
Translate this page into:
Percutaneous autologous stem cell enriched marrow concentrate injection for treatment of cases of impaired fracture healing with implant in situ: A cost-effective approach in present Indian scenario
Address for correspondence: Dr. Sachin Upadhyay, Assistant Professor Orthopaedics, 622, "Poonam" Sneh Nagar, State Bank Colony, Jabalpur - 482 002, Madhya Pradesh, India. E-mail: drsachinupadhyay@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Upadhyay S, Varma HS, Yadav V. Percutaneous autologous stem cell enriched marrow concentrate injection for treatment of cases of impaired fracture healing with implant in situ: A cost-effective approach in present Indian scenario. J Orthop Allied Sci 2016;4:18-29.
Abstract
Background:
The objective of present study is to investigate the feasibility of proposed methodology in present Indian scenario, to enhance fracture repair in cases of impaired healing with the implant in situ using autologous bone marrow concentrate. During critical analysis, the existing study also aimed to assess the outcome (both objective and subjective) as well as to document complications specific to the proposed therapy if any.
Materials and Methods:
First the marrow is aspirated from posterior iliac crests. After that Ficoll-Paque technique of density gradient separation for the isolation of mononuclear cell populations enriched with stem cells is employed. Later, the concentrate is injected into critical-sized defects of eight patients with stable fracture delayed/nonunion via fluoroscopic guidance. New bone formation was evaluated by X-rays in two standard planes (anteroposterior (AP)/lateral). Level of statistical significance was set at a P < 0.05.
Result:
The critical osseous defect reached radiographic observable union by a mean of 12.28 ± 1.38 weeks. A distance of 5 mm or less between the fractures' ends resulted in healing in seven cases (87.5%). The results of the Likert four-point scale showed that majority were very satisfied with the outcome of the procedure (Cronbach's alpha coefficient (follow-up): 0.93 (6 week); 1.0 (1 year)). There were no adverse events reported during the procedure.
Conclusion:
Our preliminary results indicate that the approach proposed is feasible and effective in the management of stable (implant in situ) fracture with impaired healing. In context of its cost-effectiveness, we recommend to follow proposed methodology in present Indian scenario.
Keywords
Bone marrow concentrate
Cronbach′s alpha coefficient
delayed union
ficoll-paque
fracture healing
Likert scale
nonunion
stem cells

Introduction
Impaired fracture healing is a common clinical problem confronting the treating surgeon, and can have significant impact on the quality of life for patients who have it with regard to physical, functional, psychologic, and financial domains.[1] Recognizing the potential biologic value and low risk of operative complications,[2] many surgeons have used bone marrow aspirate injection as an alternative to conventional autogenous open cancellous bone grafts from the iliac crest. There have been several controlled studies[3,4,5] that demonstrated beneficial effects attributed to the availability of osteoprogenitor cells[4,6] in disturbed fracture healing. The efficiency of bone marrow aspirate can be significantly increased either by centrifugation[7] or by limiting the volume of aspiration from a given site to 2 cc or less.[8]
All relevant studies[4,9,10,11,12] used cumbersome, highly sophisticated equipments for concentration of mononuclear cells. The desires and expectations of patients may be quite different in developing countries, and may impact upon treatment planning. These "critical concerns" focus attention on the pressing question that remains difficult to answer in a world of limited healthcare resources: "Is it possible to use such automated equipments in resource-limited settings? Is it feasible to produce results consistent with the published data using simple centrifugation system and that too in a cost-effective manner?" The answer will have significant impact on access to these cost-effective interventions and, thus, management of impaired fracture healing in developing countries. As noted by Christensen et al., the market for simple, elective operative interventions no longer rewards higher functionality, but rather rewards convenience, accessibility, low cost, and reliability.[13]
Besides several risk factors[14] that can interfere with fracture healing; in developing countries like India, therapeutic noncompliance is crucial. This is attributed to low literacy skills, long distances which have to be travelled to access specialty care, inadequate transportation systems or the cost of travel as well as social and economic factors. There is thus an acute need to develop a basic operational process using simple compact laboratory equipments by which surgical services deployment occurs in peripheral, resource-limited settings.
The primary aims of the present study are twofold. The first goal is to investigate the feasibility of the proposed methodology to enhance fracture repair in cases of impaired healing with implant in situ using autologous bone marrow concentrate enriched with mesenchymal stem cells (MSCs) in poor infrastructural setup. The study's second aim is to assess critically the outcomes (both subjective and objective) as well as to document complications specific to the proposed therapy if any.
Materials and Methods
All the patients' acknowledgement (informed consent) to undergo the aforementioned process was received before beginning with the study. The study was approved by the Research Ethical Committee of NSCB Medical College Hospital. Among 12 registered patients with radiological evidence of impaired fracture healing with implant in situ screened at our outpatient clinic, a total of eight patients (two females and six men) with a mean age of 39.5 ± 14.3 years (range, 24-68 years) [Table 1] were enrolled.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (i) Patients of either sex, 18-65 years of age, (ii) radiographic evidence of disturbed fracture union (with no progression of fracture healing over 3 consecutive months) with the implant in situ. Non progression of fracture healing was further defined on radiographs by: (i) absence of bone crossing the fracture site, (ii) persistent fracture line(s), and (iii) lack of evidence of progression of healing on serial imaging.
The exclusion criteria were as follows: (i) Active infection, (ii) active inflammatory or connective tissue disease (i.e., lupus, RA); (iii) any medical comorbidity such as cardiac or pulmonary disease, endocrine disorder; (iv) hypersensitivity to nonsteroidal anti-inflammatory drugs (NSAIDs), abnormal liver or kidney function tests, history of peptic ulceration and upper gastrointestinal hemorrhage, cancer, and hyperkalemia; (v) history of coagulopathies and hematological or neurological disorders; (vi) and/or any other conditions that in the our opinion, would make participation not in the best interest of the patient or could prevent or limit the protocol-specified outcome assessment.
Study design
The study was designed as a single-center prospective research. The steps were as shown in Figure 1.

- Study design: Schematic flow chart showing different steps
Device description
The present study utilized a REMI centrifuge C-854/6 System [Figure 2].

- REMI centrifuge C-854/6 System
Methodology
Before conducting the procedure, osseous defect was measured approximately by X-rays in two planes (anteroposterior (AP) and lateral view).
Aspiration of bone marrow
With all aseptic precautions under local anesthesia (1% lidocaine without epinephrine) in prone position, a small 2-mm skin incision was made with a sharp pointed scalpel blade over posterior iliac crest. The aspiration needle (16G) is pointed anterolaterally in the direction of the iliac crest and was advanced slowly through the incision. The beveled needle was securely placed within the marrow cavity/spongy bone;[15] the marrow aspirated into a Dispovan 20 ml plastic syringe (heparin rinsed). At a given depth, the needle is turned 45° during successive aspirations to reorientate the bevel, thereby facilitating aspiration from larger space. After the tip is swept around a full circle, the needle was withdrawn approximately 1 cm proximally and successive aspirations were begun, repeating the same procedure.
