
Translate this page into:
Percutaneous transforaminal endoscopic discectomy and drainage for spondylodiscitis: A technical note and review of literature
Address for correspondence: Dr. Ajay Krishnan, C302, Orange Avenue, Maple County 1, Thaltej, Ahmedabad - 380 059, Gujarat, India. E-mail: drajaykrishnan@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Krishnan A, Barot MP, Dave BR, Bang P, Devanand D, Patel D, Jain A. Percutaneous transforaminal endoscopic discectomy and drainage for spondylodiscitis: A technical note and review of literature. J Orthop Allied Sci 2018;6:S16-20.
Abstract
Spondylodiscitis is on rise due to increasing elderly population and immunocompromised people and now gets early detected due to early imaging. Percutaneous Transforaminal Endoscopic Discectomy and Drainage (PTELDD), is simple procedure that yields high culture wihich helps in specific targeted antimicrobial bombardment. Dr. Satishchandra Gore has been pioneer in introducing transforaminal endoscopy in India way back in 1999. His persistent efforts has made inroads into traditional spine care treatments and endoscopy bandwagon is flying high and many surgeons are able to give results with the technique all over India. The available english literature of transforaminal endoscopy in spondylodiscitis is reviewed here with technical note of this simplistic procedure. The reported outcome in literature is excellent in majority of cases. Authors unpublished report of 16 cases is also comparable with literature. PTELDD is a simplistic most minimalist minimally invasive procedure that gives very positive outcome in early cases of spondylodiscitis.
Keywords
Discitis
endoscopy
percutaneous
percutaneous transforaminal endoscopic discectomy and drainage
spondylodiscitis
transforaminal

Introduction
Spondylodiscitis is an infection of the intervertebral disc and adjoining vertebra, and there can be variable predominance of one over other.[1-3] Spondylodiscitis can be primary or secondary. Primary infection is occurring directly and only in the spine. Secondary is a spread from infective foci elsewhere in the body. Infection to the spine can occur through hematogenous spread or spread from contagious adnexa or by direct inoculation by any intervention (needle or surgery).[1,2] The incidence is on rise due to increasing elderly population and immunocompromised people.[1,3-5] Postoperative discectomy patients developing discitis is also not very uncommon with incidence of 0.21%–3.6% reported.[6] Spondylodiscitis can also be categorized on the basis of the organism causing the discitis as pyogenic, granulomatous, or fungal.[1,3] Most common site of discitis is lumbar or thoracolumbar region.[1] The early diagnosis depends on a combination of clinical, laboratory, and imaging findings.[1-3]
Clinical Features
Clinical features in spondylodiscitis are pain and disability. The onset is acute in pyogenic and chronic in granulomatous infection. Fever and constitutional features of septicemia may be present in pyogenic spondylodiscitis. The pain and disability is usually progressive. Night pain is common feature in chronic granulomatous spondylodiscitis. The presenting feature may include deformity and neurological deficits also.[1,2,7] The diagnosis is strongly suggested by a persistently elevated erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) values, and by typical changes on magnetic resonance imaging (MRI). Findings on a plain radiograph may not be reliable. The radiographic finding which may first appear is loss of intervertebral height accompanied with erosion of end plates. MRI with gadolinium scan is more sensitive. It is the radiographic imaging modality of choice in diagnosing POS.[7,8]
The goals of treatment are to make a prompt diagnosis, isolate the organism, and start antibiotic treatment. This is to be combined with variable rest and bracing. Conservative approach works in most of the cases detected early. Surgery is reserved for those who fail to respond and develops instability or neurological deficits or serious epidural abscess.[1-3,5,9]
Specimen samples are to be obtained by transpedicular vertebral body biopsy or transforaminal discal or paraspinal aspiration biopsy and culture; blood culture can give positivity in many patients. The sample is to be sent for culture sensitivity in proper bottles for bacterial, granulomatous, and fungal culture. GeneXpert and tuberculosis (TB) polymerase chain reaction is other advanced investigation to be combined in our country where TB is very common.[1,3] Normalization or decreasing trend of the ESR and CRP values is an important parameter to monitor for healing response.[1-3,9,24] The leading cause in most of the cases is Staphylococcus aureus(60%). Gram-negative organisms are also common, but in recent years, immunocompromised states and the use of broad-spectrum antibiotics have led to an increase in the infection rate with unusual organisms including fungi and mycobacterium species.[3]
