
Translate this page into:
Obesity and osteoarthritis of the knee joint: Is leptin the missing link?
Address for correspondence: Dr. Obinna Henry Obiegbu, Department of Orthopaedic Surgery, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria. E-mail: obinnaobiegbu@yahoo.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Obiegbu OH, Nnakenyi ID, Ndukwu CU. Obesity and osteoarthritis of the knee joint: Is leptin the missing link? J Orthop Spine 2019;7:57-61.
Abstract
BACKGROUND:
Osteoarthritis (OA) involves a progressive degeneration of the articular cartilage, remodeling of the subchondral bone, and synovitis. It typically affects diarthrodial (synovial) joints including the knee joints. Obesity, which represents a body mass index (BMI) of ≥30, has been linked to OA of the knee joint. A biomechanical theory which infers that repetitive application of axial loading at the knee joint is the mechanism through which obesity causes OA has long been put forward. However, metabolic factors (adipokines) may yet be a link between OA and obesity.
AIM AND OBJECTIVES:
This study was performed to establish if there is a correlation between serum leptin and radiological severity of OA of the knee joint in obese individuals.
MATERIALS AND METHODS:
This was a prospective study carried out after ethical clearance was obtained from the hospital's ethical committee. Written informed consent was obtained from all prospectively recruited participants. Patients who met the inclusion criteria were selected by random sampling into either the obese or nonobese group based on their BMI. The patients were radiographically evaluated, and data were collected using a well-designed and structured pro forma. 5 ml of blood was collected from each patient for the analysis of serum leptin level.
RESULTS:
A total of 100 patients were included into this study. Fifty of these patients were obese (BMI ≥30), whereas the other fifty were nonobese (BMI <30). The peak age of the occurrence of knee OA was 61–70 years. The mean serum leptin level in obese patients was 20.11 ng/ml, as opposed to that in nonobese patients of 4.88 ng/ml. The radiological severity was analyzed, and there was a positive correlation between serum leptin level and radiological severity in OA of the knee joint. A higher percentage of females in this study were obese (71%) as opposed to males (29%), and females had statistically significantly higher leptin levels when compared to males.
CONCLUSION AND RECOMMENDATION:
From the results of this study, it is concluded that there is a correlation between serum leptin levels and radiological severity of OA of the knee joint in obese patients.
Keywords
Body mass index
osteoarthritis
serum leptin

Introduction
Osteoarthritis (OA), a clinical classification for a combination of pathological conditions involving progressive degeneration of articular cartilage, remodeling of subchondral bone, and synovitis (usually limited to the affected joint), commonly affects the knee joint.[1] OA of the knee has been demonstrated to be a complex process that includes multiple changes in the joint components such as cells, matrix, and molecular production. However, despite its prevalence throughout history, the etiology is yet to be fully understood. OA is a multifactorial disease with both genetic and environmental determinants.[2,3] Obesity has been linked to OA, but is most strongly linked to the knee joint.[3] Although some studies have found a cross-sectional association between obesity and OA of the knee joint (including a four-fold increase in radiographic OA of the knee joint in obese women),[3,4] how obesity causes OA of the knee joint has been of considerable debate.
Two major theories have been proposed to explain the association: biomechanical and metabolic theories. The biomechanical theory infers that obesity leads to repetitive application of increased axial loading of the knee with consequent degeneration of the articular cartilage and sclerosis of the subchondral bone.[5] However, the association between obesity and OA in nonweight-bearing joints such as those of the hands/or wrist suggests that other factors may yet play a role. The metabolic theory infers that there is a role for adipokines, especially leptin which has received major attention because of its correlation to body size. Leptin is a glycosylated peptide hormone encoded by the obese gene (ob), and is mainly produced by the adipocytes.[6] Leptin may produce pro-inflammatory and catabolic effects on the cartilage through induction of matrix metalloproteinases and nitric oxide and production of pro-inflammatory cytokines.[7] These factors can lead to articular cartilage damage.
The most common method of radiographic classification of knee OA is the Kellgren–Lawrence (K–L) radiographic grading scheme and Atlas which has been used for more than four decades.[8] It grades OA into the following five levels (from 0 to 4):
Grade 0 – No abnormality
Grade 1 – Incipient OA, beginning of osteophyte formation on eminences
Grade 2 – Moderate joint space narrowing, moderate subchondral bone sclerosis
Grade 3 – >50% joint space narrowing, rounded femoral condyle, extensive subchondral sclerosis, and extensive osteophyte formation
Grade 4 – Joint destruction, obliterated joint space, subchondral cysts, and subluxation of the joint.
