
Translate this page into:
Observational study of management of stenosing tenosynovitis at wrist
Address for correspondence: Dr. Parag Manoj Tank, Department of Orthopedics, Smt Nathiba Hargovandas Lakhmichand Municipal Medical College, Ellise Bridge, Paldi, Ahmedabad 380006, Gujarat, India. E-mail: pmtank1211@yahoo.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Upadhyay KA, Tank PM, Patel HN, Damor HN, Katara DL. Observational study of management of stenosing tenosynovitis at wrist. J Orthop Spine 2023;11:8-13.
Abstract
BACKGROUND:
De Quervain’s tenosynovitis is a common painful inflammation of the tendons of the wrist. It affects the tendon of the first dorsal compartment, abductor pollicis longus, and extensor pollicis brevis. Symptoms are generated mainly due to excessive wrist movement causing friction of the synovial sheath.
MATERIALS AND METHOD:
The study included a total of 90 patients in the outpatient department of orthopedic division of the institute. Various modalities of conservative management like ultrasound therapy, laser therapy, and local steroids injection along with surgical management have been studied.
RESULT & CONCLUSION:
The study concluded that the conservative treatment is as effective as the surgical management, but the surgical management is the ultimate choice when other conservative modalities fail.
Keywords
De Quervain tenosynovitis
laser
local steroid injection
surgical release
ultrasound

Introduction
De Quervain (DQ) tenosynovitis involves tendon entrapment affecting the first dorsal compartment of the wrist. “Tenosynovitis” in DQ states the presence of an inflammation.[1] Studies have shown that the prevalence of DQ is high in the subjects 30–55 years of age and the frequency of tenosynovitis is higher in women compared to men in middle aged population.[2] Myxoid degeneration into the fibrous tissue deposits along with the increased vascularity causes hypertrophy of the dorsum retinacula.[3] Tendons in the narrowed canal stimulate the nociceptors and hence there is pain resulting in the impairment of wrist, hand, and thumb movements and functions with activities such as pulling, lifting, and gripping.[4] Finkelstein test was performed in the patients having pain and swelling at the outer aspect of the wrist while gripping any object with first and second finger.[5] Although the diagnosis for DQ is clinically done, plain radiographs help in differentiating other conditions related to radial wrist pain such as thumb carpo-metacarpal joint osteoarthritis.[1,4] Nonsurgical treatment modality included ultrasound therapy, laser therapy and local injection of steroid. Other than these routine nonsurgical modalities such as ultrasound, laser, and local steroid injection, there has also been the use of various hand therapies and orthosis for the same.[6] Surgical modality included the release of the tendon sheath. Because some patients prefer conservative treatment options rather than surgical release and each of these treatment modalities has its advantages and disadvantages, we carried out this study to compare the outcome of these four treatment methods.
