
Translate this page into:
Midterm results of cementless total hip arthroplasty in young
Address for correspondence: Dr. Abhijit Chandrakant Kawalkar, Department of Orthopaedics, Mahatma Gandhi Institute of Medical Sciences, Sewagram - 442 001, Wardha, Maharashtra, India. E-mail: dr.abhijitkawalkar@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Kawalkar AC, Badole CM, Phadke A. Midterm results of cementless total hip arthroplasty in young. J Orthop Allied Sci 2016;4:30-5.
Abstract
Introduction:
There are a variety of etiological factors that may result in arthritis of the hip in young adults. There are, therefore, not infrequent occasions when orthopedic surgeons may encounter very young patients with end-stage arthritis of the hip necessitating surgical intervention. In the past hip arthrodesis or resection arthroplasty were used to address end-stage arthritis of the hip in young patients but recently total hip arthroplasty emerged as the viable alternative to above surgical procedures. The high activity level, repetitive loading and excessive demand placed on the hip on one hand and issues of durability of the implant materials on the other lead to high failure rates of total hip arthroplasty in young patients in the past. The aim of this prospective study was to evaluate the clinical and radiographic results of these modern cementless THA in patients with end stage arthritis who were younger than 40 years of age.
Materials and Methods:
A prospective study was carried out in which 25 patients (28 hips) younger than 40 years with hip arthritis underwent primary cementless total hip arthroplasties participated. The Taperloc femoral component with Porous coated cementless acetabular cup and highly crossed linked polyethylene liner was used in all hips. The Harris hip score was used to determine functional outcome and activity level was evaluated by the classification of Johnston et al. Radiographic analysis consisted of antero-posterior views of the hip and pelvis, a true lateral view of the hip.
Observations and Results:
All 25 patients were available for both clinical and radiographic evaluation. 93% of patients had excellent to good; and none of the hips had poor clinical outcome. Radiographic assessment revealed consistent evidence of bony ingrowth. No femoral component was loose or required revision.
Conclusion:
Cementless total hip arthroplasty can be safely and successfully performed in young patients less than 40 years with excellent results in short to midterm follow-up.
Keywords
Cementless total hip arthroplasty
hip arthritis
young patients

Introduction
There are a variety of etiological factors that may result in arthritis of the hip in young adults. Avascular necrosis of the femoral head, post traumatic arthritis, ankylosing spodylosis and juvenile rheumatoid arthritis are few such conditions that may lead to disabling arthritis of the hip. The disability imposed by arthritis can compromise the activities of daily living of these young patients. There are, therefore, not infrequent occasions when orthopedic surgeons may encounter very young patients with end-stage arthritis of the hip necessitating surgical intervention. In the past hip arthrodesis or resection arthroplasty were used to address end-stage arthritis of the hip in young patients but recently total hip arthroplasty emerged as the viable alternative to above surgical procedures.[1]
Total hip arthroplasty (THA) is by no means a recent development, however the advances in the last 30 years have transformed total hip arthroplasty into possibly the most common and successful orthopedic surgical procedure. Part of the success of THA has been in the refinement of the surgical procedures and the part to the advances in implant materials and design. Total hip arthroplasty is the main treatment option for restoring function and mobility for various end-stage degenerative conditions of the hip joint.[2] Despite the fact that THA was initially designed to be performed in elderly low-demanding patients, the benefit of the procedure in younger populations has also been well-documented in resent past.
The high activity level, repetitive loading, and excessive demand placed on the hip on one hand and issues of durability of the implant materials on the other lead to high failure rates of total hip arthroplasty in young patients in the past.[3] Although compromised survivorship of THA in the young and very active patients cannot be disputed, improvements in the design of prosthesis and introduction of alternative bearing surfaces in recent years have lead to increasing number of total hip arthroplasty being performed in active and younger patients. But the outcome of this cementless modern generation THA for young patients is largely unknown.
The aim of this prospective study was to evaluate the clinical and radiographic results of these modern cementless THA in patients with end stage arthritis who were younger than 40 years of age.