The objective of this study was to determine if there is a correlation between serum leptin levels and radiological severity of OA of the knee joint in obese patients.
Materials and Methods
This was a prospective study involving 100 patients with OA of the knee joint attending the outpatient department of Nnamdi Azikiwe University Teaching Hospital, Nnewi, Nigeria, between July 2016 and June 2017. Fifty of these patients were obese (body mass index [BMI] ≥30) and the other fifty were nonobese (BMI ≤30).
Approval was sought and obtained from the Nnamdi Azikiwe University Teaching Hospital (on the December 03, 2015, with protocol number: NAUTH/CS/66/VOL. 8/34).
Inclusion criteria were patients diagnosed with OA of the knee joint who voluntarily gave their consent for the study. Patients who had prior surgery, or who had grade 0/1 radiologic knee OA (—K–L), or who refused to give consent were excluded from the study. Grades 2, 3, and 4 were classified as mild, moderate, and severe knee OA, respectively.
The sample size was calculated based on the statistical formula (Daniel, 1999)[9] as shown below:
n = Z2 P (1 −P)/d2
where n = sample size,
Z = Statistic for level of confidence; at 95% level of confidence which is conventional, Z value is 1.96,
P = Expected prevalence or proportion. Value of 7% was chosen for this study,[10]
d = Absolute precision, i.e., the value required (in percentage points) which in actual term describes the maximum difference between the population rate and the sample rate that can be tolerated. 5% (0.05) was taken for this study.
Therefore,
n = (1.96)2 0.07 (1 − 0.07)/(0.05)2
=100.03, which is approximately 100.
Therefore, 100 patients were recruited for this study.
Serum leptin assay
Test samples – 5 ml of blood was obtained from all the 100 patients.
An in-vitro sandwich enzyme-linked immunosorbent assay (ELISA) technique was employed for the quantitative measurement of human leptin in serum. The micro-titer wells were coated with a monoclonal anti-leptin antibody. The test samples were added into the coated wells with the specific leptin antibody.
After this, the unbound material was washed off, and the enzyme substrate was added for the detection of bound leptin. The intensity of the color developed was proportional to the concentration of leptin in the sample.
Diagnostic Automation Leptin Human in vitro ELISA kit AccuDiag Leptin ELISA kit (Diagnostic Automation/ Cortez Diagnostics, Inc., Calabasas, California, USA). was utilized for this study.
Radiological grading
All patients had X-rays done on the affected knee, and classification of the severity was done using the —K–L classification system.
Results
A total of 100 patients (fifty each in the obese and nonobese groups) were recruited into this study and analyzed. The age range was from 45 to 79 years, with a mean age of 59 ± 7.2 years.
Table 1 shows that the most commonly affected age group was 51–60 years.
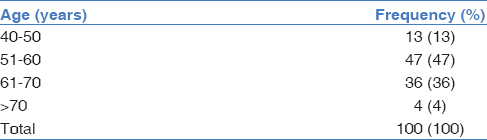
Figure 1 shows a female preponderance with a female-to-male ratio of 2.4:1.
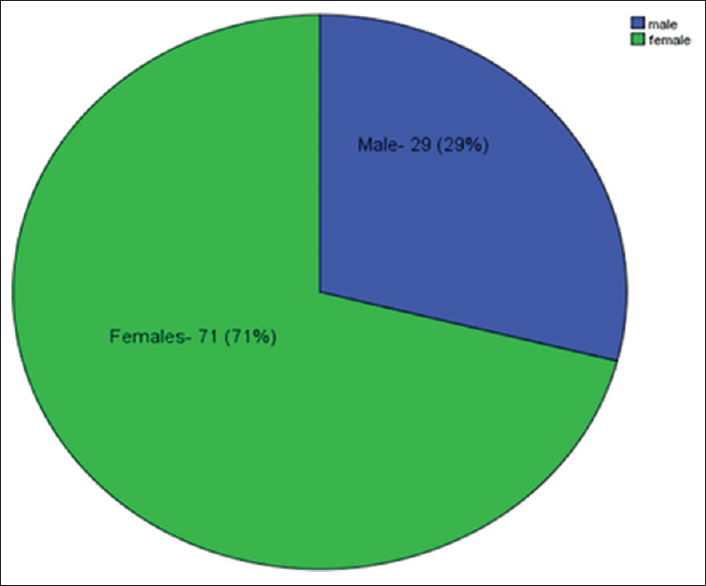
- Sex distribution of the patients
Table 2 shows no statistically significant difference among the age groups of the obese and nonobese groups.

