
Translate this page into:
Primary Intramedullary Nailing in Compound Type 1 and 2 Femur Shaft Fractures and Their Effect on Functional Outcome
Address for correspondence: Dr. Prasanna Kumar GS, Departments of Orthopaedics, Grant Government Medical College, Mumbai, Maharashtra, India. E-mail: prasannakumargs5@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Mahajan NP, Kumar GSP, Palange ND, Yadav AK, Harsoor A, Pawar H. Primary intramedullary nailing in compound Type 1 and 2 femur shaft fractures and their effect on functional outcome. J Orthop Spine 2020;8:86-90.
Abstract
Background:
Femur shaft fractures are the most common long bone fractures encountered in orthopedic practice. Open fractures of the femur shaft are due to high-energy trauma; these patients are usually associated with other system injuries and vascular involvement. The initial management of open fractures includes antibiotics, debridement, and stabilization. If the initial debridement is believed to be adequate, definitive fixation of the femoral shaft can be performed usually with reamed intramedullary nailing. The present study was conducted to evaluate the functional outcome in open Type 1 and 2 femur shaft fractures managed with primary intramedullary nailing and the complications related to it.
Materials and Methods:
Twenty-two patients, having Grade 1 and 2 compound femur shaft fractures were admitted and included in the study from January 2016 to February 2019 after obtaining valid consent. All the patients were investigated with X-rays, and fractures were classified according to Gustilo–Anderson classification. All the patients were treated primarily with intramedullary nailing, and the functional outcome was assessed by using Harris Hip Score and Oxford Knee Score.
Results:
Thirteen (59.09%) patients had Type 1 open femur shaft fractures and nine (40.90%) patients had Type 2 fractures. Fracture union was observed in six patients (27.27%) at 3 months and in 16 (72.72%) at 3–6 months. Complications observed were superficial wound infections in two patients, deep infections in two patients, and nonunion in one patient. Thirteen (59.09%) patients got excellent outcome, four (18.18%) patients got good outcome, three (13.63%) patients got fair outcome, and two (09.09%) patients got poor outcome.
Conclusion:
Primary intramedullary nailing is an effective method of managing Type 1 and 2 open femur shaft fractures if thorough early and timely debridement can be done. It is associated with less complications, helps in early mobilisation and also avoids secondary procedures.
Keywords
Compound femur fracture
nailing
outcome

Introduction
Femur shaft fractures are the most common long-bone fractures encountered in orthopedic practice. The evolution and management of femoral shaft fractures continue to evolve on the basis of improved understanding of anatomy, outcome of treatment, and biomechanics of fixation techniques.[1]
Since from the introduction of intramedullary nailing by Kuntscher, patient survival and outcomes have continued to improve.[2] Improved prevention and management of infection, nonunion, and shortening, made the intramedullary nailing the primary line of treatment for most of the femoral shaft fractures. Biomechanical improvements in nail design and instruments have further expanded the indications for nailing.
Open fractures of the femur shaft are due to high-energy trauma; these patients are usually associated with other system injuries and vascular injuries. Because of the thick muscular envelop around the femur shaft, open fracture suggests significant initial displacement and soft-tissue disruption.
The initial management of open fractures includes antibiotics, debridement, and stabilization. A thorough debridement should be performed to decrease the risk of early and late infections.
If the initial debridement is believed to be adequate, definitive fixation of the femoral shaft can be performed usually with reamed intramedullary nailing. Historically, traction and external fixation have been used to definitively treat open femoral shaft fractures, however these methods had numerous disadvantages such as knee stiffness, prolonged immobilization and pin tract infection, shortening, malunion, and nonunions. The delay in stabilization of femoral shaft fractures has been shown to be associated with increased mortality.[3]
The present study was conducted to evaluate the functional outcome in open Type 1 and 2 femur shaft fractures managed with primary intramedullary nailing and the complications related to it.