Materials and Methods
A prospective study was carried out from January 2011 till December 2014 in 33 consecutive patients with 37 arthritic hips underwent primary cementless total hip arthroplasties. All surgeries were performed by a senior surgeon.
Inclusion criteria
Patient having either unilateral or bilateral hip arthritis
Skeletally mature patients less than 40 years
No medical contraindication for anesthesia.
Exclusion criteria
Skeletally immature patients and patients more than 40 years.
Dysplastic hip conditions (congenital)
Active infection at operative or other site
Septic arthritis
Tubercular arthritis
Neurological weakness of the limb.
The Taperloc femoral component was used in all hips in this series. The stem has a tapered rectangular shape designed to achieve fixation mediolaterally with the proximal femur. The implant is non-collared and proximal 40% of the implant is porous coated with a pressure plasma spray technique. The distal non-porous-coated portion of the stem has a satin surface finish [Figure 1] All of the femoral components were modular and had a 28-mm articulating head. The femoral component insertion for the taperloc component requires no endosteal reaming. Broaching achieves the solid cortical press fit. Mallory head radial cementless acetabular cup was used for all the patients in our study. It is hemispheric titanium alloy component with plasma spray coating. The peripheral flange has flair to provide the press fit. The plasma spray coating increases the outer diameter by 1 mm over the reamed the diameter, further enhancing stability. Also screws are used for further stability of cup. The cup liner is the cylindrical shell made of highly crossed linked polyethylene. It is available in standard, hi-wall and 10 degree options [Figure 2]. A floating titanium metal ring located in the shell's periphery securely locks into a groove around the outer periphery of the polyethylene liner when the two components are engaged, providing maximum push-out and lever-out strength.

- Proximally porous coated Taperloc femoral component

- Porous coated cementless acetabular cup with highly crossed linked polyethylene liner
All surgeries were performed in lateral position using postero-lateral approach. 19 patients received epidural with spinal anaesthesia and nine patients received only spinal anesthesia. Antibiotics were administered thirty minutes preoperatively and continued for 3 days postoperatively. Anticoagulation prophylaxis consisted of 2.5 mg fondaparinaux subcutaneous daily for 5 days. Mobilization was started from second post-operative day with the help of walker allowing full weight bearing.
Clinical and radiographic analysis
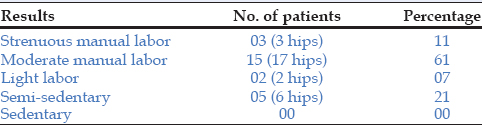
Patients were evaluated preoperatively and immediate postoperatively and at 1 month, 3 months, 6 months, 1 year and every other year thereafter. The Harris hip score was used to determine functional level and evaluate pain.[4] In addition, the presence or absence of thigh pain was recorded. A result was considered excellent if the Harris hip score was between 90-100, good if between 80-89, fair if between 70-79, and poor if less than 70. Activity level was evaluated by the classification of Johnston et al.[5] Heavy manual labour was defined as frequently lifting 23-45 kg or engaged in vigorous sports. Moderate manual labor was defined as lifting 23 kg or less and involved in moderate sports. Light labor included heavy lifting, house cleaning, and walking less than 5 km. Semi-sedentary indicated white collar job or light housekeeping. Sedentary activity indicated minimal capacity for walking, and bedridden was defined as being confined to a wheelchair or bed.
Radiographic analysis consisted of antero-posterior views of the hip and pelvis, a true lateral view of the hip. The immediate postoperative radiographs were compared with the most recent radiographs. The femur was divided into the seven zones as described by Gruen et al.,[6] [Figure 3]. All radiographs were assessed for radiolucencies and osteolysis in each of these zones. Radiolucencies with a scalloped or cystic appearance or greater than 2 mm in width were recorded as osteolysis. Femoral component stability was evaluated by the criteria of Engh et al.[7] A stable implant demonstrated no migration. Stable fibrous ingrowth occurred when an implant showed no progressive migration. Definite femoral loosening was defined as progressive migration of the implant. Subsidence was analyzed by the technique of Pellegrini et al.[8] Subsidence occurred if the stem settled greater than 4 mm. Femoral component alignment was considered neutral if the center lines of the implant and the femur were within 3 degree. A difference of greater than 3 degree indicated a varus or valgus orientation.[9] The Student t-test and Fisher exact test were used to determine significance.