Table 3 shows that the serum leptin levels were significantly higher in the obese patients, and thus there is a positive correlation between serum leptin and BMI (U = 142.00, P < 0.001).
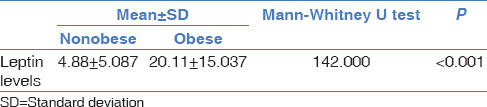
Table 4 shows the difference in mean leptin levels across the radiological severity groups in nonobese patients. This difference is weakly statistically significant.
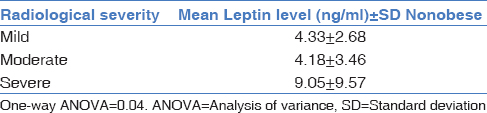
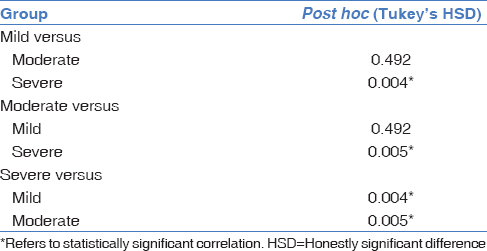
Table 5 shows the difference in mean leptin levels across the radiological severity groups in obese patients. This difference is statistically significant. Post hoc analysis was done to determine which subgroup had more correlation with serum leptin levels.
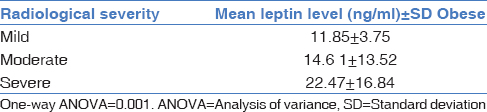
Table 6 shows that patients with severe radiological features had statistically significant higher leptin levels when compared to those with mild and moderate radiological features.
Discussion
This was a prospective study conducted to establish the role of serum leptin in obese patients with OA of the knee joint. It highlighted the correlation between serum leptin levels and obesity and also the correlation between serum leptin level and the radiological severity of OA of the knee joint.
OA of the knee joint was found to occur most commonly within the age range of 51–70 years, with a peak age of occurrence within the 50–60 years' age group. This is similar to the findings of Adebusoye et al.[11] and Ebong,[12] where the most commonly involved age bracket was also between 51 and 65 years. It also agrees with documentation in other literature that OA of the knee joint occurs commonly in females.[13] Similarly, the average age of patients with OA of the knee joint in this study was 59 ± 7.2 years; this agrees with the mean age of 52 years reported by Ebong [12] and also by Kaur et al.[13] in their series.
The current study found a female preponderance, with a female-to-male ratio of 2.4:1, which is within the ratio found by Ebong.[12] However, this was slightly different from the ratio of 3.5:1 found by Akinpelu et al.[13] and 4.95:1 reported by Ojoawo et al.[14] These differences are probably due to the influence of the population being studied on the distribution of OA of the knee joint.
The mean serum leptin level in nonobese patients in this study was 4.88 ± 5.09 ng/ml, whereas that in obese patients was 20.11 ± 15.04 ng/ml; this difference was statistically significant. This difference between the obese and nonobese groups agrees with the study done by Chow and Phoon [15] where overweight/obese individuals generally demonstrate higher circulating leptin concentration than healthy weight/nonobese individuals. This difference was also statistically significant. Similarly, it also agrees with the findings reported by Usman et al.[16] where the mean leptin level was 16.59 ± 13.56 ng/ml compared to that in the nonobese group of 5.58 ± 6.30 ng/ml. A statistically significant positive correlation between obesity and serum leptin level was also found in this study.
In this study, there was a positive correlation between serum leptin level and radiological severity as graded by the K–L classification system.[8] This is in agreement with a study done by Ellaban et al.[17] who found a highly significant correlation between serum leptin and the K–L score of the knee joint. It is also in agreement with the study done by Misra et al.[18] where a positive correlation was found between serum leptin and the severity of knee OA.
In contrast to these findings, in a study by Iwamoto et al.[19] done on postmenopausal Japanese women with OA of the knee joints, it was found that there is no significant correlation between the serum leptin concentration and the radiographic grade of knee OA. This may be due to the different management protocols and inclusion criteria, as most of their patients were receiving weekly to monthly intra-articular injections of hyaluronate.
