
Translate this page into:
Preoperative Knee Self-Efficacy Scale as a predictor of outcome following anterior cruciate ligament reconstruction: A short-term study
Address for correspondence: Dr. Ravi Kumar, Department of Orthopaedics, AIIMS, Patna - 801 507, Bihar, India. E-mail: k2.drravi@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Kumar S, Kumar A, Kumar R. Preoperative Knee Self-Efficacy Scale as a predictor of outcome following anterior cruciate ligament reconstruction: A short-term study. J Orthop Spine 2021;9:39-42.
Abstract
BACKGROUND:
The purpose of this study was to validate the possibility for preoperative self-efficacy of knee function measured by the Knee Self-Efficacy Scale (K-SES) to foresee patient outcome in terms of patient-reported outcome (PRO) scores at 2 years after an anterior cruciate ligament (ACL) reconstruction (ACLR).
MATERIALS AND METHODS:
This was a prospective study of cohort of 90 patients who underwent primary ACLR using hamstring tendon graft by a single team of surgeons over a period of 2 years at a government teaching tertiary care hospital. Demographic data (age and sex) and self-efficacy of knee function using K-SES were measured before surgery. Functional outcome were assessed using Tegner Lysholm Knee (TLK) Scoring Scale, Knee Injury and Osteoarthritis Outcome Score (KOOS), and International Knee Documentation Committee (IKDC) score at every scheduled follow-up after surgery. The mean of K-SES, TLK, IKDC, and KOOS scores was calculated. Pearson correlation coefficient was calculated to find out the relation between K-SES and the three knee subjective scores independently. Two-tailed test was used to compute the statistical significance of parameter deduced from data set.
RESULTS:
There was a strong positive correlation between K-SES and the three subjective scores independently. Two-tailed tests were statistically significant for all the three correlations.
CONCLUSION:
Evaluation of knee function using K-SES preoperatively is of predictive value for good functional outcome at 2 years after ACLR.
Keywords
Anterior cruciate ligament
International Knee Documentation Committee score
Knee Injury and Osteoarthritis Outcome Score
Knee Self-Efficacy Scale
Tegner Lysholm Knee Scoring Scale

Introduction
Anterior cruciate ligament reconstruction (ACLR) is one of the most commonly performed arthroscopic surgeries in orthopedics,[1] and anterior cruciate ligament (ACL) injuries are one of the most researched topics in orthopedic publications with annual incidence of ACL tears as 68.6/100,000 person-years following adjustment to age and gender.[2] These injuries are often seen in young active individuals who aspire to return to their demanding work as early as possible. The past decade has seen enormous work in ACL surgical techniques and rehabilitation protocols which subsequently resulted in improved patient outcomes; however, ACL surgery still requires vigorous and extensive rehabilitation efforts from patients.[3]
Recently, a Multicenter Orthopaedic Outcomes Network cohort in 2012 reported that out of 63%–69% of athletes who returned to play football at high school or college level following ACLR; just 43% of them reported returning to similar performance level.[4] Fifty percent of the nonreturners in this study specified fear of re-injury as a reason, and the authors advocated an undervalued role of psychological factors in getting athletes back to the playing fields.[4] The psychological factors, especially the one which is correlated to how the patients think of their knee function, have a significant impact on postoperative outcome.[5] For instance, an athlete who fears re-injuring his or her knee and lacks confidence in the function of the reconstructed knee shall eventually fall short of accomplishing their goals and culminates into dissatisfaction.[6] The concept of self-efficacy was first given by Bandura,[7] and later, Crossman[8] propounded the significance of self-efficacy in assessing rehabilitation outcome following sports injuries. Thomee et al.[9] defined self-efficacy as a perception of one's aptness to carry out a task, rather than an assessment of whether one can or does execute the task.[9] The significance of self-efficacy beliefs for patients with an ACL injury was discussed by Evans and Hardy, but they did not have any specific instrument.[10] It was only in 2006 that Knee Self-Efficacy Scale (K-SES) as an instrument for measuring self-efficacy in patients with an ACL injury was recommended.[9] Literature is concordant in assuming unequivocal role of psychological factors in recovery following ACLR, but it has limited studies mentioning correlation between preoperative psychological assessment and postoperative functional outcome.
The purpose of this study was to find out the effect of preoperative K-SES as a predictor of functional outcome following ACLR. Our hypothesis is that clinical outcome following ACLR can be predicted by how patients perceive their knee self-efficacy preoperatively.