Processing and density gradient centrifugation
We employed Ficoll-Paque technique of density gradient separation for the isolation of mononucleated cells. As this technique takes advantage of the density differences between mononuclear cells and other elements found in the blood sample, it yielded a virtually Red blood cells (RBCs)-free bone marrow cell suspension as described by Wells et al.[16] Heparinized marrow was diluted 1:1 in phosphate-buffered saline (PBS) and carefully layered over the Ficoll-Paque gradient in approximately 1:2-2.5 ratio (Ficoll-Paque solution of 1.077 g/ml density; ~1:2.5[17]). The bone marrow aspirate was then concentrated using the centrifugation system (REMI centrifuge C-854/6) [Figure 2] for 10 min at 500 g (~2,000 rpm) in the operating room at room temperature. The majority of the mononucleated cells and platelets accumulated on top of the Ficoll-Hypaque layer because they have a lower density; in contrast, RBCs and granulocytes have a higher density than Ficoll-Hypaque and sediment at the bottom of the Ficoll-Hypaque layer [Figure 3]. The mononuclear cell interface layer was harvested carefully using long bore micropipette after discarding the supernatant. The resultant mononuclear cells were resuspended twice in PBS (for 5 min at 500 g (~2,000 rpm) [Figure 4]. This technique reduces 120 ml of bone marrow aspirate to a 'concentrated myeloid' suspension of about 6-7 ml. The concentrate transferred by sterile technique back to the sterile field for reinjection. Both aspirate and concentrate (1 mL were saved of each sample for in vitro analyses) were analyzed using flow cytometry (fluorescence activated cell sorting (FACS)) regarding the containing cells [Figure 4]. One drop of concentrate is taken on the slide for staining with trypan blue dye (1:1) to assess the viability of mononuclear fraction. Sample is also sent for culture and sensitivity test. Rest is preserved for injection under IITV control. The concentration factor was calculated cell count-quotient bone marrow aspirate concentrate (BMAC)/aspirate after the centrifugation procedure.
- Showing Density gradient sedimentation. (a) RBCs and granulocytes; (b) clear layer of Ficoll; (c) buffy colored mononuclear fraction; and (d) clear layer of plasma. RBC = Red blod cell
- (a) Buffy colored concentrate of mononuclear fraction after washing (twice) with PBS and (b) a magnified view. PBS = Phosphate-buffered saline
Injection of BMAC (in vivo application)
The diluted BMAC (2 ml) is injected slowly at a defect site. After the injection, the needle is gradually withdrawn, with small oscillating motions being made to fill in the path of the needle.
Postprocedure protocols
Drugs: Analgesic (for 3 days and then Si opus sit), antacid (for 3 days), antibiotics (for 3 days), and supplements (calcium and multivitamins). Immobilization: 4-6 weeks. Physiotherapy: Active, assisted physiotherapy and mobilization of adjacent joints. Weight bearing: Partial weight bearing (toe-touch): Week 6-10 and full weight bearing: Week 10-12 (considering compliance of the patient and bone quality; clinical and radiological parameters). X-ray assessment (at least two planes): To record the orientation of implants, and also it provides a basis for the evaluation of how fracture healing is progressing.
Criteria for evaluation of outcome
Clinical[18]
Pain (if any): pre- and postprocedure (visual analog scale (VAS) score activity);[19] tenderness at the fracture site (if any).
Radiological:[18,19,20] pre- and postprocedure
Critical osseous defect was measured approximately by X-rays in two planes (pre- and postprocedure) and cortical continuity and progressive loss of the fracture line (postprocedure).
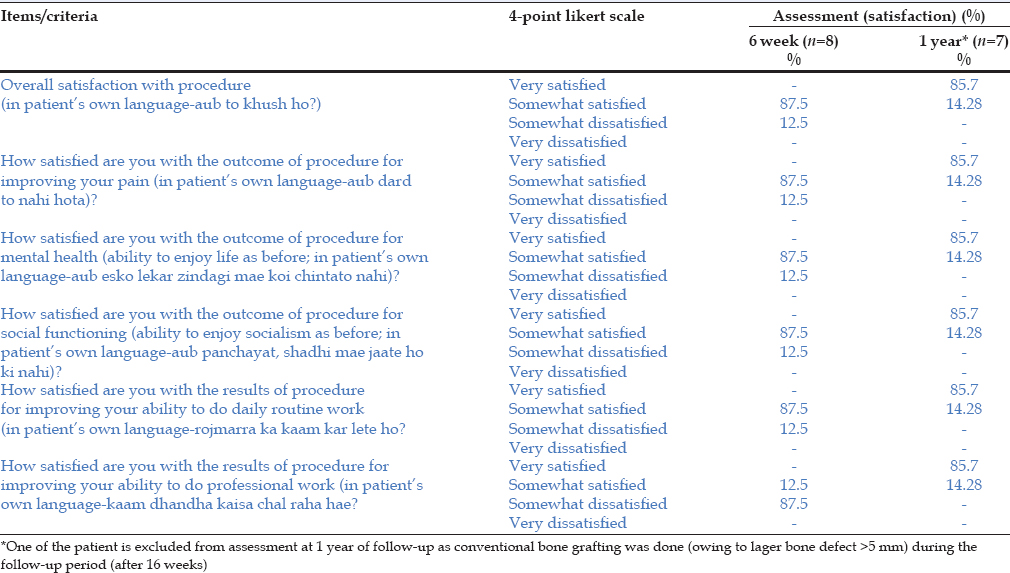
Subjective: (4-point Likert scale (Likert response scale)[21]
Six items/criteria, as determined by an expert consensus panel-an orthopedic surgeon, physiotherapist, and a psychiatrist/behavioral scientist-were chosen; although not specific, yet are significant enough to interfere with patients' functioning, mostly affected by surgical procedures. The items include patients' overall satisfaction with procedure, the extent of pain relief, mental health (ability to enjoy life as before), social functioning (ability to attend social functions as before), the ability to perform routine work at home, and the ability to perform professional activities. Items are scored on a 4-point Likert scale with response categories consisting of: Very satisfied (100 points), somewhat satisfied (75 points), somewhat dissatisfied (50 points), and very dissatisfied (25 points). The current scale score is the unweighted mean of the scores from the individual items, ranging from 25 to 100 per item (with 100 being very satisfied). Face validity was assessed by having the scale reviewed by a panel of independent experts in the field of orthopedics. The internal consistency or reliability of the scale was evaluated using the Cronbach's alpha coefficient.
Statistical analysis
The data are presented as means ±standard deviation (SD). All calculations and statistics were performed with Statistical Package for Social Sciences (SPSS 20) software. A P - value of less than 0.05 (P < 0.05) was regarded as significant. The internal consistency (reliability) of the scale was assessed using Cronbach's alpha coefficient.