Materials and Methods
This prospective observational study was conducted at a tertiary care hospital from January 2016 to February 2019, over a period of 3 years. Twenty-two patients, having Grade 1 and 2 compound femur shaft fractures, were admitted and included in the study after obtaining valid consent. Fractures were classified according to the Gustilo–Anderson classification; all the patients were treated primarily with intramedullary nailing and the functional outcome was assessed by using Harris Hip Score and Oxford Knee Score. All data were collected and analyzed by the Epi Info 7 software, developed by the Centers for Disease Control and Prevention in Atlanta, Georgia (USA) and using Chi-square test. P < 0.05 was considered statistically significant.
Inclusion criteria
Patients with Type 1 and type 2 open femoral shaft fractures
Patients who are medically fit for surgery and age >20 years
Patients with polytrauma with Grade 1 and 2 femur shaft fractures.
Exclusion criteria
Closed fractures
Pathological fractures
Medically unfit patients.
Patient evaluation
On admission, detailed history and examination of the patient was done after hemodynamic stabilization which includes screening for head, pelvic, abdominal, and chest injury and are subjected to routine preoperative investigations. X-ray of the involved femur (anteroposterior and lateral view) was taken, and the fractures were classified as per Gustilo–Anderson classification. Fracture was immobilized initially with Thomas splint, and injection tetanus toxoid and injection tetanus immunoglobulin were given to all patients in the emergency room.
Surgical technique
All the patients were operated in supine position on traction table, and the wound was thoroughly debrided and wash was given (3–6 L of normal saline with betadine solution). Foreign bodies, if any, were removed during the debridement procedure and stay suture was taken. Intraoperative samples were sent for culture and sensitivity.
Approach used was the standard nailing approach with pyriform fossa entry. Initially, a guide wire was passed through the entry hole followed by gradual reaming. Simple fractures were reduced indirectly by using nail and the complex comminuted fractures were reduced by manipulation through the fracture wound. Appropriate-sized nail was used to fix the nail with proximal and distal locking. Type 1 wounds were closed primarily at the time of surgery after thorough debridement, clean Type 2 wounds were closed primarily, and doubtful Type 2 wounds were thoroughly debrided during surgery and closed secondarily.
Postoperative protocol
Postoperatively intravenous empirical antibiotics were given depending on the type of compound wound (for Type 1 wound till 1 week, clean Type 2 wound for 1 week, and doubtful Type 2 wound for 3 weeks), latter converted to oral antibiotics till the wound heals.
All the patients were advised to take high-protein diet, and we tried to keep postoperative hemoglobin >12 g% for better wound healing.
Hip and knee range of motions were started on the 2nd postoperative day, and weight bearing was initiated depending on the fracture pattern (on the 2nd day for simple transverse or short oblique fractures and after 3 weeks for complex fractures).
Follow-up
The patients were followed up at 3 weeks, 6 weeks, 3 months, 6 months, and 1 year; assessed for radiological and clinical union and wound status; and observed for complications such as nonunion, malunion, delayed union, implant failure, and infection. The functional outcome was assessed by using Harris Hip Score and Oxford Knee Score.
Results
We studied 22 patients with open Type 1 and Type 2 femur shaft fractures with age range from 20 to 70 years, with a mean age of 45 years (standard deviation 12.51). Fourteen patients (63.63%) were between 20 and 40 years of age, five patients (22.72%) were between 41 and 60 years of age, and three patients (13.63%) were above 60 years; among the total study population, 18 patients were male and four patients were female.
The mode of trauma was road traffic accident in 19 (86.36%) patients and 03 (13.63%) patients had a history of fall. Right-sided fractures were observed in 15 (68.18%) patients and the remaining were of left sided. Thirteen (59.10%) patients had Type 1 open femur shaft fractures and nine (40.90%) patients had Type 2 fractures [Table 1]. Fracture union was observed in six patients (27.27%) at 3 months and in 16 (72.72%) at 3–6 months.

