
Translate this page into:
Osteofibrous dysplasia mimicking exostosis
Address for correspondence: Dr. Priyank Sahoo, Department of Orthopaedics, Era's Lucknow Medical College, Sarfarazganz, Lucknow - 226 003, Uttar Pradesh, India. E-mail: p.sahoo03@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Sahoo P, Khan AA. Osteofibrous dysplasia mimicking exostosis. J Orthop Allied Sci 2019;7:28-30.
Abstract
Osteofibrous dysplasia is an uncommon benign fibro-osseous lesion of childhood, more often seen in maxilla and mandible. Among a long bone, it is usually encountered in the tibia as a painless swelling or anterior bowing. Osteofibrous dysplasia mimicking exostoses has never been reported in the literature, to the best of our knowledge. Here, we would like to present an unusual case of osteofibrous dysplasia of the tibia clinically mimicking exostoses.
Keywords
Exostoses
fibro-osseous lesion
osteofibrous dysplasia

Introduction
The term osteofibrous dysplasia also known as Kempson-Campanacci lesion or cortical fibrous dysplasia is not a true neoplasm rather a fibrovascular defect.[1,2] Exact cause is still an enigma. Accounting for 0.2% of all primary bone tumors, this distinct entity is seen in thefirst two decades of life and is rare after skeletal maturity. There had been seldom reports of this lesion mimicking exostoses clinically. More encountered in the maxilla, mandible the tibia, fibula, radius, ulna, and hummers follow accordingly.[3-5]
This case report brings forth the unusual presentation of osteofibrous dysplasia of the tibia mimicking exostoses clinically which was successfully treated by surgical excision and curettage without bone grafting or internal fixation.
Case Report
A 13-year-old boy presented to us with a 2-year history of swelling in his right leg. History of trauma while playing was present 2 years ago. Initially, he noticed a small bony swelling which gradually increased in size over the years. Local examination revealed a nontender, hard swelling not fixed to overlying skin. Radiographs revealed a large area of irregular cortical thickening along the anterior, lateral, and posterior aspect of mid tibial diaphysis on the right side [Figure 1]. Corticomedullary differentiation was not lost, and the lesion borders were well-marginated without transition zone [Figure 2]. No periosteal reaction was observed. The lesion was completely excised [Figures 3 and 4], and the diagnosis was made by subsequent histological examination of the excised lesion and immunohistochemistry. Both revealed osteofibrous dysplasia. The patient was treated with above knee cast and advised nonweight bearing for 3 months. Follow-up at 1 year revealed no recurrence [Figure 5], and the patient returned to full-time activities.
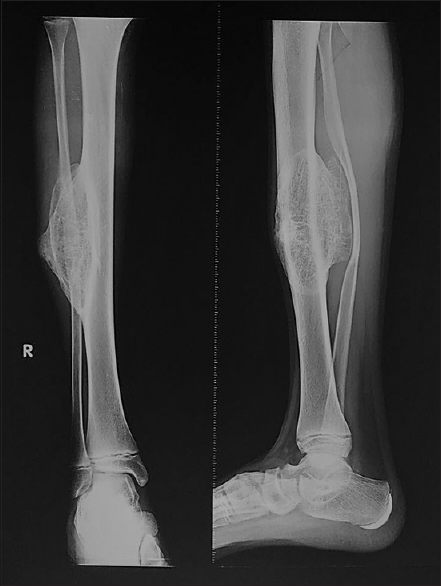
- Preoperative X-ray
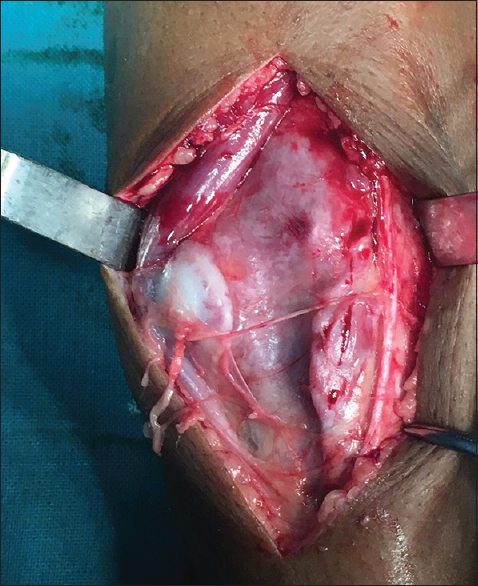
- Picture after dissection

