
Translate this page into:
LUMBAR facet denervation for degenerative symptomatic functional spinal unit: Overview
Address for correspondence: Dr. Satishchandra Gore, Spine Clinic 1128 Shivajinagar FC Road, Pune - 411 016, Maharashtra, India. E-mail: yesgore@yahoo.co.in
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Gore S. LUMBAR facet denervation for degenerative symptomatic functional spinal unit: Overview. J Orthop Allied Sci 2018;6:S8-12.
Abstract
Symptomatic lumbar facets manifest as low back pain located paraspinally of varying intensity. The pain may increase with extension and rotation and can be well localized or diffuse and associated with extension lag on prolonged sitting. This pain can be easily identified by facet or medial branch block and then treated by ablating under vision this medial branch. Results are gratifying and can delay need for fusion in patients.
Keywords
Facet denervation
facetal arthropathy
low back pain
medial branch block

Introduction
Elderly patients may have severe back pain due to facet changes, they present clinically with bilateral paraspinal pain, that is increased with extension and or rotation. Traditionally fusion is suggested for the pain, in this age group. Presence of associated medical comorbidity may complicate the decision making and intervention. Facet denervation by nerve ablation may achieve pain relief, with intervention under local anesthesia. It is a visualized least morbid surgery without use of implants.
Facet Innervation
Lower lumbar facet joints are commonly symptomatic; affected by degenerative changes. Facet is innervated on its lateral surface by the medial branch of the dorsal ramus of the index level. The medial branch travels over the transverse process under the mamillo-accessory ligament [ligament is along upper border of the transverse process]. The segmental artery is at lower border of the transverse process, and within 5 mm under (ventral) is the lumbar plexus. Blue arrow [Figure 1] is pointing to medial branch on the transverse process. Additionally Nerve branches visualized near the foraminal ligament during foraminal endoscopy when ablated, may also provide back pain relief. These are pure sensory nerves from the dorsal ramus, innervating the facet joints dorsally without crossing the transverse process.
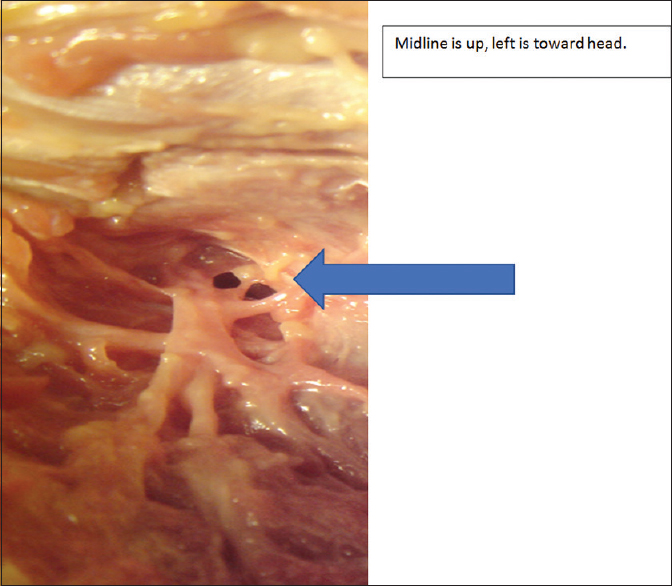
- Blue arrow showing medial branch of dorsal ramus on right transverse process dorsal surface
The medial dorsal surface of facet joint is supplied by the nerve branch coming from the level above. Thus, one facet has 2 nerves supplying it and needs denervation at 2 levels, one index and one above to cover both its medial and lateral dorsal surfaces by targeting medial branches. In general, facet change is bilateral change so we may be looking at 4 spot surgery in an elderly patient with facet related severe back pain.
History
Mooney and Robertson described facet syndrome in 1976. They used X-ray-guided localized injection of steroids and local anesthetic into facet joint as a diagnostic-therapeutic procedure. The facet joint was thought to be a persistent contributor to the chronic back pain in complaints of individuals with low back and leg pain.[1]
In 1982, Bogduk studied the anatomy of the facet and lumbar mamillo-accessory ligament (MAL) and the branches of the dorsal ramus which enervated the facet at [lateral surface] and below the disc segment level [medial facet surface]. The MAL encloses the medial branch of the dorsal ramus in an osseofibrous tunnel. The tunnel maintains the proximal course of the medial branch in a constant relationship to the bone. This constancy allows for percutaneous techniques to stimulate, anesthetize, or destroy the medial branch better than blinded radiofrequency (RF) ablation. The MAL is ossified in over 10% of lower lumbar vertebrae, and ossification may interfere with some percutaneous denervation techniques.[2] Visualized ablations are better as it can excise the tunnel roof and also document the targeting.