Percutaneous transforaminal endoscopic lumbar discectomy and drainage (PTELDD) is a promising technique and is fast emerging for its simplicity, accuracy of diagnosis, and therapeutic advantage of debridement.[4,5,11-24]
Indications and Contraindications
Any spondylodiscitis without advanced vertebral destruction or instability or without serious neurological deficit or multilevel affection can be considered for PTELDD. Typical lumbar spondylodiscitis presenting early and postoperative open/endoscopic discectomy discitis are classic indications. Elderly patients or patients with serious medical condition who have advanced spondylodiscitis where open definitive surgery cannot be feasible can be considered as logical and absolute indication as well.[4,25]
Anatomical Considerations
Any level from L5–S1 to D12–L1 can be approached by the transforaminal percutaneous endoscopic lumbar discectomy (PELD) approach through the Kambin's Triangle which is a well-established method for discectomy and evolving for stenosis decompression.[26] The technique variation of entry and obliquity of approach to reach the epidural space is not needed for spondylodiscitis. The target of the procedure is center of the disc and can be achieved with a trajectory of 45°–55° from a 6–8 cm entry point. Though drainage of dural abscess or granulation will need more shallow access.
Technique
It is done under local anesthesia though general anesthesia is also practiced at many centers in world. It has to be understood that these patients have more severe pain than a standard percutaneous discectomy patients. So, more cooperation is expected from the patient and more counselling is to be done. Prone position is well tolerated but lateral position can be considered. Another important consideration is to be made that local aneasthesia may not be as effective around infective tissue which necessitates larger amount of drug given locally. Markings are done in anteroposterior and lateral image intensifier view to obtain a centralized vertebra with equidistant pedicles from a centered spinous process. The orthogonal view is obtained paralleling the disc space. Good image intensifier and efficient technician is mandatory as patients may not be able to give good position because of pain, vertebral destruction or collapse may obscure standard endplate visibility. Preferably, no antibiotics are given 72 h preoperative to increase the chances of positive culture. Markings are done as per standard protocols of PTELDD, and under local anesthesia, sequential and railroading is done: needle, guided wire, dilator–trocar, working cannula, and irrigating endoscope with attachment. Aspiration of the disc with needle positioning and taking first biopsy bites of disc with endoscope without starting irrigating fluid is necessary. To get concentrated sample disc, forceps biopsy through the working cannula without endoscope can retrieve more tissue. But beware, the most important dangerous technical error can occur. Because of friability of annulus, any instrument can violate the confines of intervertebral disc space and lead to catastrophic iatrogenic injuries. Hence, hand-mind feedback has to be softer and perfect in PTELDD. Image intensifier is to be used frequently with small change or advancements of instruments also. After obtaining sample, piecemeal discectomy of friable tissue is to be completed slowly and a saline irrigation of 3–4 l is to be finished. Larger fragments may be removed; loose endplate cartilage and at times small sequestra of bones may also be removed. Bleeding from exposed bone is an added concern in PTELDD which can be countered by saline. Pressure manually or with pump intermittently after the completion of the procedure, a drain is put in the disc space and stay sutures are taken. Negative suction drain is to be kept till the drain amount reduces to negligible below 5 ml for 2–3 days. A patient is given injectable antibiotic according to sensitivity and the switched to oral antibiotic. The total antibiotic duration including injectable and oral schedules is 8 weeks. Antituberculosis treatment as per institutional protocol and the WHO guidelines is completed in tuberculous spondylodiscitis which is for a period of 12 months. As per symptoms and tolerance of patients, they are mobilized with lumbosacral corset/belt for basic personal activities.
Complications
All complications related to PELD approach can occur with PTELDD, namely dural tear, root injury, dysesthesia, visceral injury, discitis, instrument breakage, failure of treatment, etc. Through the literature reports variable complication rate of PTELD, it is less reported for PTELDD in spondylodiscitis. The complication of anesthesia, blood loss, iatrogenic injuries, and other morbidities is not uncommon with open instrumented or noninstrumented surgeries for spondylodiscitis. However, for PTELDD, it is very less reported in literature.