Materials and Methods
In the study, we included total 90 patients with 71 women and 19 men after taking their written consents from May 2019 to January 2022 with 6-month follow-up. The study was conducted after obtaining ethical permission from institutional review board. All the patients were presented with clinical signs and symptoms of De Quervain’s disease which includes tenderness over radial styloid, positive Finkelstein’s test. The diagnosis was confirmed with ultrasound by a radiologist. X-rays were done to rule out any other bony pathology. We have recorded visual analogue scale (VAS) and Disability of Arm, Shoulder, and Hand Score (DASH) score before treatment and after treatment at the end of the final follow-up. All routine hematological investigations were done in all the patients. We treated 32 patients with local ultra sound therapy, 25 patients with local steroid injection, 14 patients with laser therapy, and 19 patients with surgical release. Patients with no prior history of any treatment for De Quervain’s tenosynovitis (operative or nonoperative) for at least 3 months were included in the study. Written informed consent for participation in the study was obtained from all patients. We included all adult patients with VAS score 5 or above along with positive Finkelstein test. Patients with previous history of trauma or had received any treatment recently for the same and patients with metabolic or autoimmune diseases were also excluded. The physical signs recorded for all groups were Finkelstein’s test and its response in VAS score, site of tenderness or nodule over radial styloid (size in mm), and soft tissue tenderness grading DASH score. Patients who were clinically diagnoses with De Quervain’s tenosynovitis attended the Orthopedics Out Patient Department, were included in the study. The dominant/nondominant extremity was recorded. A physiotherapist performed ultrasound procedure using frequency of 3 MHz for 6 min in each sitting. A total of 10 sittings of ultrasound treatment for 6 min were given to the patients. If patients had relapse of symptoms or not satisfied with one cycle of 10 sittings, such patients were given 2nd cycle of ultrasound treatment for 10 sittings after 1 month. In each sitting, total two cycles of laser were conducted. 10 sittings of laser treatment for 6 min were given to the patients. If patient had relapse of symptoms or not satisfied with one cycle of 10 sittings, those patients were given 2nd cycle of laser treatment for 10 sittings after 1 month. Injection Triamcinolone acetate 10 mg in 1 mL used with 1 mL of lidocaine local anesthesia for steroid injection treatment. Injection was given locally with complete aseptic precautions inside the sheath of 1st dorsal extensor compartment of affected wrist.