Results
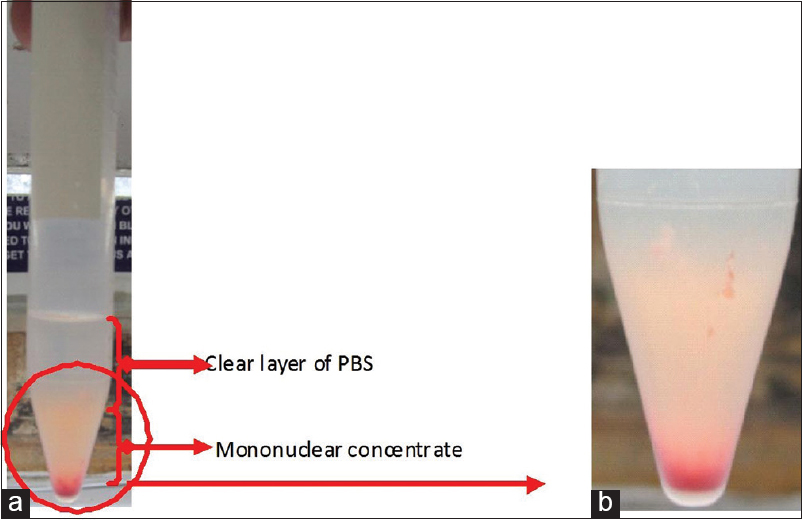
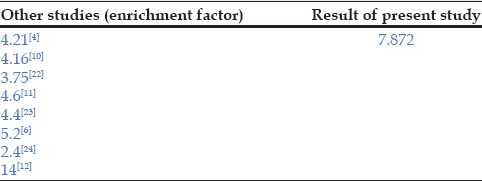
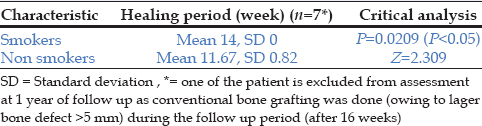
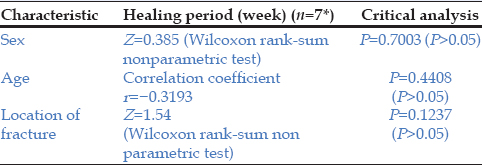
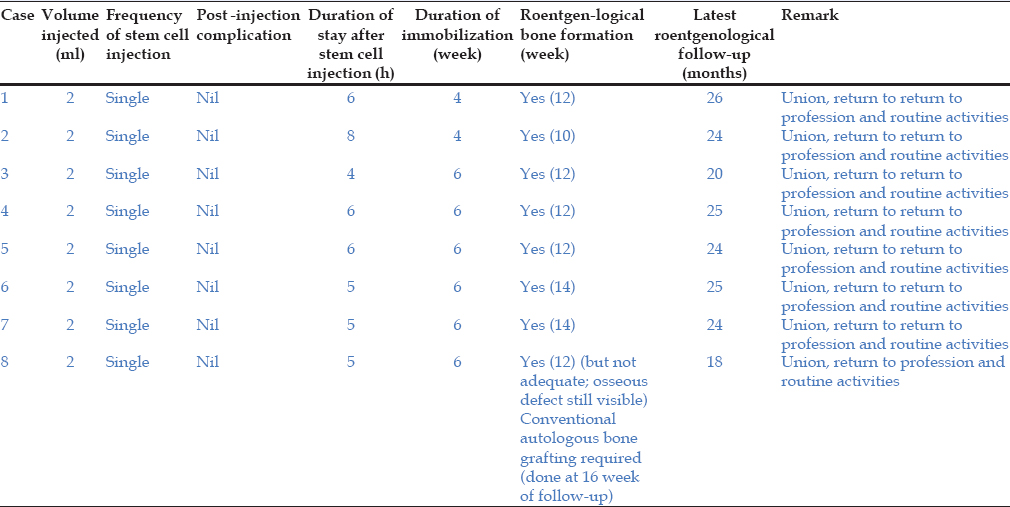
The mean interval from injury to percutaneous BMAC injection was 24.9 ± 7.9 months [Table 1]. The in vitro analysis of aspirate and BMAC showed significant concentration of mononuclear fraction after centrifugation (before 16.55 ± 0.5127/μL; after centrifugation viable CD34 = 129.55 ± 10.01513/μL; (P < 0.05)). The average concentration factor of the BMAC compared to the aspirate was 7.82 (SD 5.25) [Table 2]. The viability of fresh cells was 94.7 ± 3.6% (ranged from 88.6 to 98.0%). In vitro analysis showed a viability level of 75.7 ± 9.16% (ranged from 68 to 90.2%). None of the samples in present study was culture-positive. A positive radiographic response was detected after 4.5 ± 0.462 weeks of stem cell enriched fraction injection. The critical defect 2.6 ± 6.5 mm reached radiographic observable union by a mean of 12.28 ± 1.38 weeks [Table 1]. The mean immobilization period following intervention was 5.5 ± 0.92 weeks [Table 1]. All except one patient (patient 8) in the present study showed fracture healing (87.5%) and/or sufficient new bone formation within follow-up and majority of our patients have significant symptomatic improvement and good return to full prefracture functional activities. The one unsuccessful case (patient 8) had bone defect greater than 5mm and open bone grafting was necessary within the follow-up period (patient 8 is excluded from assessment at 1 year of follow-up). The time to union was significantly longer for smokers (14 weeks) than for others (11.6 ± 0.89 weeks; P < 0.05) [Table 3]. Furthermore, the mean time to union for fractures in the context of demographic variables (age (P = 0.4408), sex (P = 0.7003), and location (P = 0.1237)) was not significantly different (P > 0.05) [Table 4]. All patients experienced a significant reduction in pain after the procedure during follow-up period (P < 0.05). The mean hospital stay following procedure was 5.625 ± 1.18 h. No peri- and/or postoperative complications have been found. At the mean follow-up of 10.85 (SD 0.89) months after treatment, all patients returned to their profession. There were no restrictions to any physical activities at latest follow-up (23.25 ± 2.76 months) [Table 1]. With regard to subjective satisfaction, seven out of eight patients (87.5%) were satisfied [Table 5]. One patient (patient 8), for whom the indication of open bone grafting was made during the further course of recovery, evaluated the procedure as somewhat dissatisfactory at 6 week of follow-up. Cronbach's alpha coefficient for internal consistency of the satisfaction scale is 0.93 at 6 week and 1.0 at 1 year of follow-up [Table 6]. Table 7 gives detailed information about the outcome in patients who received stem cell enriched mononuclear fraction injection after Ficoll-Hypaque gradient centrifugation technique. The follow-up X-rays of case 3, 4, and 7 [Tables 7 and 8] are shown in Figures 5-7.