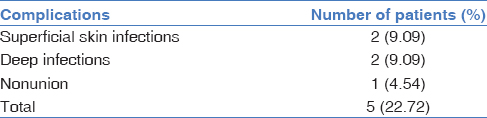
Complications observed were superficial wound infections in two patients, deep infections in two patients, and nonunion in one patient [Table 2]. Superficial infections were managed with dressing and antibiotics. One patient with deep infection was managed with thorough debridement and use of antibiotic beads and the other patient with deep infection was managed with debridement and implant removal. The nonunion patient was managed with bone grafting.
The relation between age of the patient, mode of trauma, and grade of compound fractures with the functional outcome was not statistically significant (P > 0.05). The difference between the grade of fractures and the risk of deep infection was significant. We observed deep infection(2 patients) only in grade 2 fractures not in grade 1 fractures.
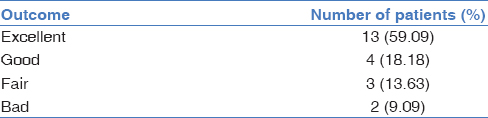
In our study, 13 (59.09%) patients got excellent outcome, 4 (18.18%) patients got good outcome, 3 (13.63%) patients got fair outcome, and 2 (09.09%) patients got poor outcome as per the Harris Hip Score and Oxford Knee Score [Table 3]. The functional outcome was calculated by combining both the scores, and the difference was not statistically significant (P > 0.05) [Figure 1-3].

- (a) Case 1 – preoperative X-ray. (b) Case 1 – clinical wound picture. (c) Case 1 – postoperative X-ray

- (a) Case 2 – preoperative X-ray. (b) Case 2 – clinical wound picture. (c) Case 2 – postoperative X-ray
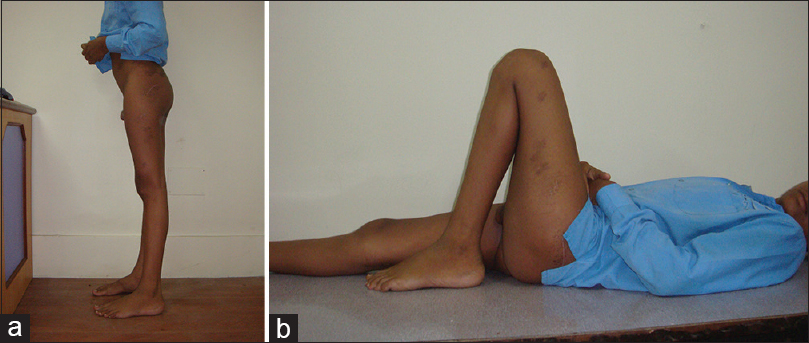
- (a) Functional outcome: knee extension. (b) Functional outcome: knee flexion
Discussion
Conventionally, according to Chapman,[4] intramedullary nailing for open femoral fractures was delayed until 1 week till the closure or coverage of the open fracture wound. However, delayed surgical stabilization and management of open femoral fractures associated with severe soft-tissue injury was problematic. In polytrauma patients, immediate or early stabilization of femur shaft fractures is important for the prevention of pulmonary complications.[5]
In our study, we observed more number of male patients compared to females, which is similar to the study conducted by Mohammad et al.[6] because males are more involved in outdoor activities. The common mode of injury was road traffic accidents and young patients (64%) were involved more as compared to older individuals, which is similar to the study by Ferracini et al.[7] because more young individuals are involved in rash driving with alcohol consumption. Complications observed were (22.72%) superficial and deep infections, nonunion. The infection rate observed was similar to the study by O'Brien et al.[8]
The infection and nonunion rates had decreased compared to previous studies by Yokoyama et al.,[9] most probably because of improved surgical techniques, debridement techniques, and postoperative management.
We had two patients with deep infections, which were Grade 2 fractures. The risk of infection increases as the grade of compound fractures increases (according to Gustilo–Anderson classification). Similar result was observed in the study by Noumi et al.[10] It is always essential to give thorough wound wash and better debridement at the first time during the fixation to avoid infection risk.