Review of Literature
Now, it is the world literature and evidence-based medicine that mandates and advocated biopsy of the infective spine before starting antibiotic.[1,27,28] First biopsy of the spine was reported in 1934 by Ball.[2,29] Transforaminal aspiration of the disc or from pedicular biopsy has been reported in literature.[1] Since Adapon first described computed tomography (CT)-guided percutaneous needle biopsy, spine biopsy using CT guidance has been widely used as cost-effective procedure.[27,29,30] Percutaneous discectomy to diagnose and treat spondylodiscitis was reported in the 1990s.[11,13,14] Now, PTELDD has abundant literature support for its higher biopsy success rate (86%–100%). Reduction of pain and final healing success ratio varies from 83% to 100%.[4,6,10-24] The biopsy success rate and culture bacterial recovery are higher than the CT-guided biopsy also.[16] The comparative results of PTELDD and anterior debridement fusion also advocate PTELDD to be considered the first choice.[23] Especially for patients of serious comorbidities and immunocompromised and complicated spondylodiscitis, it is the treatment of choice.[4,5]
In postoperative spondylodiscitis promising after open/minimally invasive spinal surgery/endoscopic discectomy as well, PTELDD holds true that early intervention before structural damage gives excellent outcome approaching 100%.[18,20,21] Percutaneous endoscopic debridement by direct different 4 approaches has also been reported with excellent outcome in 14 patients, 2 repeat procedures, and 1 failure in a group of 17 elderly patients with comorbidities.[31] Even adnexal abscess, especially psoas abscess, can be drained.[31,32] CT-guided safe placement of angiography catheter followed by the same day or next day percutaneous endoscopic debridement for even dorsal spondylodiscitis has been efficiently and effectively described with good outcomes.[5] PTELDD biportal approach has also been reported in literature.[22]
Author's Experience
The unpublished data of short-term outcome in 16 cases of spondylodiscitis is excellent. Out of these, five cases are postoperative spondylodiscitis, seven are early primary spondylodiscitis, two are complicated spondylodiscitis in serious comorbid chronic renal failure patients, and two are in destructive spondylodiscitis without gross mechanical instability [Figure 1a-g]. Of the 16 patients, one patient of postoperative spondylodiscitis and one patient of primary spondylodiscitis did not respond to PTELDD. Both of these patients had symptom duration of 2 and 2.5 months each and failed to respond and needed fusion. In postoperative spondylodiscitis, all patients had symptom duration of >5 weeks. Though the 2 cases of destructive spondylodiscitis had symptom duration of 3 and 4 months, respectively, they responded excellently [Figures 2 and 3]. There has an element of bias because at our institute, we do aggressively fusion for all patients with mechanical instability and late presentation. Again, in unpublished data, we have noticed a low threshold for fusion at our center for postoperative spondylodiscitis (n = 44 from October 2003 to October 2017) presenting from elsewhere primarily, operated because long time of 8–12 weeks had elapsed before they present to us. Probably, these cases could be considered for PTELDD before mechanical symptoms develop, i.e., if they present early within 4 weeks. However, these patients have protracted treatment time since the first onset of symptoms, lost belief in spine surgery in them, and even depression in many patients. If these patients are put through PTELDD and then consider fusion in non responsive cases, then more time will be spent till outcome becomes apparent. More uncertain time and the indirect cost of getting back to productive active life may add to the burden of poor depressed patients. In personal communication with most of the endoscopic surgeons, unbelievably, it is noted that PTELDD gives immediate pain relief in early operated cases.