All the surgical release procedures were done under local anesthesia. 1.5–2.0 cm long superficial incision was taken longitudinally over the styloid process of radius avoiding damage to the radial sensory branch. First compartment tendons were isolated. Identifying the extensor polices brevis tendon, the rest of the sheath of dorsal retinaculum covering the tendon was dissected perpendicular to it. Septum between the extensor pollicis brevis (EPB) and abductor pollicis longus (APL) tendons were incised longitudinally. Any entrapments, which were inspected by plucking and lifting the tendon and smooth gliding of the tendons, were checked. Whenever any septum was encountered between the extensor polices brevis and adductor polices longus, they were addressed separately. Skin closure was done after proper saline wash and sterile dressing was applied.
Results
In the study, 29 patients (32.22%) were of 18–30 years of age group, 25 patients (27.77%) were of 31–40 years of age, and 23 patients (25.55%) were of 41–50 years of age. Remaining eight patients (8.88%) were of 50–60 years age and 5 patients (5.55%) were from more than 60 years of age [Figure 1]. Among them, 71 patients (78.89%) were women. Dominant hand involvement was seen in 62 patients (68.89%).
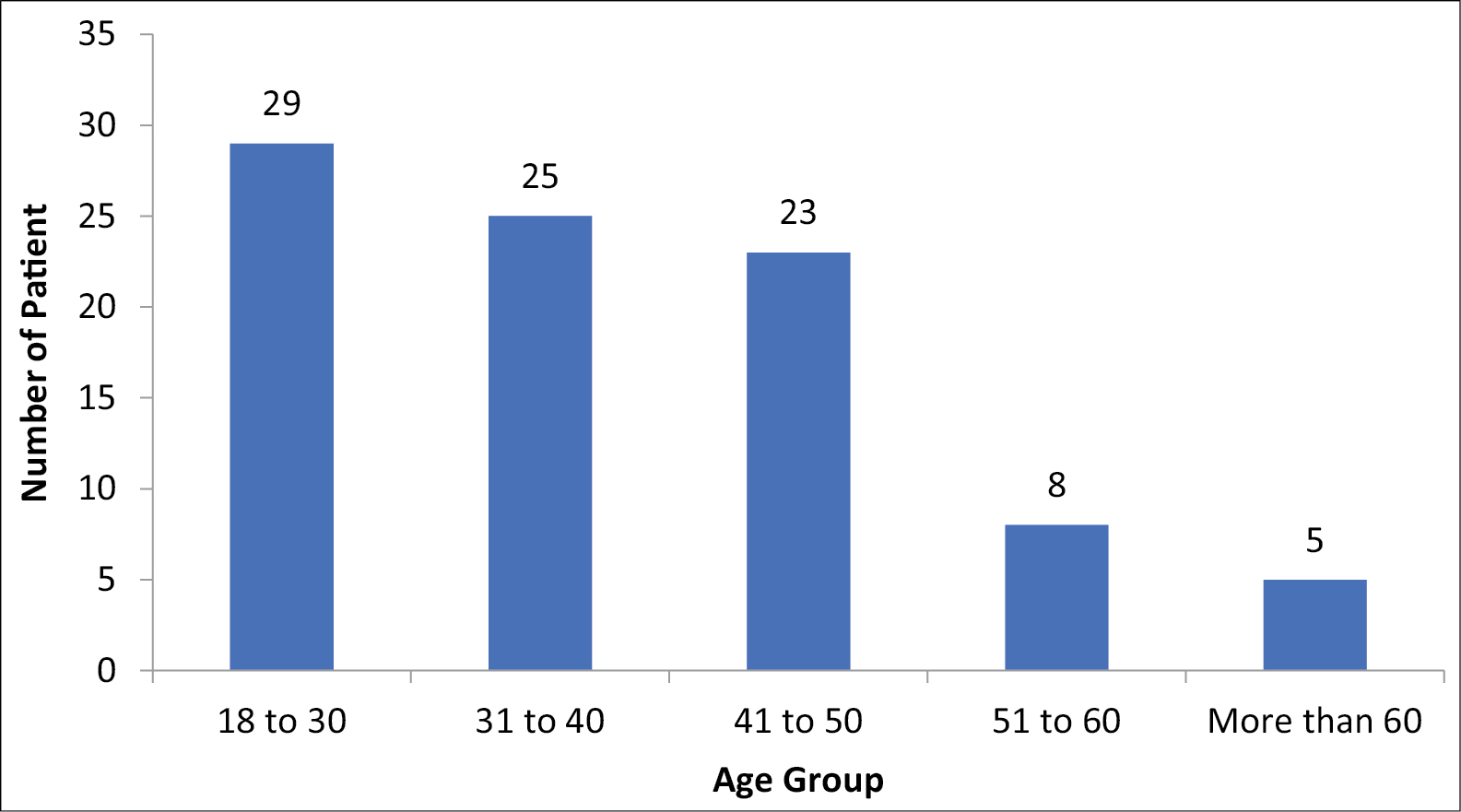
- Age distribution
Among the patient, 53 (58.89%) were right-dexterity and 37 patients (41.11%) are left-handed. In the modality of treatment 32 patients (35.56%) were given ultra sound therapy, 14 patients (15.55%) were given laser therapy, 25 patients (27.78%) were treated with steroid injection, and the remaining 19 patients (21.11%) were treated with surgical release [Table 1].
| Method of treatment | Number of patients |
|---|---|
| Ultra sound therapy | 32 |
| Injection steroid | 25 |
| Laser therapy | 14 |
| Surgical release | 19 |
| Total | 90 |
Patients were scheduled follow-up posttreatment after 2 weeks, 6 weeks, 10 weeks and then after 6 months. Initiation of pain relief was achieved in steroid injection therapy within 7–25 days, for ultrasound/laser therapy it varies in between 5 and 15 days, surgical release benefitted within 7–15 days. Results were evaluated by VAS score and DASH score comparing it at the time of treatment started and last follow-up visit at 6 months.