- (a) Nonunions with implant in situ; (b-d) after bone marrow concentrate injection; (d) showing consolidation (latest follow-up) (case 3)
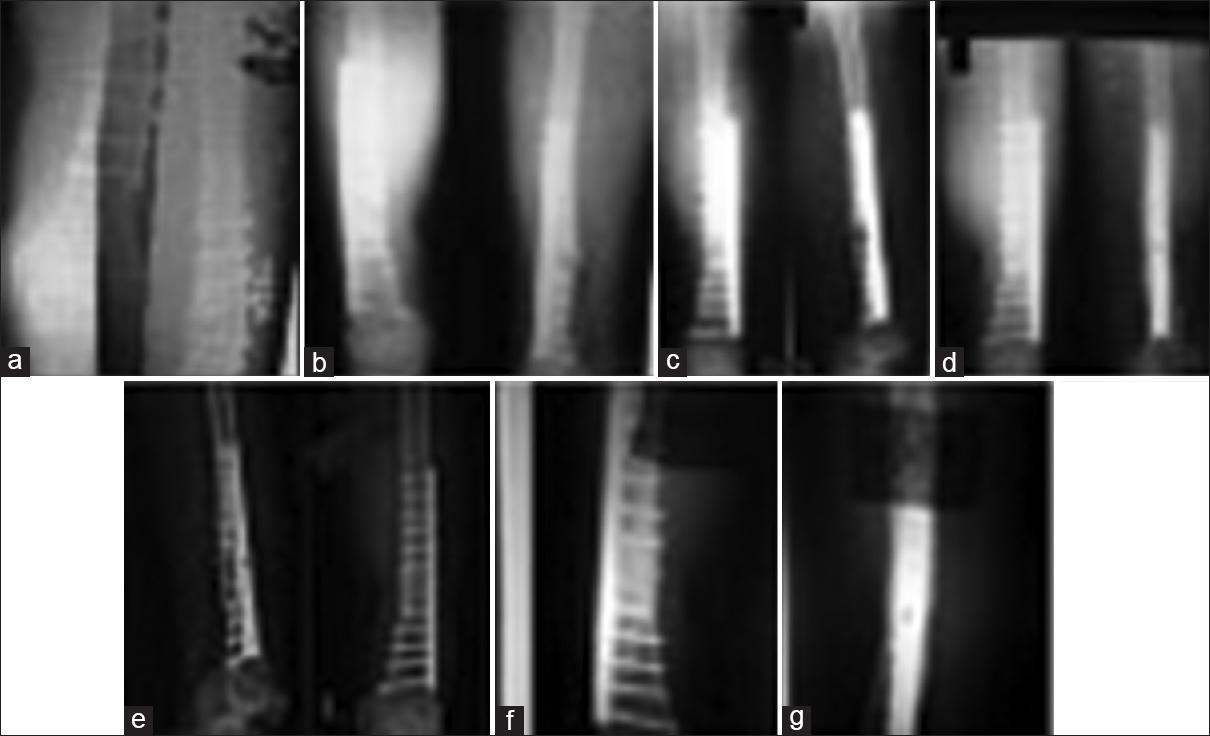
- (a and b) Nonunions with implant in situ; (c-g) after bone marrow concentrate injection (f); (g) showing consolidation (latest follow-up) (case 4)
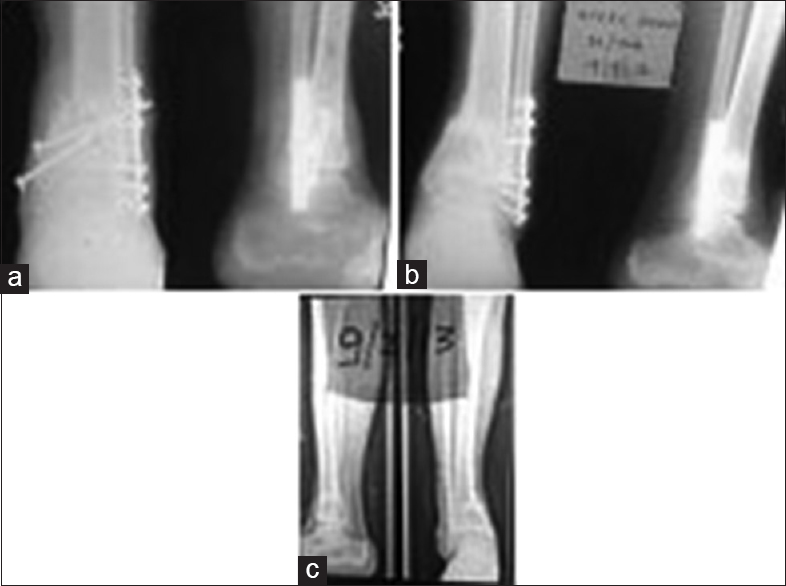
- (a) Nonunions with implant in situ; (b and c) after bone marrow concentrate injection; (c) showing consolidation (latest follow-up) (case 7)


Discussion
Impaired fracture healing, leading to delayed union or nonunion,[25] is a multifactorial phenomenon[26] and can cause significant changes in a person's personality (personal and professional productivity (i.e., paid and unpaid), lifestyle, and ability to function-all of which compromise patients' health-related quality of life, thus necessitating the need to consider more aggressive intervention. Currently, numerous methods are employed to deal multitudinal problems associated with impaired fracture healing: Stable osteosynthesis,[27,28] bone grafts,[29] microvascular bone transplants,[30] biophysical therapies,[31] and the Ilizarov method of distraction osteogenesis.[32,33] None of these methods yield satisfactory outcome. Further more, all these procedures require convoluted surgical procedures and are usually associated with increased morbidity and various complications.
MSCs are immature, natural, resident, pluripotent cells of bone marrow with a wide spectrum of differentiation proliferative capacity.[34] MSC have an inherent capability to differentiate into cells of three blastophyllums (ectoderm, mesoderm, and endoderm).[35] Currently, it is difficult to discern the underlying mechanism, but most probably it could be either direct due to their intrinsic ability for repair and regeneration or indirect through their immunomodulatory and paracrine effects.[36] There is still an ongoing debate regarding the mechanism of action of MSCs at cellular and molecular level. Several studies[6,37,38] reported that bone marrow-derived mononuclear cells are able to elicit angiogenesis, thus significantly enhancing blood flow at the fracture site and inherently delivering the core components, such as growth factors and cytokines that play a vital role in the normal healing process.
Owing to ample supply, presence of osteogenic progenitor cells[34] and associated minimal donor and recipient site morbidity makes percutaneous bone marrow implantation for the treatment of impaired fracture healing as a low risk inexpensive procedure with high biological activity.[39]
Though there are substantial evidences[40,41,42] that bone marrow injection can accelerate and augment the fracture-healing process in cases of impaired healing, like all techniques, it has certain limitations that need to be taken into account when considering this procedure. Any preexisting angular deformities, prior shortening, large critical sized defect, or gross displacement of the fragments; making percutaneous injection of the bone marrow impossible.[43] The prior studies[44,45] have demonstrated that normal marrow has significantly lower proportion of MSCs; further limits its use if the concentration of progenitors is critical. It has also been previously demonstrated[8] that larger aspirate volume is associated with decrease concentration of progenitor's cells because of dilution of the sample with peripheral blood. So this approach may be least applicable in situations where success is entirely dependent on the transfer of sufficient numbers of osteoprogenitors cells. It is frequently impractical to harvest adequate bone marrow with the required number of osteoprogenitor cells. Therefore, techniques (differential centrifugation, selective-retention,[46,47] or ex vivo or culture-expanded cell technology)[48,49,50] capable of increasing the volume of osteoprogenitor cells are of great clinical benefit.
