
Translate this page into:
Management of C1-C2 instability with distorted cranio-vertebral anatomy by using 3D CT angiography model: A rare case report
Address for correspondence: Dr. Tushar Chandrakant Patil, Department of Orthopaedics, Grant Govt Medical College, Mumbai, Maharashtra, India. E-mail: tushar6919@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Mahajan NP, Chandanwale AS, Sonawane DV, Patil TC. Management of C1-C2 instability with distorted cranio-vertebral anatomy by using 3D CT angiography model: A rare case report. J Orthop Spine 2021;9:94-100.
Abstract
Atlantoaxial instability is between C1/atlas and C2/axis, and it can be caused by different conditions such as congenital anomalies (Down syndrome, Morquio syndrome, and other skeletal dysplasias), inflammatory diseases, traumatic fractures, tumors, and infections. This necessitates the need for surgical occipito-cervical fusion (OCF) to prevent further injury to the spinal cord and subsequent myelopathy. Atlantoaxial instability is a rare condition and is commonly seen in 30% of patients with Down syndrome and in 30–80% of patients with rheumatoid arthritis; however, very few are symptomatic. Here, we present a rare case of a 17-year-old male with atlantoaxial instability due to occipitalized atlas and congenital fusion of C2-C3. The patient was operated by occipitoaxial fixation using C2 pedicle screws and an occipital plate with a rod construct with onlay bone allograft for bony fusion. Occipitoaxial fixation with a significant decrease in atlantodental interval (ADI) can be obtained by the use of C2 pedicle screws, and an occipital plate with a rod construct provides a rigid fixation and stability in the management of atlantoaxial joint instability with C1-C2 fusion due to an onlay bone allograft. Unnecessary C1 instrumentation and donor site morbidity for bone autografts can be avoided. Use of the 3D CT model helps to delineate the altered occipitocervical and vertebral artery anatomy intraoperatively, which aids in appropriate reduction and fixation.
Keywords
3D CT model
atlanto axial
bone grafting
C1-C2
cranio vertebral
fusion
instability
occipito axial
occipito cervical
posterior fixation
posterior instrumentation

Introduction
Atlantoaxial instability is between C1/atlas and C2/axis, and it can be caused by different conditions such as congenital anomalies (Down syndrome, Morquio syndrome, and other skeletal dysplasias), inflammatory diseases, traumatic fractures, tumors, and infections. This necessitates the need for surgical occipito-cervical fusion (OCF) to prevent further injury to the spinal cord and subsequent myelopathy. It is a rare condition and is commonly seen in 30% of patients with Down syndrome and in 30–80% of patients with rheumatoid arthritis; however, very few are symptomatic.[1]
Congenital synostosis of the atlas to the occiput is seen in some patients with C1-C2 instability and is known as occipitalization of the atlas. It occurs due to the failure of segmentation and separation of the first cervical sclerotome into cranial and caudal parts.[2]
This causes pain, stiffness, and restricted neck movements; even trivial events such as sneezing may cause symptoms. This fusion can, in turn, increase the stress on the atlantoaxial joint, leading to ligamentous laxity with advancing age, hypermobility, and eventual C1-C2 instability.[2]
Another condition that is commonly associated with 72.7% of patients with Klippel Feil syndrome is congenital C2-C3 fusion. Occipitalization of C1 along with C2-C3 fusion in the same patient increases the stress on C1-C2 articulation, leading to an increased risk of further neurological complications.[3]
Increased atlantodental interval (ADI) of more than 5 mm in dynamic cervical X-rays suggests atlantoaxial instability. Neurological symptoms such as pain, myelopathy, and sensory or motor deficit due to nerve root or spinal cord compression are of more diagnostic significance than ADI.[4]
X-rays and computed tomography (CT) scans diagnose the bony destruction of the C1-C2 joint due to arthritic changes in osteoarthritis and rheumatological condition, causing pain to the patient while rotating the neck toward the involved side.[4]
Occipitocervical fusion is a technically challenging procedure due to the unique anatomy and function of this region. It is accompanied with the proximity of vital neurovascular structures with occasional anatomical variations.[1]
The perioperative and postoperative mortality rates have been found to be 2.7% due to the complexity of the procedure.[5]
Case Report
A 17-year-old male came to the OPD with neck pain since five months, radiating to the right upper limb with a tingling numbness of the right hand. There was no history of trauma or other comorbidities. There was no evidence of a short neck or a decreased hair line. On examination, the patient had decreased power of the right hand grip and the wrist, which was 4. The rest of the neurology was normal. On plain radiographs, occipitalization of the atlas with C2-C3 fusion was observed [Figure 1]. In CT and MRI scans [Figure 2], we can see the increased atlantodental interval of 9.8 mm. The 3D reconstruction and CT angiography of the cervical spine was done to rule out any anatomical variations [Figure 3] along with a 3D model of the cervical spine prepared to guide intraoperatively.

