructive hip osteoarthritis. Follow-up radiographs in a few months of the onset of symptoms demonstrate destruction of the femoral head and acetabulum with sclerosis, subchondral cysts, and minimal or no osteophytes. However, the rapid progression of this disease makes it difficult to obtain sequential radiographs in its early stages.[3] Subchondral bone ischemia and cell necrosis recently have been emphasized as major factors in the development of RDHD by Mitrovic and Riera.[4] It is essentially a diagnosis of exclusion. We ruled out septic arthritis (on the basis of laboratory studies and joint aspiration) and neuropathic arthropathy (in the setting of an underlying neurologic disorder) as both of these diagnoses are associated with worse outcomes following total hip arthroplasty.[5] In inflammatory arthritis, joint destruction is accompanied by formation of a large pannus which was not seen in this case. Several types of crystal-induced arthropathy can also cause rapid hip destruction.[5] Detection of crystals in the joint fluid confirms the diagnosis and was negative in our patient.
Gorham-Stout disease is a spontaneous, massive, and nonfamilial idiopathic osteolysis. Lymphatic and neovascular tissue extensively replace bone tissue, therefore, Hagendoorn[6] suggested that the signaling pathway of the platelet-derived growth factor-BB (receptor of the lymphangiogenic growth factor: PDGFR-b) could play some role in pathogenesis. Biopsy reviews reveal an excessive intraosseous nonmalignant proliferation of small vessels, resulting in bone resorption, and may extend to adjacent bones and soft tissues.[7] These lesions are progressively replaced by extensive fibrosis. Osteolysis[8] is concentric in long bones. Although clinically and radiologically our patient seemed to be having Gorham's syndrome, histological findings showed evidence of ischemic necrosis and hemorrhages with no osteoclastic activity and no fibrotic proliferation. Because of the degree of joint deformity and the patient's level of disability, the typical treatment of rapidly destructive arthropathy is total hip arthroplasty. Our patient underwent reverse hybrid total hip replacement of involved side and is having an uneventful course.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Coxites rheumatic, subacute and chronic (study of 180 observations, test classification of certain isolated hip disease. In: Thesis. 1957.
- [Google Scholar]
- Risk factors affecting radiological failure of the socket in primary Charnley low friction arthroplasty. A 10-to 20-year followup study. Clin Orthop Relat Res (306):84-96.
- [Google Scholar]
- Early MRI findings of rapidly destructive coxopathy. Magn Reson Imaging. 2001;19:47-50.
- [CrossRef] [PubMed] [Google Scholar]
- Synovial, articular cartilage and bone changes in rapidly destructive arthropathy (osteoarthritis) of the hip. Rheumatol Int. 1992;12:17-22.
- [CrossRef] [PubMed] [Google Scholar]
- Rapidly destructive hip disease: Clinical and imaging abnormalities. Radiology. 1993;186:461-6.
- [CrossRef] [PubMed] [Google Scholar]
- Platelet-derived growth factor receptor-beta in Gorham′s disease. Nat Clin Pract Oncol. 2006;3:693-7.
- [CrossRef] [PubMed] [Google Scholar]
- Disappearing bone disease. A clinical and histological study. J Bone Joint Surg Am. 1977;59:57-61.
- [CrossRef] [Google Scholar]
- The Gorham-Stout syndrome (Gorham′s massive osteolysis). A report of six cases with histopathological findings. J Bone Joint Surg Br. 1999;81:501-6.
- [CrossRef] [Google Scholar]