We had one patient with nonunion, which was Grade 2 femur fracture. The risk of nonunion increases as the grade of soft-tissue injury increases as suggested by Noumi et al.[10] Soft-tissue injury at the time of trauma and the debridement procedures cause the loss of fracture hematoma, which may lead to the nonunion and distraction at the fracture site during the fixation also leads to the nonunion.
Brumback et al.[11] advised that if a thorough and timely debridement can be accomplished, immediate intramedullary nailing of Grade 1 and Grade 2 open fractures of the femoral shaft does not increase the risk of postoperative infection.
The functional outcome (78% excellent-to-good outcome) observed in our study was comparable to that of the study by Grosse et al.[12] Good debridement of the wound, stable fracture fixation, and early mobilization of the patients help to get good functional outcome. Studies by Thoresen et al.[13] and Basha et al.[14] showed 63% and 60% of excellent outcome, respectively; they considered malalignment, shortening of femur, knee range of motion, and pain for the assessment of functional outcome.
Conclusion
Primary intramedullary nailing is an effective method of managing Type 1 and 2 open femur shaft fractures if thorough early and timely debridement can be done. It is associated with less complications, helps in early mobilisation and also avoids secondary procedures.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Femur shaft fractures. In: Court-Brown Charles M, Heckman James D, eds. Rockwood and Greens Fractures in Adults. Philadelphia: Wolters Kluwer; 2015. p. :2149.
- [Google Scholar]
- Further progress in the area of medullary nailing. Langenbecks Arch Chir. 1996;316:224-231.
- [CrossRef] [PubMed] [Google Scholar]
- Early versus delayed stabilization of femoral fractures. A prospective. J Bone Joint Surg Am.. 1989;71:336-40.
- [CrossRef] [PubMed] [Google Scholar]
- The role of intramedullary fixation in open fractures. Clinical orthopaedics and related research.. 1986;212:26-34.
- [CrossRef] [Google Scholar]
- Early osteosynthesis and prophylactic mechanical ventilation in the multitrauma patient. J Trauma. 1982;22:895-903.
- [CrossRef] [PubMed] [Google Scholar]
- Interlocking intramedullary nailing in comminuted femoral shaft fractures. J Nobel Med Coll. 2011;1:57-63.
- [CrossRef] [Google Scholar]
- Prospective and randomized study of patients with open fractures of the femoral shaft, treated with plate or open intramedullary locked nail. ActaOrtop Bras.. 2008;16:102-6.
- [CrossRef] [Google Scholar]
- Primary intramedullary nailing of open femoral shaft fractures. J Trauma. 1991;31:113-6.
- [CrossRef] [PubMed] [Google Scholar]
- Deep infection and fracture healing in immediate and delayed locked intramedullary nailing for open femoral fractures. Orthopedics. 1999;22:485-90.
- [Google Scholar]
- Intramedullary nailing for open fractures of the femoral shaft: Evaluation of contributing factors on deep infection and nonunion using multivariate analysis. Injury. 2005;36:1085-93.
- [CrossRef] [PubMed] [Google Scholar]
- Intramedullary nailing of open fractures of the femoral shaft. J Bone Joint Surg Am. 1989;71:1324-31.
- [CrossRef] [Google Scholar]
- Open adult femoral shaft fracture treated by early intramedullary nailing. J Bone Joint Surg Br. 1993;75:562-5.
- [CrossRef] [PubMed] [Google Scholar]
- Interlocking intramedullary nailing in femoral shaft fractures. A report of forty-eight cases. J Bone Joint Surg Am. 1985;67:1313-20.
- [CrossRef] [Google Scholar]
- A clinical study of surgical management of fracture shaft femur in adults with intramedullary interlocking nail. J. Evid. Based Med. Healthc.. 2017;4:3541-4. DOI: 10.18410/jebmh/2017/706
- [CrossRef] [Google Scholar]