- Preoperative cervical spine X-rays showing occipitalized atlas and C2-C3 vertebral fusion
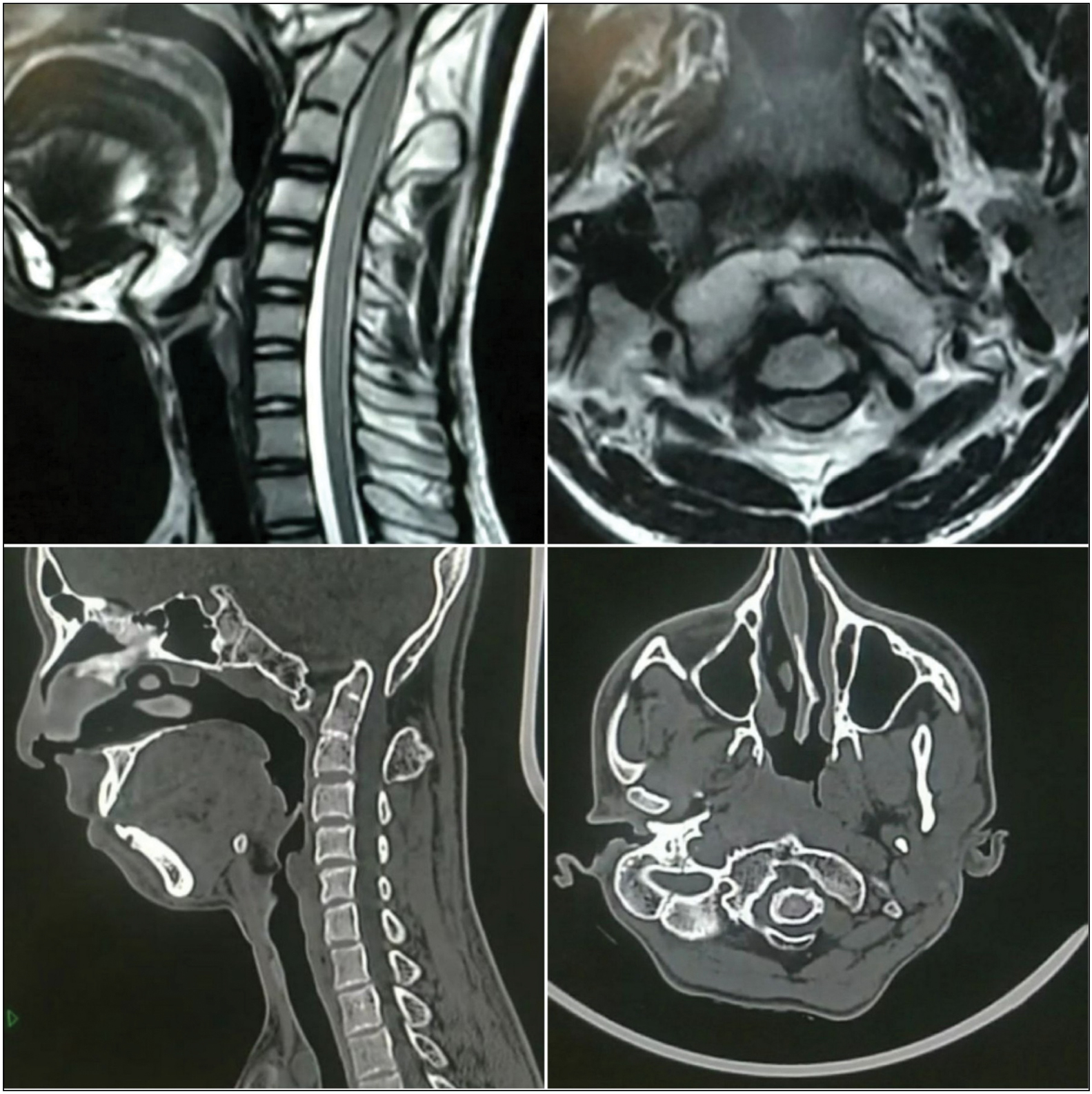
- Preoperative MRI and CT scan cuts of cervical spine with ADI more than 9.8 mm
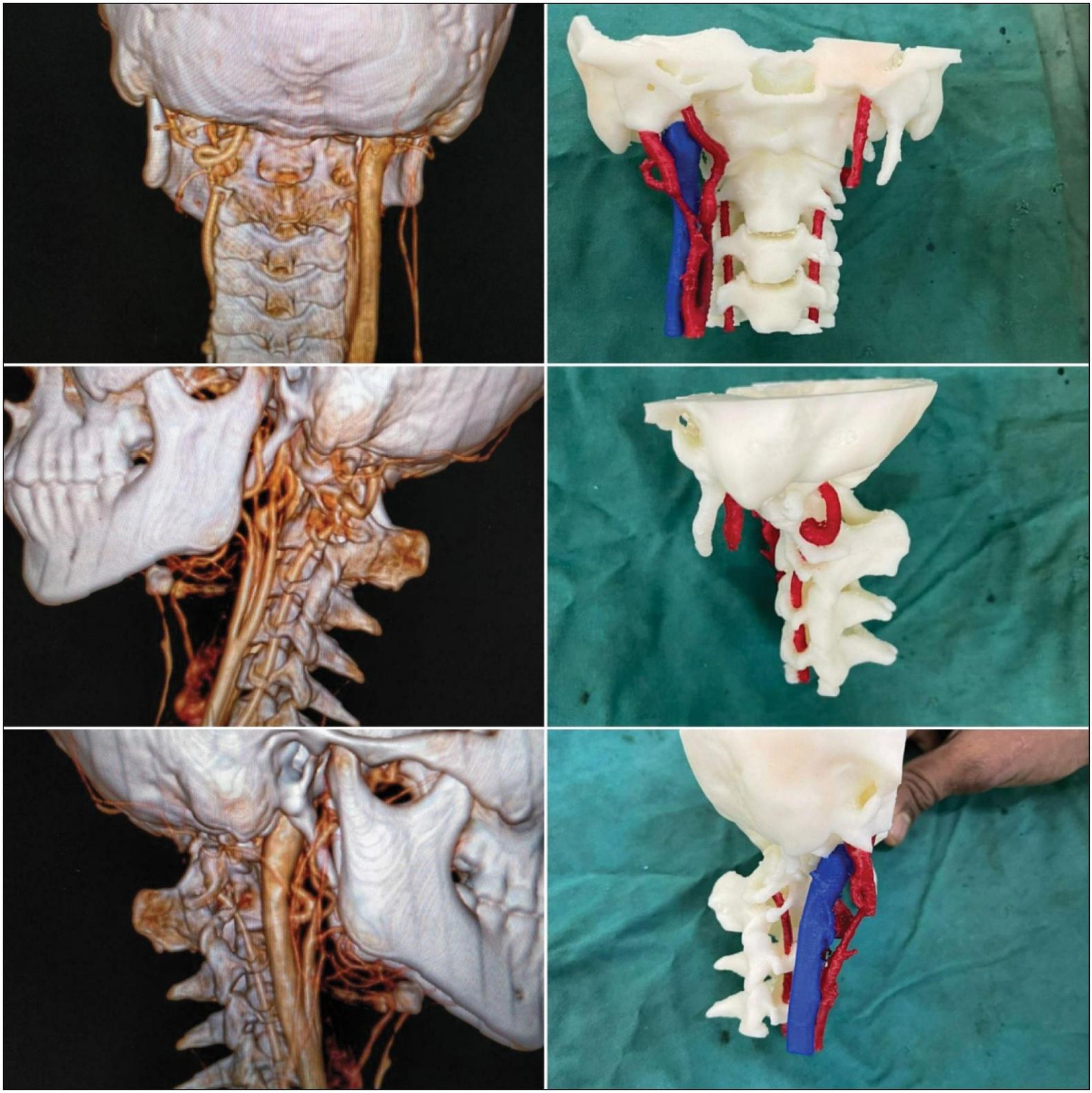
- Showing 3D CT angiography and 3D reconstruction model of cervical spine preoperatively
The patient was operated for C1-C2 instability by occipitoaxial fusion using two C2 pedicle screws and an occipital plate with a rod construct with an onlay bone allograft.