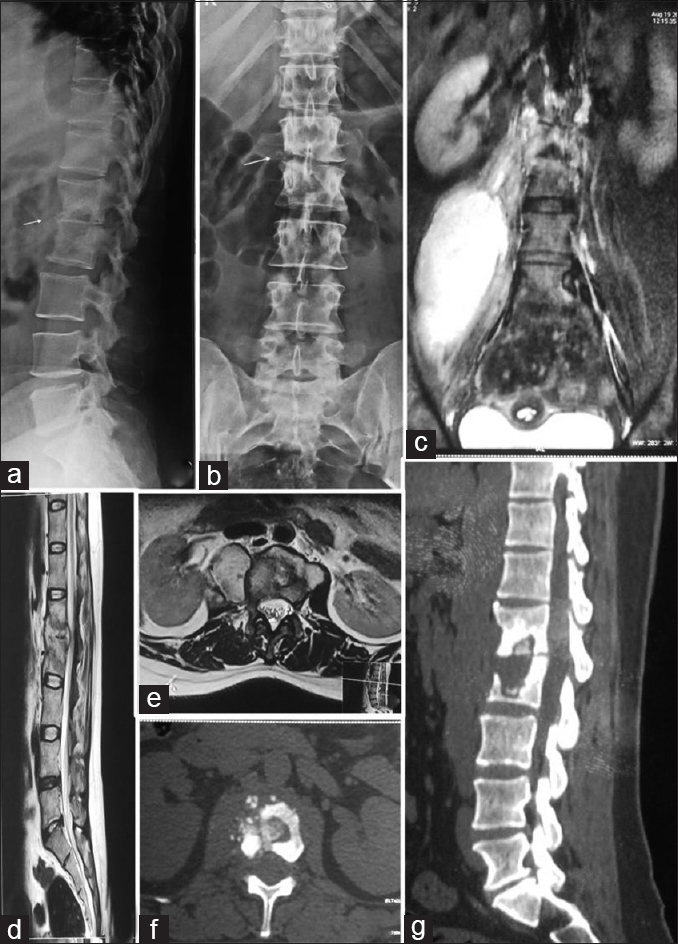
- (a and b)Radiograph showing cavitating peridiscal lesion, (c) Coronal T2 STIR magnetic resonance imaging showing spondylodiscitis L1-2 with large psoas abscess, (d and e) T2 sagittal and axial magnetic resonance imaging showing abscess and granulating lesion in epidural and paravertebral region. (f and g) Computed tomography axial and sagittal showing destructive lesion with sequestrums
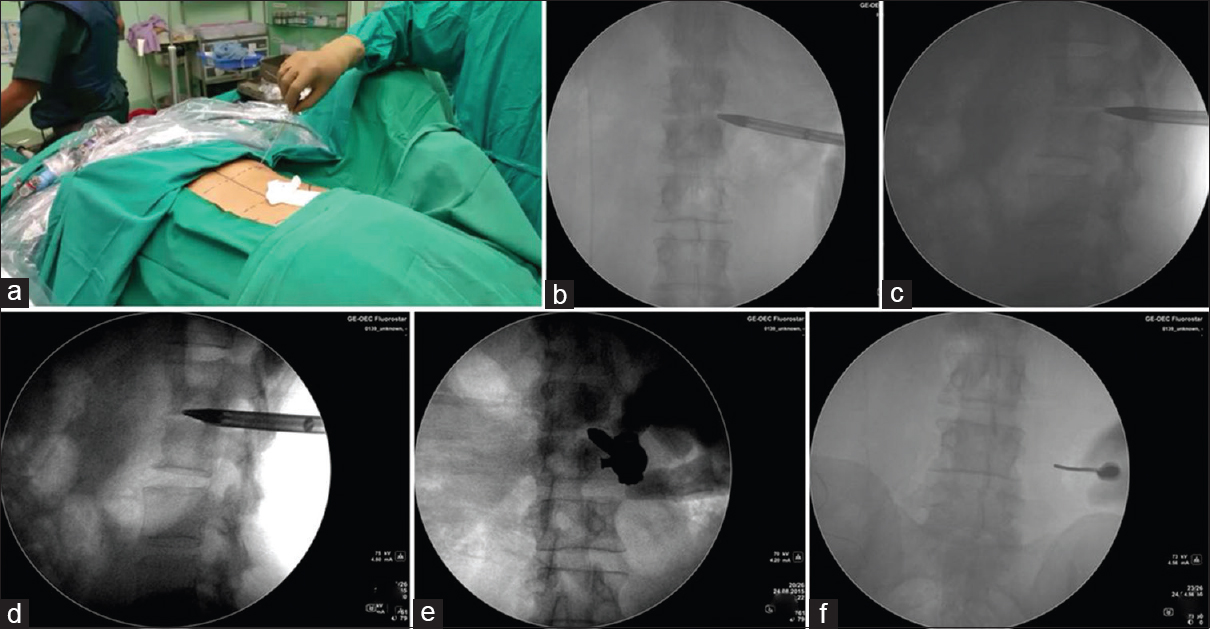
- (a)Classic entry at 7 cm, 45°. (b and c) C-arm image showing trocar reached posterolateral corner, (d and e) Trocar followed by working sheath in center of disc, (f) Needle put paravertebral to guide the endoscope into psoas abscess
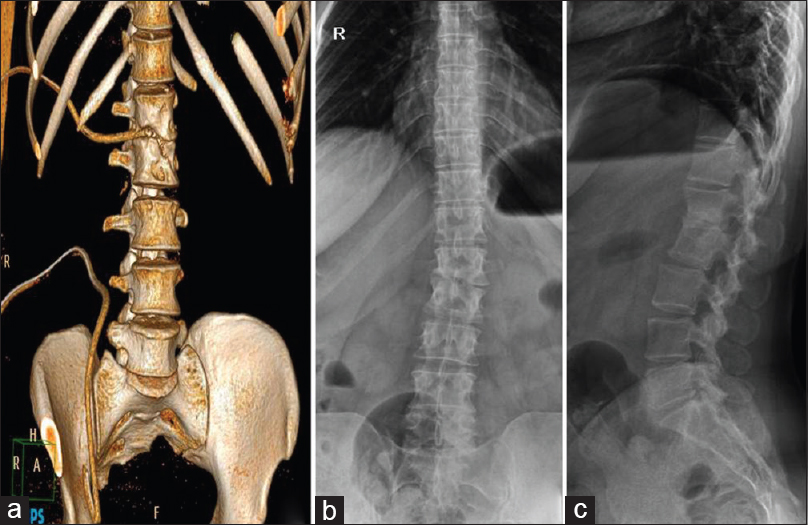
- (a) Computed tomography image postoperative showing the position of two drain tubes in intervertebral disc and psoas abscess, respectively. The patient ambulated the same day, (b and c) radiographs at 3-year follow-up showinghealed lesion
Conclusion
Looking to the excellent biopsy yield and literature, minimalist minimally invasive PTELDD should be considered in all cases of spondylodiscitis as the first-stage treatment, especially before setting in of structural derangement and instability. Other cases of long-standing symptoms and instability comparative studies are needed with consideration of outcome, cost, and resumption of work as the main parameters to establish protocols.