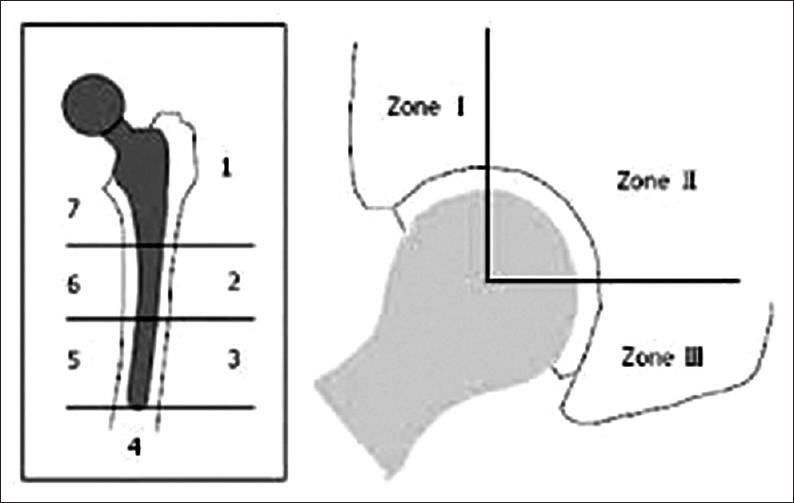
- Zone system used by Gruen et al
Observations and Results
Twenty-five patients (28 hips) were included in the study according to inclusion criteria and all of them available for both clinical and radiographic evaluation. Eight patients (nine hips) were excluded as their age was more than 40 years (exclusion criteria). There were eight females (nine hips) and 17 males (19 hips) in the study group. The mean follow-up was 2 years 10 months (range 2-4 years). The average age of the patients at the time of surgery was 27 years (range, 20-39 years). There were 12 left-sided and 16 right sided THRs among them three patients had bilateral THR. The etiology of hip arthritis for which patients underwent total hip arthroplasty is noted in Table 1. The average period of hospitalization was 12 days (range 10-21 days), average operative time was 90 min (range 70-100 min) and average blood loss was 450 ml (range 300-600 ml) measured by mop count.
Two patients (7%) had intra-operative hoop stress fractures of proximal femur, of which one was managed conservatively by keeping the patient non weight bearing for 6 weeks and another one with cerclage wiring [Figure 4a and b]. Three (11%) patients had anterior thigh pain which subsided with conservative management subsequently; none of these patients had restricted activity due to intensity of pain. Two (7%) patients had leg length discrepancy more than 2 cm [Figure 5a and b] and one (3.5%) patient had superficial infection of the operated wound which was managed with antibiotics and regular wound dressing. None of the patients had any major complication nor required revision till date.
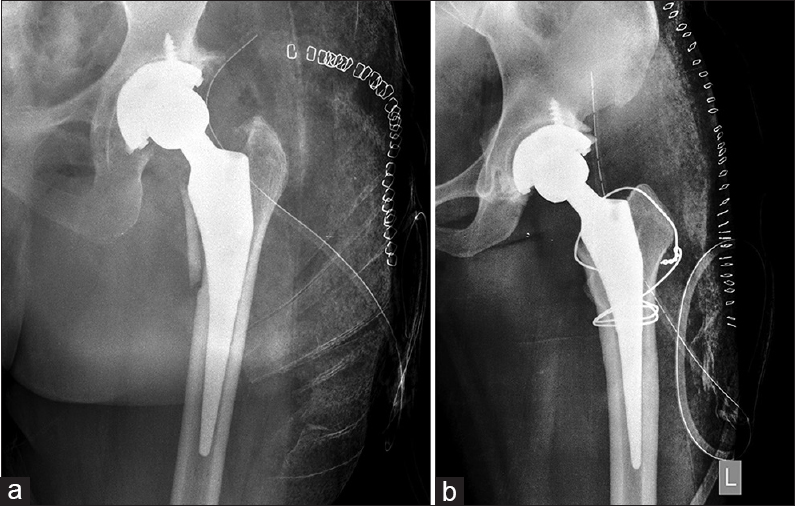
- (a) Intra-operative hoop stress fractures of proximal femur. (b) Intra-operative hoop stress fractures of proximal femur with cerclage wire

- (a) Post Total hip arthroplasty leg length discrepancy. (b) Post Total hip arthroplasty leg length discrepancy
The Harris hip score at a minimum follow-up of 2 years was available for all 28 hips. The mean Harris hip score increased from 34 points (range 15-46) preoperatively to 93 points (range, 76-96) at final follow-up. There was marked increase in post operative Harris hip score as compared to the pre operative Harris hip score, mean increase being 59 points, lowest improvement being 43 points and highest improvement in post operative Harris hip score being 74 points suggesting marked improvement in the functional outcome of the patient after total hip arthroplasty. The clinical outcome according to Harris hip score is depicted in Table 2. Patient having fair result had limb length discrepancy of 3 cm. At the time of last follow-up, the activity level as evaluated by the classification of Johnston et al., is given in Table 3.