Surgical technique
The patient was taken on the operating table under all aseptic precautions and under general anesthesia in the prone position [Figure 4]. A midline incision was made from C1 to C4 level. Two pedicle screws were then inserted into the C2 vertebra. Entry for the C2 pedicle screws was 2 mm lateral to the midpoint of the pars over an imaginary line extending along the rostral border of the C2 lamina in the cranio caudal direction. A line was drawn along the cranial leading edge of the C2 lamina, and a line was drawn along the midpoint of the pars mediolaterally. The point of intersection was taken as the insertion point for the C2 pedicle screw. An occipital plate was placed just below the superior nuchal line, and it was fixed with 8 × 4 mm screws. Two connecting rods were placed on either sides connecting the polyaxial screws of C2 to the occipital plate. The cervical spine was then extended to decrease the ADI, and final tightening was done. The C1-C2 lamina were shingled posteriorly with a burr, and a bone allograft was placed onlay [Figure 5]. Deep closure was done with vicryl 1 and vicryl 2.0. The skin was closed with ethilon 2.0.

- Showing positioning of patient on operating table
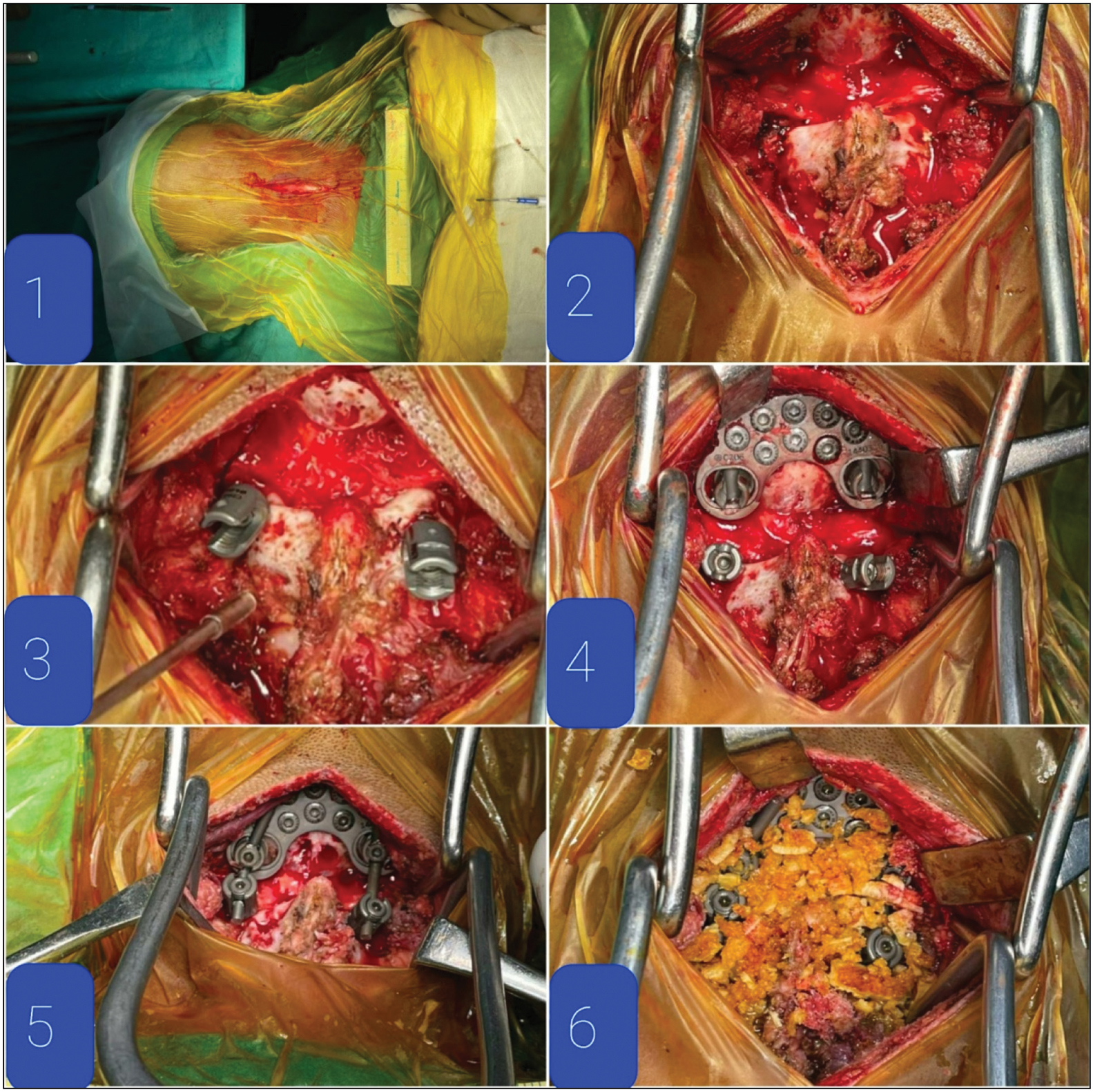
- Intraoperative pictures showing 1. Midline incision, 2. Exposure of lamina and pedicles of C2 vertebra and occiput below superior nuchal line, 3. C2 pedicle screws inserted, 4. Occipital plate fixed below superior nuchal line, 5. Connecting rods attached on both sides, and 6. Onlay bone allografting done after placing in antibiotic solution
Postoperative X-rays and CT scans showed decreased ADI [Figure 6]. There was immediate relief from radiation and tingling numbness with an improved power of hand grip and wrist to grade 5.
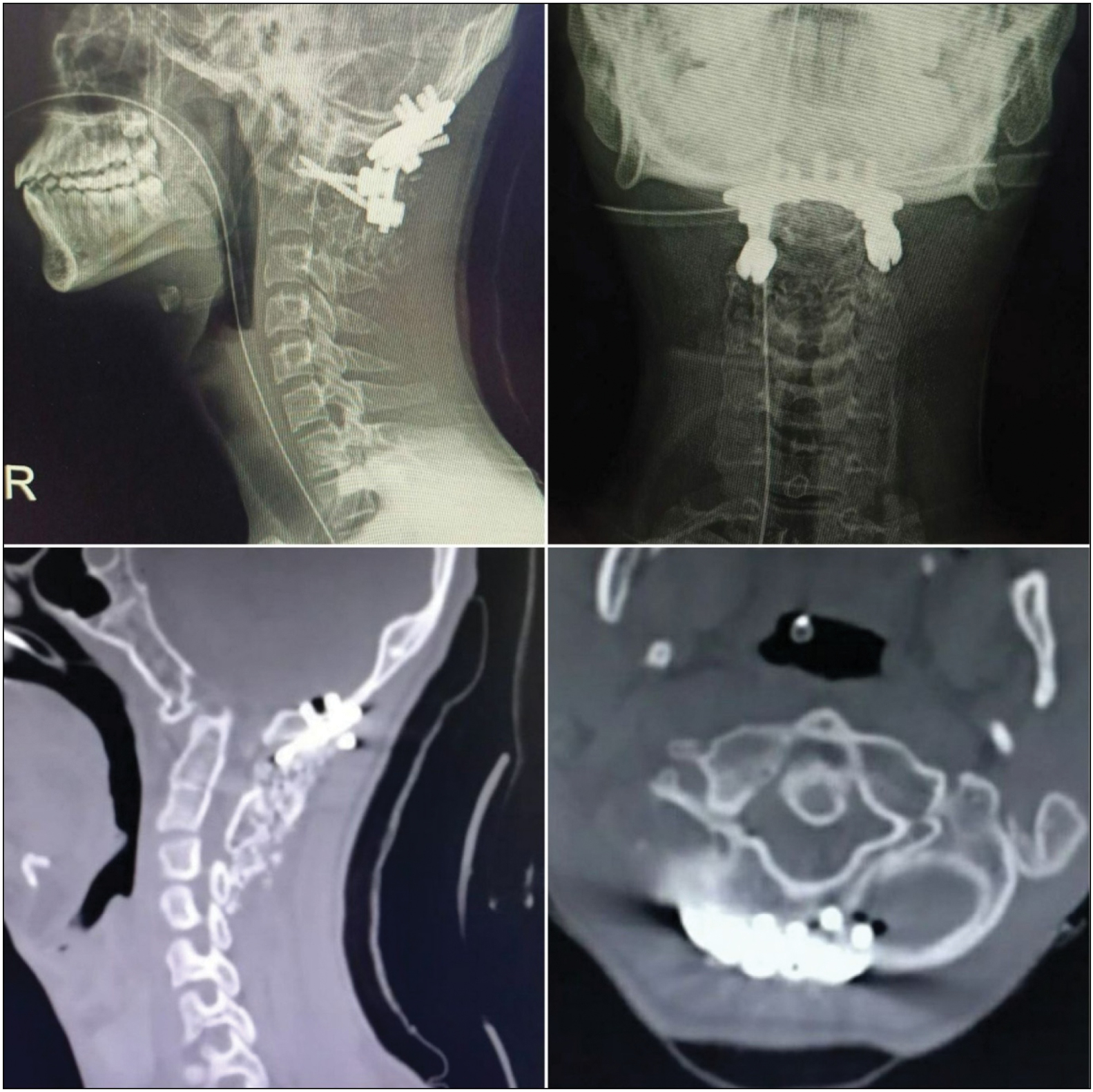
- Immediate postoperative X-rays and CT scan showing decreased ADI
The patient was relieved of all symptoms of nerve root compression and neurodeficit immediately postoperatively.
Postoperative immediate mobilization was started with a Philadelphia collar that was given for three months. The patient was checked and was found to be healthy on postoperative day 3. Suture removal was done on day 11.
Discussion