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Spinal Infections & Trauma (1st). ASSI (Jaypee); 2011.
- Spondylodiskitis. A retrospecitve study of 163 patients. Acta Orthop. 2008;79:650-9.
- [CrossRef] [PubMed] [Google Scholar]
- Sponylodiscitis: update on diagnosis and management. J Antimicrob Chemother. 2010;65(3):11-24.
- [Google Scholar]
- Percutaneous endoscopic debridement and drainage in immunocompromised patients with complicated infectious spondylitis. Minim Invasive Ther Allied Technol. 2010;19:42-7.
- [CrossRef] [PubMed] [Google Scholar]
- A Minimally Invasive Endoscopic Surgery for Infectious Spondylodiskitis of the Thoracic and Upper Lumbar Spine in Immunocompromised Patients. Biomed Res Int. 2015;2015:780451..
- [CrossRef] [PubMed] [Google Scholar]
- Postoperative spondilodiscitis. International Orthopaedics (SICOT). 2012;36:433-38.
- [CrossRef] [PubMed] [Google Scholar]
- Spondylodiscitis. Clinical and magnetic resonance diagnosis. Spine (Phila Pa 1976). 1997;22:1741-6.
- [CrossRef] [PubMed] [Google Scholar]
- The role of magnetic resonance imaging (MRI) in the diagnosis of spondylodiscitis. Neurosurgical review. 1990;13:279-83.