The directives for in vitro and ex vivo analysis of bone marrow cells follows certain, stringent requirements.[51] Additionally, there are well-documented complications such as contamination or significant diminution of regenerative capabilities, as well as additional costs, including personnel expenses, automated laboratory and culture instruments, and actinic and contagion tests.[52,53]
Though Clinical benefit has been shown, but unfortunately the high cost and stringent requirements of these techniques has led to concern about their appropriate use, especially in developing countries context.
From Indian perspectives
In developing countries like India, the most important factor in fracture healing is affordability.[54] In developing world, impaired fracture healing has profound human and socioeconomic consequences in all societies. The economic effects of fracture healing impairment can be divided into direct and indirect costs.[55,56] Furthermore, the psychological and physical trauma to the patient when faced with the prospect of another surgery is often underestimated. Although no hospital-specific data are available, any multispecialty hospital treats almost 500-700 cases of impaired fracture healing per year.[57] There are number of such tertiary care centers in each metropolitan city, hence India has to deal with an enormous burden of complicated fractures.[54,57] If we aim at providing maximum relief to the largest number we will have to develop and adopt techniques to suit our requirements.[58] The developed countries do not have to conduct research for our clinical problems. Mere importation of sophisticated, expensive equipments and methodology; however, does not solve the problem. We have to find out solutions to our problems as well as devise cost-effective problem-solving strategies to one and all.[59,60]
For these reasons, an impetus exists to develop and validate alternative cost-effective technique in developing country contexts using simple laboratory centrifugation system and locally available equipments/reagents that is capable of replicating the performance of the published literatures significantly, while dramatically reducing the cost (both tangible and intangible), complexity of sophisticated procedure, and is accessible and affordable to mass population.
In our setting, the proposed technique enriched population of bone marrow-derived cells by a factor of 7.82 (before 16.55 ± 0.5127/μL; after centrifugation viable CD34 = 129.55 ± 10.01513/μL (P < 0.05)) [Figure 4]. Consequently, concentration capacity of the current centrifugation system was more efficient than the enrichment factor of published literature [Table 2]. Furthermore, we strongly support Kasten et al., who reported higher MSC yields [Table 2] owing to effective isolation technique (SEPAX VOL RED protocol) of the MSCs.[12] In agreement with previous studies,[8,61] in present pilot study cellular concentration showed considerable individual variations (range 1.98-19.1); probably due to physiological variables (age, menopause), associated co-morbidities (smoking), or technical reasons/variables. The authors also agreed with the fact that the concentration of osteoprogenitor cells may vary significantly between individuals, aspiration sites, aspiration technique, and isolation protocols.[8,12,61] In the current study, flow cytometric analysis [Figure 8] were done just to determine the subset of circulating cells expressing the CD34 antigen to assess the progenitor cell content in the whole marrow and after density gradient centrifugation, that is, in concentrate (the facility for CD specific for MSCs are not available; in view of that we used CD34 just to assess the efficiency of concentration). Alternation in preservation or processing of bone marrow concentrate significantly reduces the number of viable CD34 + cells available for reinfusion[62] as also noted in the present series (viability of fresh cells was 94.7 ± 3.6%; in vitro analysis showed a viability level of 75.7 ± 9.16%; P < 0.05). An immediate autologous injection of bone marrow concentrate dramatically improves the quality of cells as it significantly reduces the complications pertaining to preaging, decreased cell viability, or dedifferentiation that are usually associated with in vitro cultivation.[63,64] Therefore, "one-step" isolation/application of MSCs enriched fraction with on-table preparation was advocated, as it increases the viability of cells while reducing the cost and infection rates by decreasing the ex vivo time period.
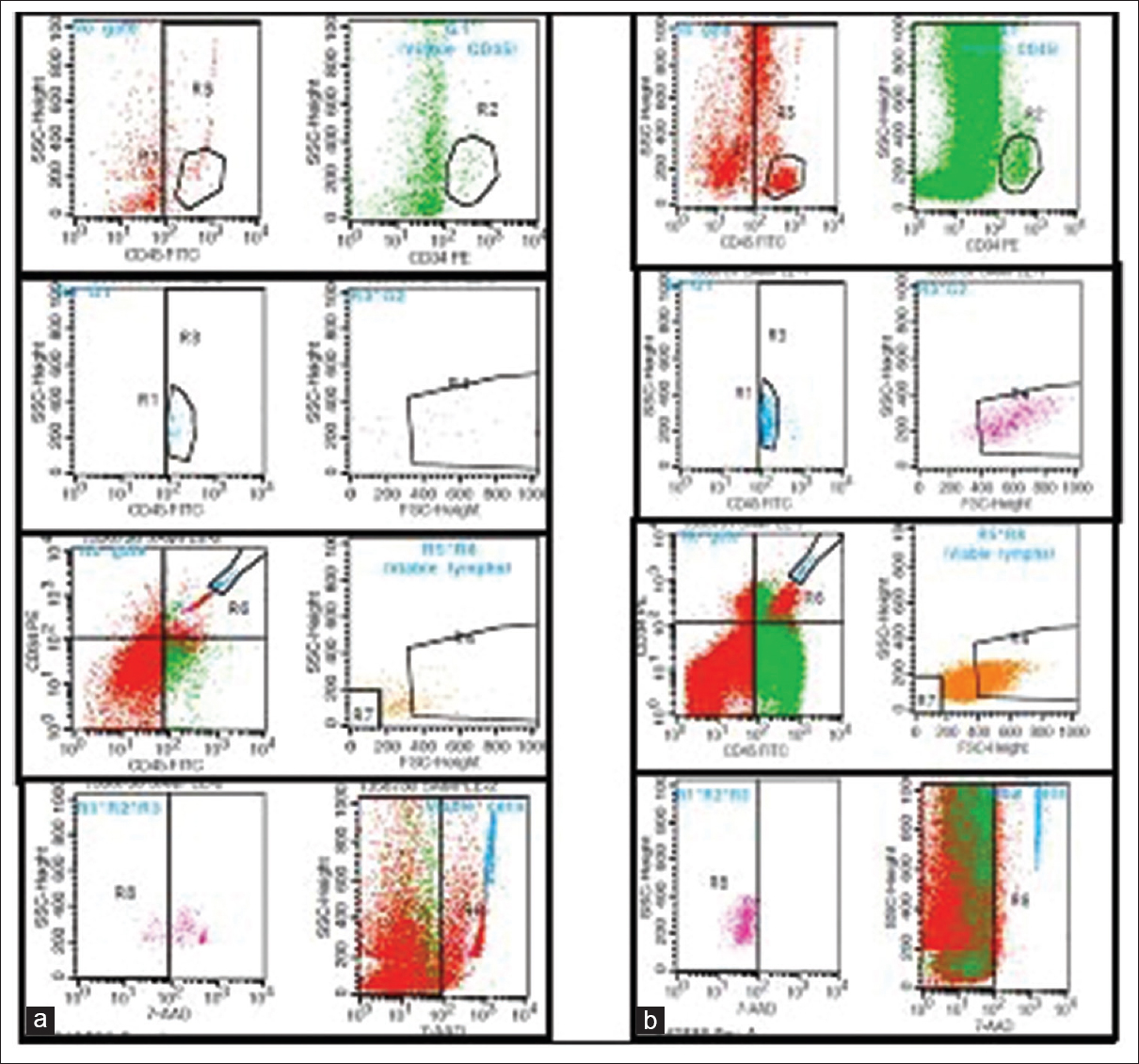
- Flow cytometric analysis of aspirate (a) and concentrate (b); showing significant concentration of mononuclear fraction (CD34, CD45, and lymphs)
The result from existing prospective study strongly supported previous studies'[4,9,10,11,64] [Table 2] concepts that centrifugation increases the efficiency of bone marrow owing to increase the concentration of osteoprogenitor cells.