Materials and Methods
This was a prospective study with sample size of 90 patients who underwent primary ACLR between January 2016 and April 2018 at a government teaching tertiary care hospital. The study had prior approval from IRB. The data collected during outpatient visit during preoperative evaluation included age, sex, side of injury, comorbidities if any, and self-efficacy of knee function using K-SES. The K-SES consists of 22 items in four sections and is a self-administered instrument. The total scores were calculated and then divided by the number of items.[9]
Our study had included all skeletally mature patients with ACL tear and minimum 2-year follow-up. We excluded patients with bilateral ACL tear, meniscal injury, associated ligament injury like medial collateral ligament, lateral collateral ligament, posterior cruciate ligament or injury involving posterolateral corner, previous history of ACL repair, or reconstruction. The sports unit of the department performed all the surgeries. Arthroscopic ACLR was performed using quadruple-looped hamstring autograft. We had used the surgical technique as described by S. Kumar et al.[11] for accurate positioning of femoral and tibial tunnel using the indigenously made grid on a transparency sheet and C-arm. Adjustable loop endobutton was used to fix the graft tendon to femur and bioabsorbable screw as suitable to the tunnel diameter was used to fix graft tendon to the tibia. All patients followed similar standard hospital ACL rehabilitation protocol. The patients were followed up postoperatively at 3, 6, 12, and 24 months, respectively. Patients were evaluated objectively with Lachman test, measurement of range of motion. Subjective data collected included Tegner Lysholm Knee (TLK) Scoring Scale, Knee Injury and Osteoarthritis Outcome Score (KOOS), and International Knee Documentation Committee (IKDC) score.
Statistical analysis was done using the Statistical package for the social sciences (SPSS) version 21.0 IBM manufacturers, Chicago, USA. The mean of age, K-SES, TLK, IKDC, and KOOS scores were calculated. Pearson correlation coefficient was measured to find out the relation between K-SES and the three individual scores independently. Two-tailed test was used to assess the statistical significance of parameter deduced from the statistics.
Results
The sample size was 90 patients. There were 85 male (94.44%) and 5 female (5.56%) with age ranging from 17 years to 50 years. The mean age was 28 years. The minimum follow-up was of 2 years. The K-SES score ranged from 2.00 to 5.86 with a mean of 4.01. The three postoperative scores at the end of 2 years were taken into consideration. TLK Scoring Scale is graded as: <65 – poor, 65–83 – fair, 84–90 – good, and >90 – excellent. The mean of TLK score was 89.54 which was good. KOOS score interpretation is 0–100 (100 as excellent) while IKDC score interpretation is 0–100 (100 as excellent). The mean of IKDC score was 66.57, while for KOOS score, the mean was 84.89.