C1 or the atlas articulates with C2 or the axis to form an atlantoaxial joint. It is a mobile synovial joint with four interfaces that are formed by posterior surface of the atlas, odontoid process of the axis, transverse ligaments, and bilateral atlantoaxial facet joints. The main function of this joint is axial rotation with a limited amount of flexion or extension and the least amount of lateral bending. The atlantoaxial range of motion is found to be 38.9 degrees of axial rotation on either side, 11.5 degrees of flexion, 10.9 degrees of extension, and 6.7 degrees of lateral bending on either side.[4]
Multidirectional instability forces due to trauma and other pathological conditions affect the osseoligamentous complex of the atlantoaxial joint.[6]
Various vascular anomalies of vertebral arteries at the craniovertebral junction make surgeries technically more challenging. Persistent first intersegmental artery, fenestrated vertebral artery, low lying posterior inferior cerebral artery, and high riding vertebral artery are some vascular anomalies that increase the risk of vascular injury.[7]
Mixter and Osgood introduced sublaminar wiring techniques in 1910, for management of C1-C2 instability caused by odontoid fracture. They passed a stout braided silk under the C1 posterior arch and then tied with C2 spinous process. Interlaminar clamping for subaxial cervical fractures was first introduced in 1975 by Tucker. It was later used for C1-C2 stabilization by Halifax. Transarticular screw (TAS) fixation was first introduced in 1979 by Magerl and Seeman. Here, threaded screws are inserted 3 mm medial and 3 mm cranial from the medial margin of the C2-C3 facet joint, through the pars of axis, C1-C2 facet joints and finally coming out through the C1 lateral mass.[4]
Posterior fixation using the C1 lateral mass screw and the C2 pars screw connected by posterior cervical plates was first introduced by Goel and Laheri in 1994. It provided rigid internal fixation with early mobilization. Bony fusion was augmented with onlay and interfacet bone grafts.[8]