Defect or distance between the fracture ends is a critical factor for success of healing; a distance of 5 mm or less between the fractures ends resulted in healing in all cases except one in present series. Previous study[4] has also reported a significant association between fracture gap and outcome. The one unsuccessful case had bone defect greater than 5 mm and open bone grafting was necessary within the follow-up period.
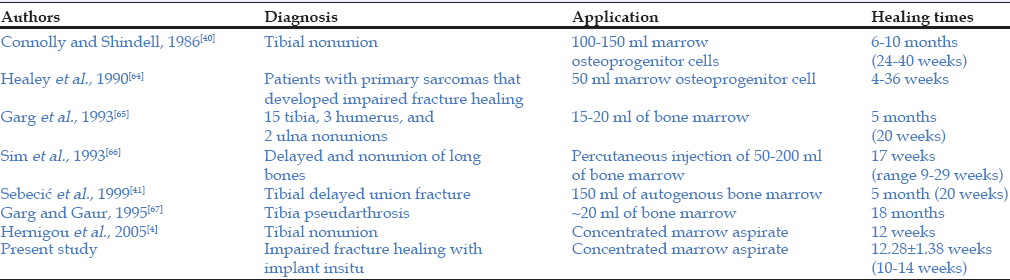
In current study, in an average of 12.28 (SD1.38) weeks, a bony union was achieved in seven of eight patients [Table 1]. This finding is consistent with that of Hernigou et al.[4] It has also been noted that patients who received bone marrow concentrate injection experienced a lower time to union [Table 9]. This efficacy can be attributed to the implantation of increased concentration of osteoprogenitor cells. The number and concentration of the stem cells being injected, affected the clinical outcome.[4] Greater the concentration of osteoprogenitor cells, less will be the healing period.
Based on the critical data analysis of present series, it was found that there was no significant relationship (P > 0.05) among demographic variables (e.g., age and sex) [Table 4] and treatment outcome; as also concluded by Hernigou et al.[4] This indifference indicates a common etiologic basis, that is, locally decreased population of progenitors.[68] Although the location of the fracture appeared in earlier study[6] to influence the healing, we were unable to confirm this [Table 4]. One fundamental reason for this issue is smaller sample size and other could be attributed almost entirely to the existing biomechanical environment.[68,69] Furthermore, patients with comorbidities (smoking) took a longer time to heal (average 14 weeks) than other patients (11.6 weeks (SD 0.89); P < 0.05) [Table 3]. Several studies[70,71,72] have shown that consolidation of a fracture is often delayed in heavy smokers and drinkers owing to overall reduction in the numbers of progenitor cells in the bone marrow. In the present series, there were only two smokers [Table 1]. Consequently, the low rate of smokers led to the low mean value in present series, probably resulting in a lack of correlation between outcome and smoking behavior.
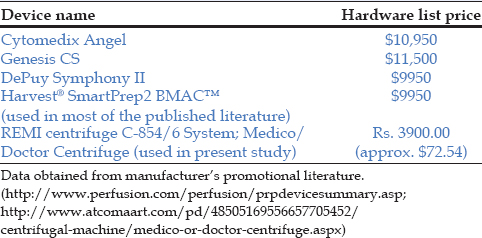
Most of published techniques[4,9,10,11,12,17,64] need special, sophisticated devices; but in practice, high logistical requirements and exorbitant cost of these commercially available kits restricts their widespread use. Availability has been limited to research centers, and it remains quite expensive. For this reason the present research is currently focused on the development of methodology that is feasible with low-cost devices. The critical analysis reveals a large difference in costs of hardware device of present study and others [Table 10]. Furthermore, the device used in the present study [Figure 2 and Table 10] is easily available even at second and third tier of Indian three-tier system[68,73] of health care's.
Patient satisfaction is an integral part of modern quality management. Treating surgeon should analyze the patient's expectations with respect to surgery: Labors, farmers, and office or sedentary workers; all have different needs. Therefore, a doctor's treatment protocol should not only be limited to objective measures but also include background information about the patient's lifestyle and profession (subjective measures).
Although many authors have reported on patient satisfaction after arthroplasty,[74,75,76,77] we are unaware of any validated self-report scale that evaluates patient satisfaction after percutaneous BMAC injection. In our setting, the majority of responses were in the very satisfied or somewhat satisfied categories [Table 5]. During the follow-up period after 6 week, more patients (87.5%) were satisfied with pain relief, their mental health and social functioning, and their ability to do daily activities compared to improvement in their ability to do professional activities [Table 5]. Further, it was found that the total satisfaction scores were gradually increased over the subsequent follow-up visits (85.7%: very satisfied and 14.28%: Somewhat satisfied) [Table 5].
In the present study, one out of eight patients [Table 5] is somewhat dissatisfied following proposed intervention. Potential reasons for patient dissatisfaction with intervention may be poor mental health or unfulfilled expectations (a further research study will also help to find out the causes for dissatisfaction). In present series, Cronbach's alpha coefficient for internal consistency of the satisfaction scale is 0.93 at 6 week and 1.0 at 1 year of follow-up, suggesting excellent reliability [Table 6]. In conclusion, present satisfaction scale may be used to evaluate the complex relationship between patient's baseline parameters (items) with outcome.
In present series, there has been no hematoma formation, or infection at the site of aspiration. None of the patients in the current study reported chronic pain at aspiration site. In none of the cases we had to repeat the procedure to achieve union. Aspiration of bone marrow from the iliac crest has not been a "rate-limiting" factor in rehabilitation or a risk factor for prolonged hospital stay.