Radiographic assessment revealed consistent evidence of bony ingrowth. Two femoral components (7%) had subsided 2 mm each in the first month postoperatively and had remained stable thereafter. No femoral component was loose. The femoral stem was aligned in neutral position in 22 (79%) hips, valgus in five (18%) hip and varus in one (3%). Statistical analysis showed no relationship between the initial alignment of the femoral component and clinical. Proximal metaphyseal filling was satisfactory in both antero-posterior and lateral X-rays in all the cases. There was no sign of osteolysis or loosening of the femoral component. All the acetabular components were stable. Angle of inclination in 97% of patients was between 40-50 degrees. The average acetabular inclination was 43 degree. Superior coverage was more than 95% in all the hips. None of the cup showed signs of osteolysis or loosening like radiolucent line around porous surface or loss of position of the cup [Figure 6a]-d and [Figure 7a]-d.
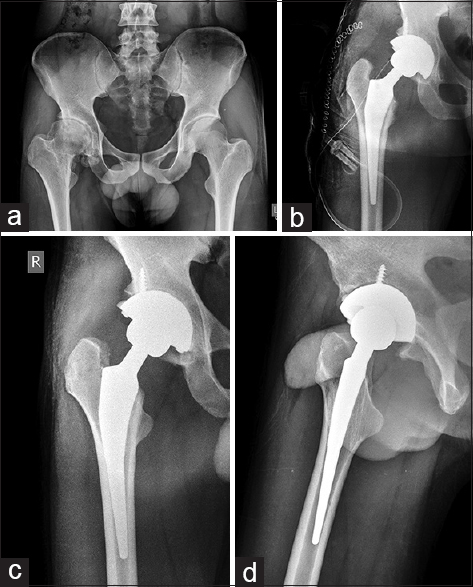
- (a) Pre operative x ray of pelvis with both hips showing right hip arthritis in 31 years male. (b) Immediate post operative X ray after cement-less total hip arthroplasty. (c) X ray right hip AP view at 3 yrs follow up with no signs of osteolysis, subsidence or loosening. (d) X ray right hip lateral view at 3 years follow up with no signs of osteolysis, subsidence or loosening
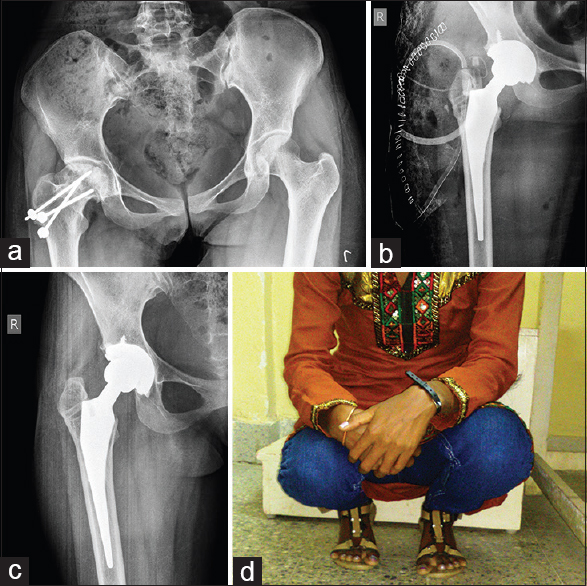
- (a) Pre operative X ray of pelvis with both hips showing post traumatic right hip arthritis in 20 years female. (b) Immediate post operative X ray after cement-less total hip arthroplasty. (c) X ray right hip AP view at 4 yrs follow up with no signs of osteolysis, subsidence or loosening. (d) Clinical result at 4 yrs follow up showing almost complete range of motion
Discussion
Total hip arthroplasty is undisputedly a successful and safe surgical procedure with excellent long term outcome in older patients.[10,11,12,13] The use of total hip arthroplasty as a salvage procedure in young patients with disabling hip diseases has generated theoretical, philosophical and practical debates. Only a few reports in the orthopedic literature have discussed THA in the very young population at the time of surgery whose lifestyle is physically and mentally more demanding.[14,15] The debate is particularly important with regard to young patients when considering the alternatives to THA: arthrodesis or resection arthroplasty. Both options provide considerable pain relief, but increase the degree of physical disability even in daily life, such as inability to sit on a regular chair or couch, severe limping and difficulties in playing sport. Furthermore, in medium to long-term follow-up after hip arthrodesis, there are reports of low back pain and ipsilateral knee pain in large number of patients. This is due to grossly altered biomechanics of the hip joint. Although most of the patients were satisfied with the results of the operation and had good functional outcome, many of them needed supportive aids for walking and activities of daily living.[16,17,18] The results of resection hip arthroplasty are much worse, especially when Harris hip score is considered. There are poor functional outcome, and low satisfaction rate. Although mobility was acceptable, the measured average oxygen consumption was 264% higher than normal.