- [CrossRef] [PubMed] [Google Scholar]
- Microsurgical management of postoperative disc space infection. Neurosurg Rev. 2003;26:102-7.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of osteomyelitis of the spine using percutaneous suction/irrigation and percutaneous external spine fixation. J Spinal Disord. 1994;7:185-205.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous diskectomy for the treatment of bacterial diskitis. Spine (Phila pa 1976). 1994;19:855-7.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous diskectomy for disk space infections. J South Orthop Assoc. 1994;3:283-9.
- [Google Scholar]
- Percutaneous lumbar diskectomy in the treatment of lumbar diskitis. Eur Spine J. 1997;6:98-101.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous transpedicular diskectomy and drainage in Pyogenic spondylodiskitis. Am J Orthop (Belle Mead NJ). 1998;27:188-97.
- [Google Scholar]
- Clinical outcome of posterolateral endoscopic surgery for pyogenic spondylodiskitis: Results of 15 patients with serious comorbid conditions. Spine (Phila Pa 1976). 2007;32:200-6.
- [CrossRef] [PubMed] [Google Scholar]
- Identifying pathogens of spondylodiskitis: Percutaneous endoscopy or CT- guided biopsy. Clin Orthop Relat Res. 2008;466:3086-92.
- [CrossRef] [PubMed] [Google Scholar]
- Minimally invasive surgical treatment for tuberculous spondylodiskitis. Minim Invasive Neurosurg. 2009;52:250-3.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous diskectomy and drainage for postoperative intervertebral diskitis. Arch Orthop Trauma Surg. 2011;131:173-8.
- [CrossRef] [PubMed] [Google Scholar]
- Minimally invasive percutaneous endoscopic diskectomy and drainage for infectious spondylodiskitis. Biomed J. 2013;36:168-74.
- [CrossRef] [PubMed] [Google Scholar]
- Extended indications of percutaneous endoscopic lavage and drainage for the treatment of lumbar infectious spondylitis. Eur spine J. 2014;23:846-53.
- [CrossRef] [PubMed] [Google Scholar]
- Minimally invasive endoscopic treatment for lumbar infectious spondylitis: A retrospective study in a tertiary referral center. BMC Musculoskelet Disord. 2014;15:105..
- [CrossRef] [PubMed] [Google Scholar]
- Bilateral Portal Percutaneous Endoscopic Debridement and Lavage for Lumbar Pyogenic Spondylitis. Orthopedics. 2015;38:e856-63.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical outcome of percutaneous drainage for spondylodiskitis. J Neurol Surg A Cent Eur Neurosurg. 2014;75:7-11.
- [Google Scholar]
- Fungal spinal infection treated with percutaneous posterolateral endoscopic surgery. J Neurol Surg A Cent Eur Neurosurg. 2014;75:170-6.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous Endoscopic Lumbar diskectomy in Spondylodiscitis. In: Minimally Invasive spine Surgery (1st). MISSI/Jaypee; 2018. p. :134-44.
- [CrossRef] [Google Scholar]
- New emerging Gore Matrix: Basis of stitchless spine surgery under local anesthesia. J Orthop Allied Sci. 2017;5:1-5.
- [Google Scholar]
- Pyogenic and tuberculous spondylodiskitis (vertebral osteomyelitis) in 80 adult patients. Clin Infect Dis. 1994;19:746-50.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnostic yield of CT-guided percutaneous aspiration procedures in suspected spontaneous infectious diskitis. Radiology. 2001;218:211-4.
- [CrossRef] [PubMed] [Google Scholar]
- Destructive spine lesions: Diagnosis by needle biopsy. J Bone Joint Surg 1935:57-58.:749-58.
- [Google Scholar]
- CT-guided closed biopsy of the spine. J Comput Assist Tomogr. 1981;5:73-78.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous Endoscopic Debridement and Drainage with Four Different Approach Methods for the Treatment of Spinal Infection; Pain Physician. . 2017;20(6):E933-E940.
- [CrossRef] [Google Scholar]
- Outcome of percutaneous continuous drainage of psoas abscess: A clinically guided technique. Indian J Orthop. 2014;48:67-73.
- [CrossRef] [PubMed] [Google Scholar]