Modification of the technique was introduced by Harms and Melcher in 2001. Here, the C2 nerve root is only retracted caudally to expose the C1 lateral mass. The C1 entry point is in the middle of the posterior arch and is the postero-inferior point of the C1 lateral mass. The C2 entry point is at the cranial and medial quadrant of the lateral mass. The screw is directed 20 to 30 degrees medially and cranially while remaining parallel to the medial and superior surface of the C2 isthmus. Connecting rods are used through these polyaxial screws for stabilization. Arthrodesis is done by using a bone graft over the decorticated C1-C2 lamina posteriorly. In literature, this technique has been considered as a gold standard by many authors for C1-C2 fusion.[9]
Posterior occipito-cervical fixation was introduced by Abumi et al. in 1999; this technique uses pedicle screws. A construct with C1 lateral mass screw with C2 pedicle screw fixation was found to be more rigid than a construct with C1 and C2 lateral mass screws fixation. The bicortical screws purchase in former construct, provided superior stability in axial rotation and lateral bending compared with C2 lamina cancellous screw fixation in the latter.[4]
Sutterlin et al. stated that OCF using modern plate systems provides better stiffness and stability than traditional wiring techniques in terms of extension and torsion. However, in extreme flexion, fracture of the C2 pedicle was seen in a few cases.[4]
Hankinson et al. found that there was no distinct advantage of including C1 in OCF. They found that when good C2 fixation is achieved, it is unnecessary to include C1 lateral mass fixation and thus can avoid complications such as venous bleeding, vertebral artery injury, and C2 neuropathy. The C2 vertebra can be chosen as lower instrumented vertebra. Also, there was no biomechanical or statistically significant difference in fusion rates and neurological improvements, deeming subaxial fusion as unnecessary.[4,6]
Posterior OCF with an autograft provides an ideal substrate for fusion but the associated rate of donor site morbidity is quite significant leading to pain, increased blood loss, more operative time, infection, cosmetic problems, peripheral nerve damage, and difficulty in postoperative mobilization. Structural allografts provide reliable bony fusion and low morbidity.[10]