Moreover, neither arthrodesis nor resection arthroplasty is an acceptable or practical option for patients with bilateral hip arthritis.[19,20,21]
The higher failure rate of THA in the younger patients has been attributed to the high activity level and the excessive demand imposed on the prosthetic hip.[22] But the number of improvements in prosthesis design and the delivery of surgical care introduced in recent years to improve the longevity of the total hip arthroplasty implant especially in the younger patients have helped in getting better outcome in recent years. The introduction of modern generation cementless components may be considered as one such advancement that has lead to an increasing number of THAs being performed in the younger patient population. Thus cementless THA is generally considered the prosthesis of choice for treatment of hip arthritis in young patients. Modern generation cementless THA has been shown to have an excellent, and in some cases superior outcome compared to cemented THA.[23,24] As seen in the present study.
Results of cementless total hip arthroplasty with specific use of the Taperloc femoral component have been reported by several authors incorporating multiple patient groups, In all of these reports, total hip arthroplasty with use of the Taperloc femoral component was associated with a low prevalence of osteolysis and low incidence of aseptic loosening.[25] In the present study, cementless THA was performed with excellent to good results in 93% of patients. There were no revisions or any major complications up to last follow-up. We believe on the basis of these findings that tapered proximally porous coated femoral components and porous coated cementless acetabular cup with highly crossed linked polyethylene liner provide durable biological fixation in young patients who require total hip arthroplasty.
This study suffers some limitations. The cohort consists of a group of patients with a number of diagnoses that may confound the outcome particularly in the long-term. Also, this study reports the outcome of THA at a relatively short follow-up. Despite the aforementioned shortcomings, the study is important as it prospectively reports the outcome of cementless THA with modern generation prosthesis and operative techniques.
Conclusion
Cementless total hip arthroplasty can be safely and successfully performed in young patients with excellent results in short to midterm follow-up. There is high level of patient satisfaction with low complication rate. But longer duration of follow-up is required to concretely establish these results.
Financial support and sponsorship
Mahatma Gandhi institute of medical sciences, Sewagram.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Total hip and knee replacements: A survey of 261 hospitals in England. J R Soc Med. 1993;86:527-9.
- [Google Scholar]
- Total hip arthroplasty in patients younger than 30 years of age. Isr Med Assoc J. 2003;5:709-12.