Pearson correlation (r value) revealed a positive linear correlation between K-SES and TLK score [Figure 1], K-SES and IKDC score [Figure 2], and K-SES and KOOS score [Figure 3], respectively, thereby implying that with the increase in K-SES score, all the three subjective scores increase significantly – P < 0.001 for TLK, IKDC, and KOOS scores.
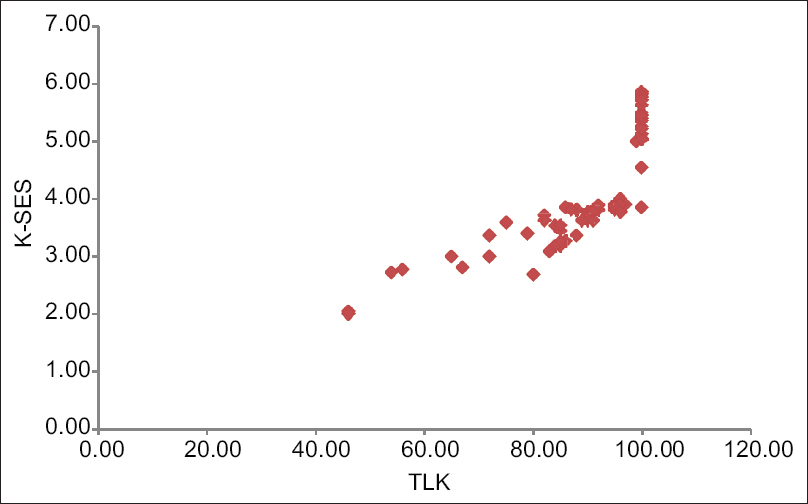
- Scattered plot depicting linear correlation between Knee Self-Efficacy Scale and Tegner Lysholm Knee score
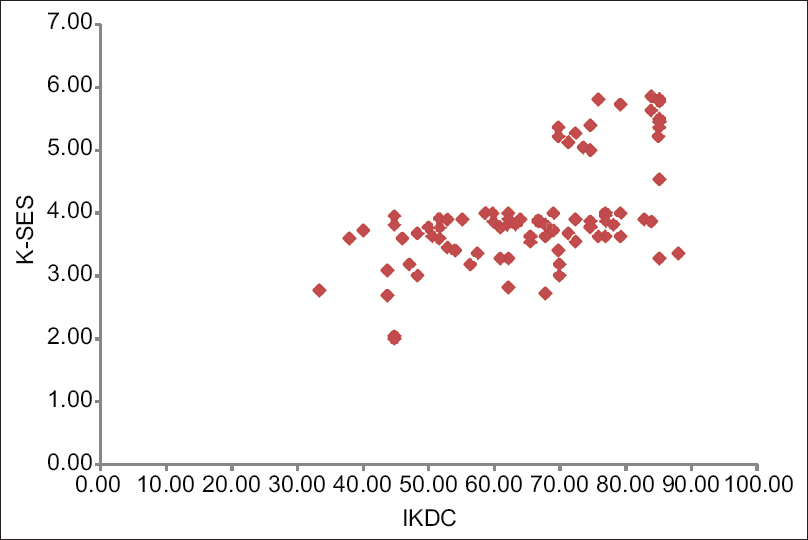
- Scattered plot depicting linear correlation between Knee Self-Efficacy Scale and International Knee Documentation Committee
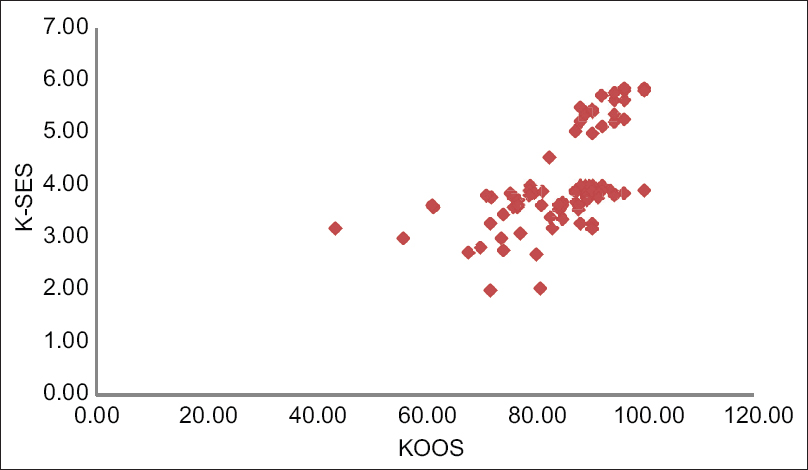
- Scattered plot depicting linear correlation between Knee Self-Efficacy Scale and Knee Injury and Osteoarthritis Outcome score
Discussion
The application of PRO measures to evaluate outcome following an intervention has become very common in medical practice and this has given the patients a voice in their health management. There are numerous factors that have been linked to affect the adherence to rehabilitation such as self-motivation, efficacy, self-efficacy, emotional adjustment, and social support for rehabilitation.[12,13,14,15] The K-SES has demonstrated good reliability and validity for outcomes but has not been specifically validated for return to sport after ACLR.[16] The last two decades has seen tremendous research in exploring the role of psychological factors in rehabilitation following sports injuries.
Our findings are in line with the study done by Thomee et al.[17] who had assumed that one of the prognosticative value for an athlete's return to acceptable levels of physical activity, symptoms and muscle function at 1 year after ACLR is there preoperative perceived self-efficacy of knee function. There are numerous studies to support the notion that strengthening the patient's self-efficacy of performance for physical work during rehabilitation shall reduce the consequences of that specific illness.[18,19,20]
Another study reported by Christino et al.[21] concluded that self-esteem levels and locus of control had significant relationships with functional test performance and validated outcome measures after ACLR and found that sport returners had significantly higher self-esteem levels than those who did not return to sports, without observable differences in knee stability or time since surgery.
Further, in 2006, a study of 100 ACLR patients found that those who returned to sports had higher psychovitality and subjective outcome scores when compared to those who could not return to sports.[22] This has been supported recently by a review of Medline database which concluded that psychological factors play an important role in return to play after ACLR.[16]
As an orthopedic surgeon, it is a formidable task for us to identify the patients who are at risk for a poor surgical outcome which if done appropriately would allow us to refer to a sports psychologist. It is imperative to have a multidisciplinary approach for ACLR.
There are few constraints of this study which needs to be brought up, i.e., extreme male predominance (94.4%) in gender distribution and small sample size.