Conclusion
OA of the knee joint is a common disorder, often characterized by pain, cartilage damage, and joint dysfunction. Although the mechanism of action of leptin in OA in obese patients is still unclear, its role cannot be ignored. This study showed a positive correlation between serum leptin and BMI and also between serum leptin and radiological severity of knee OA. A study by Jiang et al.[20] suggests that resveratrol may relieve OA pathology in obese patients by reducing systemic inflammation and/or inhibiting toll-like receptor 4 signaling in cartilage. It would be pertinent to note in further studies if drugs reducing serum leptin would lead to an alleviation of pathology in obese patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Mechanism of cartilage destruction in osteoarthritis. Nagoya J Med Sci. 2002;65:73-84.
- [Google Scholar]
- Osteoarthritis I: Epidemiological risk factors and historical considerations. Inflammopharmacology. 2002;10:5-21.
- [CrossRef] [Google Scholar]
- Osteoarthritis: New insights. Part 1: The disease and its risk factors. Ann Intern Med. 2000;133:635-46.
- [CrossRef] [Google Scholar]
- The association of obesity with osteoarthritis of the hand and knee in women: A twin study. J Rheumatol. 1996;23:1221-6.
- [Google Scholar]
- Secondary gait changes in patients with medial compartment knee osteoarthritis: Increased load at the ankle, knee, and hip during walking. Arthritis Rheum. 2005;52:2835-44.
- [CrossRef] [PubMed] [Google Scholar]
- Positional cloning of the mouse obese gene and its human homologue. Nature. 1994;372:425-32.
- [CrossRef] [PubMed] [Google Scholar]
- Adipocytokines: Mediators linking adipose tissue, inflammation and immunity. Nat Rev Immunol. 2006;6:772-83.
- [CrossRef] [PubMed] [Google Scholar]
- Atlas of standard radiographs. In: The Epidemiology of Chronic Rheumatism. Vol 2. Nnewi, Anambra State, Nigeria: Blackwell Scientific Publications; 1963.
- [Google Scholar]
- Biostatistics: A Foundation for Analysis in the Health Sciences (7th ed). New York: John Wiley Sons; 1999.
- Prevalence of symptomatic hip and knee osteoarthritis: A two-phase population-based survey. Osteoarthritis Cartilage. 2011;19:1314-22.
- [CrossRef] [PubMed] [Google Scholar]
- Magnitude of knee osteoarthritis and associated risk factors among adult patients presenting in a family practice in Nigeria. J Med Trop. 2013;15:144-50.
- [CrossRef] [Google Scholar]
- Osteoarthritis of the knee in Nigerians. Ann Rheum Dis. 1985;44:682-4.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of knee osteoarthritis and its determinants in 30-60 years old women of Gurdaspur, Punjab. Int J Med Sci Public Health. 2018;7:825-30.
- [CrossRef] [Google Scholar]
- Prevalence of symptoms of self-reported knee osteoarthritis in Odo-Ogbe community, Ile-Ife. Niger J Health Sci. 2016;16:4-10.
- [CrossRef] [Google Scholar]
- Measurement of serum leptin concentrations in university undergraduates by competitive ELISA reveals correlations with body mass index and sex. Adv Physiol Educ. 2003;27:70-7.
- [CrossRef] [PubMed] [Google Scholar]
- Effects of serum leptin on lung functions in obese and non-obese adults. Ann K Emu. 2018;24:751-5.
- [CrossRef] [Google Scholar]
- Impact of obesity on activity and severity parameters on osteoarthritis. Life Sci J. 2015;12:38-44.
- [Google Scholar]
- Serum leptin and risk of knee pain and osteoarthritis: Multicenter osteoarthritis study. Arthritis Rheum. 2015;67:189-91.
- [Google Scholar]
- Serum leptin concentration positively correlates with body weight and total fat mass in postmenopausal Japanese women with osteoarthritis of the knee. Arthritis. 2011;2011:580632.
- [CrossRef] [PubMed] [Google Scholar]
- Oral administration of resveratrol alleviates osteoarthritis pathology in C57BL/6J mice model induced by a high-fat diet. Mediators Inflamm. 2017;2017:7659023.
- [CrossRef] [PubMed] [Google Scholar]