The change in VAS score from pretreatment to posttreatment was reduction from (mean ± SD) 6.53 ± 0.67 to 1.06 ± 0.80 with mean difference of 5.46 ± 1.01 for ultrasound therapy, from 6.57 ± 0.77 to 1.5 ± 1.28 with mean difference of 5.07 ± 1.43 for laser therapy, from 6.52 ± 0.77 to 0.92 ± 0.81 with mean difference of 5.60 ± 1.25 for steroid injection, and 6.78 ± 0.63 to 0.36 ± 0.49 with mean difference of 6.42 ± 0.60 for surgical release [Table 2]. Paired t test P value in the VAS score change was <0.0001 for all the treatment modality which means that all the treatment modalities were effectively treating the patients [Table 2]. Analysis of variance test concluded that surgical release has significantly better outcome for VAS score in compare with laser therapy or ultrasound therapy.
| Method of treatment (n) | VAS score (mean ± SD) | Paired t test P value | Mean difference | ANOVA test | |
|---|---|---|---|---|---|
| Pre treatment | Post treatment | ||||
| Ultra sound therapy (32) | 6.53 ± 0.67 | 1.06 ± 0.80* | <0.0001 | 5.46 ± 1.01# | P < 0.5 (vs SR) |
| Injection steroid (25) | 6.52 ± 0.77 | 0.92 ± 0.81* | <0.0001 | 5.60 ± 1.25 | P > 0.5 |
| Laser therapy (14) | 6.57 ± 0.75 | 1.5 ± 1.28* | <0.0001 | 5.07 ± 1.43## | P < 0.01 (vs SR) |
| Surgical release (19) | 6.78 ± 0.63 | 0.36 ± 0.49* | <0.0001 | 6.42 ± 0.60 | P > 0.5 |
* Paired t test was applied between pretreatment and post-treatment score and * P < 0.0001 was considered significant #ANOVA test was applied to compare different modalities of management of De Quervains and P < 0.5 was considered significant
From pretreatment to posttreatment, DASH score has been reduced from 65.15 ± 6.65 to 2.34 ± 4.91 with mean difference of 62.81 ± 7.92 for ultrasound therapy, 67.85 ± 7.52 to 5.71 ± 7.55 with mean difference of 62.14 ± 8.01 for laser therapy, from 64.72 ± 9.07 to 1.8 ± 4.05 with mean difference of 62.92 ± 9.99 for steroid injection, from 68.94 ± 5.15 to 0 with mean difference of 68.94 ± 5.15 for surgical release [Table 3]. Paired t test was applied between pretreatment and posttreatment DASH score and a P value of <0.0001 was considered significant and all the treatments had significant changes in DASH score after the treatment suggesting their effectiveness. ANOVA test was applied to compare different methods of treatment, and a P value of <0.5 was considered significant and showed no significant difference for DASH score for different modality of treatment [Table 3].
| Method of treatment (n) | DASH score (mean ± SD) | P value | Mean difference | ANOVA test | |
|---|---|---|---|---|---|
| Pre treatment | Post treatment | ||||
| Ultra sound therapy (32) | 65.15 ± 6.65 | 2.34 ± 4.91* | <0.0001 | 62.81 ± 792 | >0.5 |
| Injection steroid (25) | 64.72 ± 9.07 | 1.8 ± 4.05* | <0.0001 | 62.92 ± 9.99 | >0.5 |
| Laser therapy | 6785 ± 752 | 5.71 ± 755* | <0.0001 | 62.14 ± 8.01 | >0.5 |
| Surgical release | 68.94 ± 5.15 | 0* | <0.0001 | 68.94 ± 5.15 | >0.5 |
* Paired t test was applied between pretreatment and post-treatment score and * P < 0.0001 was considered significant #ANOVA test was applied to compare different modalities of management of De Quervains and P < 0.5 was considered significant
For gender-specific change in VAS score, for men patients’ VAS score changed from (pretreatment to posttreatment) 6.73 ± 0.73 to 0.78 ± 0.71 with mean difference of 5.94 ± 1.07 and for women patients VAS score changed from (pretreatment to post treatment) 6.54 ± 0.69 to 0.98 ± 0.94 with mean difference of 5.56 ± 1.18. Paired t test was applied between pretreatment and post-treatment score and P < 0.0001 was considered significant. Unpaired test was applied and P value was 0.2034, Hence no significant difference between male and female. For gender specific change in DASH score, for men patients DASH score changed from (pretreatment to posttreatment) 67.89 ± 7.69 to 0.78 ± 3.44 with mean difference of 67.10 ± 7.69 and for women patients it changed from 65.84 ± 7.33 to 2.68 ± 5.25 with mean difference of 63.21 ± 8.41. Paired t test was applied between pretreatment and posttreatment score and a P value of <0.0001 was considered significant. Unpaired test was applied and P value was 0.0717. Hence no significant difference between both genders was observed.