In context with the present cohort and diamond model for bone-fracture healing,[77] it is an arduous task for to speculate as to whether or not BMAC is an effective therapy in cases of unstable fracture with impaired healing process. Furthermore, any scaffold has not been used in present study. In fact, it is anticipated that the use of needle during the procedure to deliver the BMAC to the target site seems to be traumatic enough to create a whole marrow scaffold.
Conclusion
We have conclusively demonstrated the feasibility of the proposed cost effective therapy in the context of limited healthcare resources in developing countries. This study's main strengths were the long period of follow-up (23.25 ± 2.76 months) and cost-effectiveness. The attractive feature of proposed therapy is that therapeutic osteoprogenitor cells can be delivered locally to the fracture site in relatively high concentrations and in a sustained fashion with an added advantage of its biological nature, low risk profile, and better patient compliance.
Limitations
Whilst the findings of the current study could be applied in most instances, there were some important limitations.
It is unclear whether only some or all stem cells in the concentrate differentiated into osteoblasts and integrating normally once injected. It is also difficult to tell that how many stem cells are required to induce bone regeneration in vivo.
The present study is nonrandomized and does not include any control groups and small sample size further limits the generalization of findings of present study.
Likert response scale yields ordinal rather than interval data.
Source of Support:
Nil
Acknowledgement
We want to acknowledge the doctors and senior colleagues for providing fruitful and critical comments on the draft of this paper.
Conflict of Interest:
None declared.
REFERENCES
- The epidemiology of fractures in England. J Epidemiol Community Health. 2008;62:174-80.
- [CrossRef] [PubMed] [Google Scholar]
- Morbidity at bone graft donor sites. J Orthop Trauma. 1989;3:192-5.
- [CrossRef] [PubMed] [Google Scholar]
- Autologous marrow injection as a substitute for operative grafting of tibial nonunions. Clin Orthop Relat Res. 1991;266:259-70.
- [CrossRef] [Google Scholar]
- Percutaneous autologous bone-marrow grafting for nonunions. Influence of the number and concentration of progenitor cells. J Bone Joint Surg Am. 2005;87:1430-7.
- [CrossRef] [Google Scholar]
- Percutaneous bone marrow grafting for the treatment of tibial non-union. Injury. 2005;36:203-6.
- [CrossRef] [PubMed] [Google Scholar]
- Growth factors released from bone marrow are promising tools in orthopedic surgery. Rev Rhum Engl Ed. 1998;65:79-84.
- [Google Scholar]
- Development of an osteogenic bone-marrow preparation. J Bone Joint Surg Am. 1989;71:684-91.
- [CrossRef] [Google Scholar]
- Aspiration to obtain osteoblast progenitor cells from human bone marrow: The influence of aspiration volume. J Bone Joint Surg Am. 1997;79:1699-709.
- [Google Scholar]
- Bridging the gap: Bone marrow aspiration concentrate reduces autologous bone grafting in osseous defects. J Orthop Res. 2011;29:173-80.
- [CrossRef] [PubMed] [Google Scholar]
- The use of percutaneous autologous bone marrow transplantation in nonunion and avascular necrosis of bone. J Bone Joint Surg Br. 2005;87:896-902.
- [CrossRef] [PubMed] [Google Scholar]
- Regenerate augmentation with bone marrow concentrate after traumatic bone loss. Orthop Rev (Pavia). 2012;4:e14..
- [CrossRef] [Google Scholar]
- Instant stem cell therapy: Characterization and concentration of human mesenchymal stem cells in vitro. Eur Cells Mater. 2008;16:47-55.
- [CrossRef] [PubMed] [Google Scholar]
- Will disruptive innovations cure health care? Harvard Business Rev. 2000;78:102-17.
- [Google Scholar]
- Risk factors contributing to fracture non-unions. Injury. 2007;38(Suppl 2):S11-8.
- [CrossRef] [PubMed] [Google Scholar]
- A technique for the separation and cryopreservation of myeloid stem cells from human bone marrow. Cryobiology. 1979;16:201-10.
- [CrossRef] [PubMed] [Google Scholar]
- Optimal blood mononuclear cell isolation procedures for gamma interferon enzyme-linked immunospot testing of healthy swedish and tanzanian subjects. Clin Vaccine Immunol. 2008;15:585-9.
- [CrossRef] [PubMed] [Google Scholar]
- Variability in the assessment of fracture-healing in orthopaedic trauma studies. J Bone Joint Surg Am. 2008;90:1862-8.
- [CrossRef] [PubMed] [Google Scholar]
- Accuracy of radiologic assessment of tibial shaft fracture union in humans. Clin Orthop. 1985;199:233-8.
- [CrossRef] [Google Scholar]
- Mid term results after bone marrow laser revascularization for treating refractory angina. BMC Cardiovasc Disorders. 2010;10:42..
- [CrossRef] [PubMed] [Google Scholar]
- Concentration of bone marrow total nucleated cells by a point-of-care device provides a high yield and preserves their functional activity. Cell Transplant. 2008;16:1059-69.
- [CrossRef] [PubMed] [Google Scholar]
- Bone marrow concentrate: A novel strategy for bone defect treatment. Curr Stem Cell Res Ther. 2009;4:34-43.
- [CrossRef] [PubMed] [Google Scholar]
- The role of bone growth stimulating devices and orthobiologics in healing nonunion fractures. In: AHRQ Technology Assessment Program. 2005.
- [Google Scholar]
- The effects of fixation on fracture-healing. J Bone Joint Surg Am. 1989;71:306-10.
- [CrossRef] [Google Scholar]
- Treatment of tibial malunions and nonunions with reamed intramedullary nails. Orthop Clin North Am. 1990;21:715-24.
- [CrossRef] [PubMed] [Google Scholar]
- Microvascular anastomoses for bone grafts in the treatment of massive defects in bone. J Bone Joint Surg Am. 1979;61:98-104.
- [CrossRef] [Google Scholar]
- The effect of low-frequency electrical fields on osteogenesis. J Bone Joint Surg Am. 1992;74:920-9.
- [CrossRef] [Google Scholar]
- The use of the Ilizarov concept with the AO/ASIF tubular fixateur in the treatment of segmental defects. Orthop Clin North Am. 1990;21:655-65.
- [CrossRef] [PubMed] [Google Scholar]
- The treatment of infected nonunions and segmental defects of the tibia by the methods of Ilizarov. Clin Orthop. 1992;280:143-52.
- [CrossRef] [Google Scholar]
- Bone marrow stromal stem cells: Nature, biology, and potential applications. Stem Cells. 2001;19:180-92.
- [CrossRef] [PubMed] [Google Scholar]
- Mesenchymal stromal cells: Current understanding and clinical status. Stem Cells. 2010;28:585-96.
- [CrossRef] [PubMed] [Google Scholar]
- Transplanted adult hematopoietic stems cells differentiate into functional endothelial cells. Blood. 2004;103:13-9.