- [Google Scholar]
- Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. An end-result study using a new method of evaluation. J Bone Joint Surg Am. 1969;51:737-55.
- [CrossRef] [Google Scholar]
- Clinical and radiographic evaluation of total hip replacement. A standard of terminology for reporting results. J Bone Joint Surg Am. 1990;72:161-8.
- [CrossRef] [Google Scholar]
- “Modes of failure” of cemented stem-type femoral components: A radiographic analysis of loosening. Clin Orthop 1979:17.
- [CrossRef] [Google Scholar]
- Porous-coated hip replacement. The factors governing bone ingrowth, stress shielding and clinical results. J Bone Joint Surg Br. 1987;69:45-55.
- [CrossRef] [PubMed] [Google Scholar]
- A collarless cobalt chrome femoral component in uncemented total hip arthroplasty. Five- to eight-year follow-up. J Bone Joint Surg Br. 1992;74:814-21.
- [CrossRef] [PubMed] [Google Scholar]
- Primary total hip reconstruction with a titanium fiber-coated prosthesis inserted without cement. J Bone Joint Surg Am. 1993;75:554-71.
- [CrossRef] [PubMed] [Google Scholar]
- Primary total hip arthroplasty with an uncemented femoral component: Two- to seven-year results. J Arthroplasty. 2007;22:43-6.
- [CrossRef] [PubMed] [Google Scholar]
- Uncemented primary press-fit total hip arthroplasty: A 3 to 6 years of experience. J Orthop Surg (Hong Kong). 2007;15:50-5.
- [CrossRef] [PubMed] [Google Scholar]
- The porous coated anatomic total hip replacement. A ten to fourteen-year follow-up study of a cementless total hip arthroplasty. J Bone Joint Surg Am. 2001;83:1333-8.
- [CrossRef] [Google Scholar]
- Uncemented porous-coated anatomic total hip replacement. Results at six years in a consecutive series. J Bone Joint Surg Br 1993:6-14.:75-14.
- [CrossRef] [PubMed] [Google Scholar]
- Hydroxyapatite coated implants. Total hip arthroplasty in the young patient and patients with avascular necrosis. Clin Orthop. 1997;344:124-38.
- [CrossRef] [Google Scholar]
- Total hip arthroplasties in patients younger than 45 years: A nine-to-ten year follow-up study. Clin Orthop Relat Res 1990:215-9.
- [CrossRef] [Google Scholar]
- Hip arthrodesis. A long term follow-up. J Bone Joint Surg Am. 1985;67:1328-35.
- [CrossRef] [Google Scholar]
- Hip arthrodesis in young patients. A long-term follow-up study. J Bone Joint Surg Am. 1984;66:853-9.
- [CrossRef] [PubMed] [Google Scholar]
- Girdlestone arthroplasty for loosening of the total hip prosthesis: Evaluation and results. Chir Organ Mov. 1995;80:279-85.
- [Google Scholar]
- A six-year follow-up of infected total hip replacements managed by Girdlestone′s arthroplasty. J Bone Joint Surg Br. 1984;66:340-3.
- [CrossRef] [PubMed] [Google Scholar]
- Girdlestone arthroplasty for infected total hip arthroplasty. Clin Orthop Relat Res 1982:83-7.
- [CrossRef] [Google Scholar]
- Total hip arthroplasty in patients younger than 21 years: A minimum, 10- year follow-up. Can J Surg. 2003;46:257-62.
- [Google Scholar]
- Longterm results of Charnley-Kerboull hip arthroplasty in patients younger than 50 years. Clin Orthop Relat Res 2004:112-8.
- [CrossRef] [PubMed] [Google Scholar]
- Contemporary total hip arthroplasty with and without cement in patients with osteonecrosis of the femoral head. J Bone Joint Surg Am 2003:675-81.:85-81.
- [CrossRef] [PubMed] [Google Scholar]
- Total hip arthroplasty with an uncemented tapered femoral component in patients younger than 50 years. J Arthroplasty. 2011;26:9-15.
- [CrossRef] [PubMed] [Google Scholar]