For dominant hand, VAS score changes from pretreatment to post treatment were as follow. For ultrasound therapy from 6.62 to 1.14, for laser therapy from 6.54 to 1.45, steroid injection from 6.47 to 0.89 and for surgical release 6.90 to 0.36. While for non-dominant hand, VAS score changes from pretreatment to posttreatment are as follows: for ultrasound therapy from 6.36 to 0.90, for laser therapy from 6.66 to 1.66, for steroid injection 6.66 to 1, and for surgical release from 6.64 to 0.64. Final outcome with VAS score for dominant hand was 6.61 ± 0.75 pretreatment to 0.98 ± 0.89 posttreatment with mean difference of 5.62 ± 1.16 and for non-dominant hand was 6.53 ± 0.57 pretreatment to 0.85 ± 0.93 posttreatment with mean difference of 5.67 ± 1.18. Paired t test was applied between pretreatment and post-treatment score and a P value of <0.0001 was considered significant. Unpaired test was applied and P value was 0.8530. Hence no significant difference between dominant hand and non-dominant hand was observed. For dominant hand, DASH score changes from pretreatment to post treatment are as follow: for ultrasound therapy from 64.76 to 2.85, for laser therapy from 66.36 to 5.45, for steroid injection 63.31 to 1.58, and for surgical release 70.45 to 1.43. While for non-dominant hand, DASH score changes from pretreatment to post treatment are as follows: for ultrasound therapy from 65.90 to 1.36, for laser therapy from 73.33 to 6.66, for steroid injection from 69.16 to 2.5, for surgical release from 67.85 to 1.07. Final outcome with DASH score for dominant hand was 65.61 ± 7.71 pretreatment to 2.41 ± 5.18 posttreatment with mean difference of 63.19 ± 8.63 and for non-dominant hand 67.67 ± 6.45 to 1.78 ± 4.34 with mean difference of 65.89 ± 7.58. Paired t test was applied between pretreatment and post-treatment score and a P value <0.0001 was considered significant. Unpaired test was applied and P value was 0.1582, hence no significant difference between either dexterity.
Successful outcome was defined as an absence of pain, tenderness in the limitation of movement of thumb due to the pain, both subjectively and objectively at the end of 6 months. There were five failures out of 32 in ultrasound therapy, five failures out of 14 in laser therapy, three out of 25 in steroid injection therapy and no failure out of 19 patients treated with surgical release. Treatment success rate was 84% (27/32) for ultrasound therapy, 64% (9/14) for laser therapy, 88% (22/25) for steroid injection, and 100% (19/19) for surgical release [Table 4].
| Outcome of the treatment therapy | Therapy assigned | |||||
|---|---|---|---|---|---|---|
| Post Rx DASH | Ultrasound therapy | Laser therapy | Steroid injection | Surgical release | Number of the patients treated | |
| Number of the patients treated | 32 | 14 | 25 | 19 | 90 | |
| Excellent | 0–5 | 27 | 9 | 22 | 19 | 77 |
| Good | 6–14 | 2 | 1 | 2 | 0 | 5 |
| Satisfactory | 15–35 | 3 | 4 | 1 | 0 | 8 |
| Poor | >35 | 0 | 0 | 0 | 0 | 0 |
Discussion
With the upgradation in technology and time, there has been an evolution in the treatment and diagnosis of De Quervain’s disease. Initially, there were two options either conservative management with NSAIDS and immobilizing splint or surgical release. Introduction of steroid injection at local site was introduced as a treatment option after its availability in 1950.[6] De Quervain’s disease prevalence varies from minimal physical worker to heavy manual laborer. First dorsal compartment of wrist comprises two tendons, APL and EPB and these are responsible for the abduction of thumb and extension of metacarpophalangeal joint of thumb, respectively.