- [CrossRef] [PubMed] [Google Scholar]
- Molecular mechanisms of blood vessel growth, Cardiovasc Res. 2001;49:507-21.
- [CrossRef] [PubMed]
- Self-reported recovery time of daily activity after bone marrow harvesting from healthy donors. J Anesth. 2001;15:1-5.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous autologous bone marrow grafting on the site of tibial delayed union. Croat Med J. 1999;40:429-32.
- [Google Scholar]
- Autologous iliac crest bone graft: Should it still be the gold standard for treating nonunions? Injury. 2007;38(Suppl 1):S75-80.
- [CrossRef] [PubMed] [Google Scholar]
- The use of percutaneous autologous bone marrow transplantation in nonunion and avascular necrosis of bone. J Bone Joint Surg Br 2005:87-902.:896-902.
- [CrossRef] [PubMed] [Google Scholar]
- Review injectable bone marrow preparations to stimulate osteogenic repair. Clin Orthop Relat Res 1995:8-18.
- [Google Scholar]
- Engineering principles of clinical cell-based tissue engineering. J Bone Joint Surg Am 2004:1541-58.:86-58.
- [CrossRef] [PubMed] [Google Scholar]
- Selective retention of bone marrow-derived cells to enhance spinal fusion. Clin Orthop Relat Res 2005:242-51.
- [CrossRef] [PubMed] [Google Scholar]
- The role of intraoperative bone marrow aspirate stem cell concentration as a bone grafting technique. Tech Foot Ankle Surg. 2008;7:84-9.
- [CrossRef] [Google Scholar]
- Mesenchymal stem cells in osteobiology and applied bone regeneration. Clin Orthop Relat Res. 1998;355(Suppl):S247-56.
- [CrossRef] [PubMed] [Google Scholar]
- Allogenic mesenchymal stem cell regenerate bone in a critical-sized canine segmental defect. J Bone Joint Surg Am. 2003;85A:1927-35.
- [CrossRef] [PubMed] [Google Scholar]
- Bone grafts prepared with selective cell retention technology heal canine segmental defects as effectively as autograft. J Orthop Res. 2006;24:857-66.
- [CrossRef] [PubMed] [Google Scholar]
- [Perspectives of clinical stem cell therapy in the treatment of musculoskeletal diseases in Germany] Z Orthop Unfall. 2010;148:149-54.
- [Google Scholar]
- Differential effects of culture-expanded bone marrow cells on the regeneration of bone between the femoral and the tibial lengthenings. J Pediatr Orthop. 2009;29:643-9.
- [CrossRef] [PubMed] [Google Scholar]
- Cellular strategies for enhancement of fracture repair. J Bone Joint Surg Am. 2008;90(Suppl 1):111-9.
- [CrossRef] [PubMed] [Google Scholar]
- Fracture healing in India: Available therapies, indications, and protocols. Indian J Orthop. 2009;43:175-81.
- [CrossRef] [PubMed] [Google Scholar]
- The health economics of the treatment of long-bone non-unions. Injury. 2007;38(S2):77-84.
- [CrossRef] [PubMed] [Google Scholar]
- Economic evaluation in orthopaedics. J Bone Joint Surg Am 2003:129-42.:85-42.
- [CrossRef] [PubMed] [Google Scholar]
- Musculoskeletal training for orthopaedists and nonorthopaedists: Experiences in India. Clin Orthop Rel Res. 2008;466:2350-9.
- [CrossRef] [PubMed] [Google Scholar]
- The art and science of orthopaedics in developing countries. J Bone Joint Surg Br. 1985;67:840-2.
- [CrossRef] [PubMed] [Google Scholar]
- Orthopedic services and training at a crossroads in developing countries. Indian J Orthop. 2007;41:177-9.
- [CrossRef] [PubMed] [Google Scholar]
- Research in orthopaedics: A necessity. Indian J Orthop. 2009;43:315-7.
- [CrossRef] [PubMed] [Google Scholar]
- Characterization of human bone marrow stromal cells with respect to osteoblastic differentiation. J Orthop Res. 1997;15:546-57.
- [CrossRef] [PubMed] [Google Scholar]
- Number of viable CD34 (+) cells reinfused predicts engraftment in autologous hematopoietic stem cell transplantation. Bone Marrow Transplant. 2002;29:967-72.
- [CrossRef] [PubMed] [Google Scholar]
- Transdifferentiation potential of human mesenchymal stem cells derived from bone marrow. FASEB J. 2004;18:980-2.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous bone marrow grafting of delayed union and nonunion in cancer patients. Clin Orthop. 1990;256:280-5.
- [CrossRef] [Google Scholar]
- Percutaneous autogenous bone marrow grafting in 20 cases of ununited fracture. Acta Orthop Scand. 1993;64:671-2.
- [CrossRef] [PubMed] [Google Scholar]
- Autologous marrow injection in the treatment of delayed and non-union in long bones. Singapore Med J. 1993;34:412-7.
- [Google Scholar]
- Percutaneous autogenous bone-marrow grafting in congenital tibial pseudarthrosis. J Bone Joint Surg Br. 1995;77:830-1.
- [CrossRef] [Google Scholar]
- Early histological and ultrastructural changes in medullary fracture callus. J Bone Joint Surg. 1991;73:832..
- [CrossRef] [Google Scholar]
- The biology of fracture healing: Optimising outcome. Br Med Bull. 1999;55:856-69.
- [CrossRef] [PubMed] [Google Scholar]
- Pseudarthrosis is treated by percutaneous autologous bone marrow graft. Rev Chir Orthop Reparatrice Appar Mot. 1997;83:495-504.
- [Google Scholar]
- The effect of nicotine of bone graft: An experimental study in rabbits. J Orthop Tran. 1993;17:1083..
- [Google Scholar]
- Bone marrow reconversion in adults who are smokers: MR imaging findings. AJR Am J Roentgenol. 1993;161:1217-21.
- [CrossRef] [PubMed] [Google Scholar]
- India Country Health System Profile 2006-2007. Available from: http://www.searo.who.int/EN/Section313/Section1519.htm
- [Google Scholar]
- National Joint Registry for England and Wales. The role of pain and function in determining patient satisfaction after total knee replacement. Data from the national joint registry for England and Wales. J Bone Joint Surg Br. 2007;89:893-900.
- [CrossRef] [PubMed] [Google Scholar]
- Patient versus surgeon satisfaction after total hip arthroplasty. J Bone Joint Surg Br. 2003;85:495-8.
- [CrossRef] [Google Scholar]
- Patient satisfaction after total knee arthroplasty: A comparison between subjective and objective outcome assessments. J Arthroplasty. 2001;16:740-7.
- [CrossRef] [PubMed] [Google Scholar]
- Enhancement of fracture healing with the diamond concept: the role of the biological chamber. Injury. 2011;42:1191-3.
- [CrossRef] [PubMed] [Google Scholar]