Allografts can cause immunogenic reactions and infection that can be eliminated by thorough donor screening with bone graft processing carried out by newer bone banks. Infection rates from allografts can be minimized by using antibiotic impregnated bone cements or mixing antibiotics manually or by directly placing allografts in antibiotic solution for a certain time period. Placing of the bone allograft directly in the antibiotic solution obliviates the need of bone cement and its colonization with certain infective organisms.[10]
Conclusion
Occipitoaxial fixation with a significant decrease in ADI can be obtained by the use of C2 pedicle screws, and an occipital plate with a rod construct provides a rigid fixation and stability in the management of atlantoaxial joint instability with C1-C2 fusion due to onlay bone allograft. Unnecessary C1 instrumentation and donor site morbidity for bone autografts can be avoided. Use of the 3D CT model helps to delineate the altered occipitocervical and vertebral artery anatomy intraoperatively, which aids in appropriate reduction and fixation.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Occipito-cervical fusion: Review of surgical indications, techniques and clinical outcomes. Sa Orthopaedic J. 2010;9:26-32.
- [Google Scholar]
- Occipitalisation of atlas-a case report. University Journal of Pre and Paraclinical Sciences. 2020;6
- [Google Scholar]
- Occipitalization of the atlas in children: Morphologic classification, associations, and clinical relevance. JBJS. 2007;89:571-8.
- [CrossRef] [PubMed] [Google Scholar]
- Posterior atlantoaxial fusion: A comprehensive review of surgical techniques and relevant vascular anomalies. J Spine Surg. 2020;6:164-80.
- [CrossRef] [PubMed] [Google Scholar]
- Atlantoaxial fusion: Sixteen years of epidemiology, indications, and complications in new york state. Spine (Phila Pa 1976). 2016;41:1586-92.
- [CrossRef] [PubMed] [Google Scholar]
- Occipitocervical fixation: General considerations and surgical technique. Global Spine J. 2020;10:647-56.
- [CrossRef] [PubMed] [Google Scholar]
- Risk of vertebral artery injury: Comparison between C1-C2 transarticular and C2 pedicle screws. Spine J. 2013;13:775-85.
- [CrossRef] [PubMed] [Google Scholar]
- Atlantoaxial fixation using plate and screw method: A report of 160 treated patients. Neurosurgery. 2002;51:1351-6. discussion: 1356-7
- [CrossRef] [PubMed] [Google Scholar]
- Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine (Phila Pa 1976). 2001;26:2467-71.
- [CrossRef] [PubMed] [Google Scholar]