- Post excisional mass
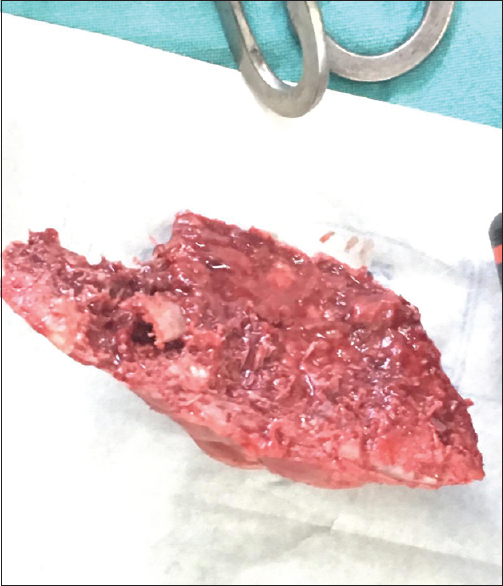
- Excised mass

- Postoperative X-ray
Discussion
The most frequent radiographic picture of osteofibrous dysplasia is a well-defined eccentric intracortical lytic lesion without any associated periosteal reaction or soft-tissue expansion.[2,5] Overlying cortex may be expanded and thinned out with associated pathological bowing and/or pathological fracture of the involved bone [Figure 6]. The lesion is well-defined by a zone of sclerosis. In our case, a sessile lesion with a cap with no periosteal reaction of the tibia with ill-defined cortical outline at places was present. Histologically, it shows loose fibrous stroma containing spicules of woven bony trabeculae that are lined by osteoblasts with zonal architecture.
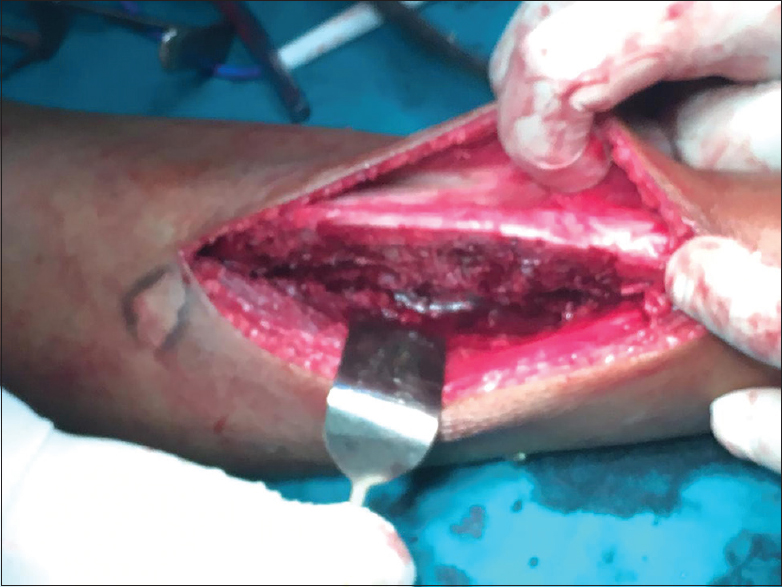
- Remaining tibial shaft post excision
Conclusion
Osteofibrous dysplasia can present in an uncommon location like the tibia. It can clinically mimic exostosis. Radiologically, it may be difficult to rule out other differential diagnoses of tibial enlargement [Figure 1], especially with preceding trauma history. Histopathology is inevitable for clinching the diagnoses.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Ossifying fibroma of the long bones. A light and electron microscopic study. Arch Pathol. 1966;82:218-33.
- [Google Scholar]
- Osteofibrous dysplasia of long bones a new clinical entity. Ital J Orthop Traumatol. 1976;2:221-37.
- [Google Scholar]
- Aclinicopathological and immunohistochemical study of osteofibrous dysplasia, differentiated adamantinoma, and adamantinoma of long bones. Skeletal Radiol. 1992;21:493-502.
- [CrossRef] [Google Scholar]
- Treatment outcome of osteofibrous dysplasia. J Pediatr Orthop B. 1998;7:199-202.
- [CrossRef] [PubMed] [Google Scholar]
- Osteofibrous dysplasia (ossifying fibroma of long bones). A report of four cases and review of the literature. Clin Orthop Relat Res. 1992;248:235-43.
- [CrossRef] [Google Scholar]