In De Quervain’s disease gliding of APL and EPB is restricted creating symptoms such as pain, tenderness, mild swelling over base of the thumb, and painful movement of thumb. While muscle is being contracted, the tendons transmit mechanical loads. When the movement becomes repetitive and greater than the ability of the tendons to bear with, it results in synovial inflammation, repair, and fibrotic changes.[7] The present study studied 90 patients with different modalities of treatment including ultrasound therapy, laser therapy, local steroid injection, and surgical release. Also, we found that occupation has not been the main factor to influence symptoms. The participants in the study were ranging from sales representative and shop keepers to manual laborer and lathe machine worker, as well as in housewives. The study supports the previous finding of prevalence that suggested that women were more affected than men. The present study also concluded that the dominant hand is more involved over nondominant hand. Local synthetic long-acting steroids are cost effective, less cumbersome, and easy to repeat therapy for patients and clinicians.[2] Study by Finkelsteins et al.[5] and Lapidus et al.[8] reported cure rate by surgical release to be 92% and 91%, respectively. The present study had a cure rate of 100%, without any complications or recurrence of the symptoms. Lapidus et al.[8] recommended the use of steroid injection was still the important modality of treatment, with surgery being reserved for refractory cases. In our study steroids and local anesthetic injection had given an 80% cure rate. A study suggested a single use of steroid injection in de Quervain disease patients gave satisfactory results in about 70% patients and further 10% patients were cured by the successive steroid injection which is time saving and cost-effective compared to surgical intervention.[9] Study by Sharma et al.[10] concluded that ultrasound therapy and laser therapy, both improved the symptoms, ultrasound was marginally better than laser therapy and found a decrease in the tendon sheath diameter and pain posttreatment. The present study found same outcome when compared between ultrasound therapy and laser therapy as 84% success rate in ultrasound therapy compare to 64% success rate in laser therapy.
A study has recommended the use of longitudinal incisions over the transverse incision in term of complications such as superficial neurovascular damage and scar in surgical decompression of the tendons in de Quervain disease patients.[11] In the present study, longitudinal incisions were used during surgical intervention. Schellar et al.[12] presented long-term results after the decompression of first dorsal compartment both tendons as well as partial release of extensor ligaments. They found excellent result outcome and no complications such as tendon subluxation. Graham et al.[13] found steroid injection superior to medication and splinting when given at the correct site and technique. A study found two-point injection, one at the tender induration and another along the parts of APL and EPB tendon superior over the one-point injection technique.[14] However, in our study, we found satisfactory results following one-point injection technique. Limited surgical release for EPB tendon sheath from the extensor retinaculum found satisfactory results in the patients with septum. They decompressed both the tendon sheath for patients without septum.[15] In our study we decompressed both the tendon irrespective of septum is present or not. Lee et al.[16] found excellent results with surgical release of first dorsal compartment sheath without any subluxation or instability of the tendons as they did not excise the tendon sheath completely. In our study, patients went through the surgical release did not have any complications as well. A study by White et al.[17] presented a case of reconstruction of the tendon sheath with extensor retinaculum in the patient with subluxation of APL and EPB tendons due to their complete sheath release. They suggested complete excision of all intra-compartmental septa and recommended incision of the sheath over the EPB at its dorsal margin, which will prevent any tendon subluxation. Wrist X-rays of our patients did not show any thickening of radial styloid, spur formation, osteopenia, erosion, or any bulging. These findings are consistent with Akdag et al.[18] study, in which they found a variable incidence of abnormal radiographic findings on radial styloid in patients with de Quervain’s tenosynovitis and asymptomatic individuals.