Conclusion
Evaluation of knee function using K-SES preoperatively is of predictive value for good functional outcome at 2 years after ACLR. We feel that a multidisciplinary approach is need of the hour so to have a greater patient satisfaction and improved functional outcomes.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- The science of reconstruction of the anterior cruciate ligament. J Bone Joint Surg Am. 1997;79:1556-76.
- [CrossRef] [PubMed] [Google Scholar]
- Incidence of anterior cruciate ligament tears and reconstruction: A 21-year population-based study. Am J Sports Med. 2016;44:1502-7.
- [CrossRef] [PubMed] [Google Scholar]
- Psychological factors, rehabilitation, adherence, and rehabilitation outcome after anterior cruciate ligament reconstruction. Rehabil Psychol. 2000;45:20-37.
- [CrossRef] [Google Scholar]
- Return to high school and college level football following ACL reconstruction: A MOON Cohort Study. Am J Sports Med. 2012;40:2523-9.
- [CrossRef] [PubMed] [Google Scholar]
- Patient participation during anterior cruciate ligament reconstruction improves comprehension, satisfaction, and functional outcomes: A simple way to improve our practices. Orthop J Sports Med. 2019;7:2325967119841089.
- [CrossRef] [PubMed] [Google Scholar]
- Psychological responses matter in returning to preinjury level of sport after anterior cruciate ligament reconstruction surgery. Am J Sports Med. 2013;41:1549-58.
- [CrossRef] [PubMed] [Google Scholar]
- Self-efficacy: Toward a unifying theory of behavioral change. Psychol Rev. 1977;84:191-215.
- [CrossRef] [PubMed] [Google Scholar]
- Coping with Sports Injuries: Psychological Strategies for Rehabilitation. New York: Oxford University Press.
- [CrossRef] [Google Scholar]
- A new instrument for measuring self-efficacy in patients with an anterior cruciate ligament injury. Scand J Med Sci Sports. 2006;16:181-7.
- [CrossRef] [PubMed] [Google Scholar]
- Injury rehabilitation: A goal-setting intervention study. Res Q Exerc Sport. 2002;73:310-9.
- [CrossRef] [PubMed] [Google Scholar]
- Accurate positioning of femoral and tibial tunnels in single bundle anterior cruciate ligament reconstruction using the indigenously made Bernard and Hurtle grid on a transparency sheet and c-arm. Arthrosc Tech. 2017;6:e757-61.
- [CrossRef] [PubMed] [Google Scholar]
- Adherence to sport injury rehabilitation programs. J Appl Sport Psycho. 1998;10:70-82.
- [CrossRef] [Google Scholar]
- Threat and coping appraisal as determinants of compliance to sports injury rehabilitation: An application of protection motivation theory. J Sports Sci. 1996;14:471-82.
- [CrossRef] [PubMed] [Google Scholar]
- Cognitive appraisal, emotional adjustment, and adherence to rehabilitation following knee surgery. J. Sport Rehabil. 1995;4:23-30.
- [CrossRef] [Google Scholar]
- The provision of social support to injured athletes: A qualitative analysis. J Sport Rehabil. 1998;7:267-84.
- [CrossRef] [Google Scholar]
- How much do psychological factors affect lack of return to play after anterior cruciate ligament reconstruction? A systematic review. Orthop J Sports Med. 2019;7:2325967119845313.
- [CrossRef] [PubMed] [Google Scholar]
- Self-efficacy of knee function as a pre-operative predictor of outcome 1 year after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2008;16:118-27.
- [CrossRef] [PubMed] [Google Scholar]
- Role of self-efficacy in rehabilitation outcome among chronic low back pain patients. J Couns Psychol. 1993;40:335-9.
- [CrossRef] [Google Scholar]
- Development and evaluation of a scale to measure perceived self-efficacy in people with arthritis. Arthritis Rheum. 1989;32:37-44.
- [CrossRef] [PubMed] [Google Scholar]
- Determinants of self-report outcome measures in people with knee osteoarthritis. Arch Phys Med Rehabil. 2006;87:96-104.
- [CrossRef] [PubMed] [Google Scholar]
- Psychological factors associated with anterior cruciate ligament reconstruction recovery. Orthop J Sports Med. 2016;4:2325967116638341.
- [CrossRef] [PubMed] [Google Scholar]
- Factors affecting return to sports after anterior cruciate ligament reconstruction with patellar tendon and hamstring graft: A prospective clinical investigation. Knee Surg Sports Traumatol Arthrosc. 2006;14:1021-8.
- [CrossRef] [PubMed] [Google Scholar]