Conclusion
De Quervain wrist tenosynovitis is one of the most debilitating conditions, when diagnosed and treated early can bring satisfactory functional outcomes. De Quervain disease occurs more common in women. This condition should always be suspected in the patients with long standing tenderness over the styloid process of radius bone. Effectiveness of the conservative therapies such as laser therapy and ultrasound therapy along with the local steroid injection procedure is equivalent to the surgical release treatment and it is also cost effective and time saving. Conservative treatment nullifies the complication of the superficial radial nerve damage and entrapment of the extensor tendons. But surgical release treatment brings the ultimate outcomes and should be kept reserved for the refractory or recurrent cases of the de Quervain disease.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- The histopathology of de Quervain’s disease. J Hand Surg Br. 1998;23:732-4.
- [CrossRef] [Google Scholar]
- A patient with de Quervain’s tenosynovitis: A case report using an Australian approach to manual therapy. Phys Ther. 1994;74:314-26.
- [CrossRef] [PubMed] [Google Scholar]
- Nonsurgical treatment of De Quervain tenosynovitis: A prospective randomized trial. Hand. 2020;15:215-9.
- [CrossRef] [PubMed] [Google Scholar]
- Common soft tissue musculoskeletal pain disorders. Prim Care. 2018;45:289-303.
- [CrossRef] [PubMed] [Google Scholar]
- Finkelstein’s test: A descriptive error that can produce a false positive. J Hand Surg. 1992;17:481-2.
- [CrossRef] [Google Scholar]
- Hand therapy versus corticosteroid injections in the treatment of de Quervain’s disease: A systematic review and meta-analysis. J Hand Ther. 2016;29:3-11.
- [CrossRef] [PubMed] [Google Scholar]
- MRI of the extensor tendons of the wrist. Am J Roentgenol. 2017;209:1093-102.
- [CrossRef] [PubMed] [Google Scholar]
- Stenosing tenovaginitis of the wrist and fingers. Clin Orthop Relat Res. 1972;83:87-90.
- [CrossRef] [PubMed] [Google Scholar]
- De Quervain’s disease: Surgical or nonsurgical treatment. J Hand Surg. 1990;15:83-7.
- [CrossRef] [PubMed] [Google Scholar]
- Outcome of low level lasers versus ultrasonic therapy in de Quervain’s tenosynovitis. Indian J Orthop. 2015;49:542-8.
- [CrossRef] [PubMed] [Google Scholar]
- De qeurvian tenosynovitis: Clinical outcomes of surgical treatment with longitudinal and transverse incision. Oman Med J. 2011;26:91-3.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term results of surgical release of de Quervain’s stenosing tenosynovitis. Int Orthop. 2009;33:1301-3.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical inquiries. Are steroid injections effective for tenosynovitis of the hand? J Fam Pract. 2007;56:1045-7.
- [Google Scholar]
- De Quervain’s disease: Efficacy of intra-sheath triamcinolone injection. Int Orthop. 2007;31:265-8.
- [CrossRef] [PubMed] [Google Scholar]
- Limited surgical treatment of de Quervain’s disease: Decompression of only the extensor pollicis brevis subcompartment. J Hand Surg. 1998;23:840-3.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical release of the first extensor compartment for refractory de Quervain’s tenosynovitis: Surgical findings and functional evaluation using DASH scores. Clin Orthop Surg. 2014;6:405-9.
- [CrossRef] [PubMed] [Google Scholar]
- Symptomatic palmar tendon subluxation after surgical release for de Quervain’s disease: A case report. J Hand Surg. 1984;9:704-6.
- [CrossRef] [PubMed] [Google Scholar]
- De quervain’s tenosynovitis and radial styloid osseous changes. Indian J Orthop. 2021;29:1-6.
- [Google Scholar]