How to select a patient for denervation?
The degeneration of facet joints is a part of a process affecting the whole functional spinal unit.[3] If we see a patient with axial back pain age >65, pain relieved by lying down, pain not increasing by coughing, flexion, but increasing in rising from a flexed position, and aggravated by, extension and rotation, it may be related to the facet joint.[4] Commonly it is associated with limitation of extension well correlated with degree of degeneration. Test to confirm the origin of facet pain is to relieve it by injection of the facet joint or the medial branch with a local anesthetic. Controlled diagnostic studies have shown the prevalence of lumbar facet joint pain in only 27% to 40% of the patients with chronic low back pain (LBP) without disc herniation or radiculitis. Single block may have high false-positive results. Datta, et al. published evidence for the diagnosis of lumbar facet joint pain with controlled local anesthetic blocks as Level I or II.[5,6] Block giving 50% relief is used to select patients for denervation, but more stringent criteria may reduce its utility.[7] Uncontrolled medial branch blocks are superior to pericapsular blocks in selecting patients, but both blocks work. If serial controlled blocks cannot be used, lumbar facet joint pain remains a diagnostic dilemma.[8] Efficacy of denervation has been questioned in some studies.[9] It should be a joint decision for rhizotomy dependent on percentage of preoperative pain relief by the block.
Technique Step by Step
Imaging is usually utilized to determine whether the disc and other known pain generators can contribute to axial back pain as well. The location of the intermuscular cleavage plane between the multifidus and longissimus muscle provides surgical access to the branches of the dorsal ramus.[10,11]
The technique step by step is
Positioning patient prone on a radiolucent table
We normally are able to localize the level by palpating the painful joint or use a spinal needle 20g under x-ray control
Precise targeting of the medial branch is possible by using line drawing to locate it
In AP imaging of the lumbar spine vertical line is drawn along lateral pedicle line which intersects a horizontal line bisecting the pedicles at index level [Figure 2]
Local anesthesia is used for numbing skin and subcut tissue. A 20G spinal needle is put straight down and perpendicular to the transverse process aiming at upper border of the process
Depth of the process is generally not more than 40 mm
Palpation of bony transverse process is done and staying along upper border we try and go towards lateral wall of pedicle, where nerve is situated
A lateral image on c arm may be taken just to be sure about location and depth. Ventral to transverse process we have the lumbar plexus within 5-8 mm. Along lower border of the transverse process is the lumbar segmental artery
Once we have landed at the required spot 1 cc of local anesthetic lignocaine 2% plain is injected
After a few minutes patient is asked to extend his spine and confirm relief of pain. If patient is relieved upto 50% or more he may be suggested utility of facet denervation for long term, upto 2 years, relief of pain
During surgery further step is to introduce a guide wire in place of stylet of the spinal needle, and then a blunt dilator over the guide wire, and subsequently [Figure 3] working channel over the dilator. There is no need to cut muscles. They are dilated. If we are able to start about 1 cm lateral to skin marking point angulation of subsequent instruments is easy
Cannula is turned facing the body of vertebra and introduction of scope makes us visualize our target
Precise visualization can be aided by using mix of radio opaque and indigo carmine dye when first block is done. Using blunt dilator to clear soft tissue along the path of the nerve adds to better visualization
Ablation of nerve and its branches is done under vision with RF after cutting the nerve in middle and ablating both ends. Use of laser or any other ablating energy can be done
Adequacy of surgery can be judged by relief of the pain on extension by asking patient to extend spine on table
Normally we have to target 2 levels bilaterally. Medial branch of index level supplies lateral and nerve from level above supplies medial aspect of the facet
If we encounter mammilo accessory ligament forming roof of tunnel for the nerve it is generally found at upper medial border of the transverse process. This can be removed by using trephine to expose the under lying nerve. Use of periosteum elevator or a annular cutter also helps [Figure 4]
We also can use smaller length scope and instruments to facilitate working on dorsal surface [back] of the patient under c arm control
Surgery is entirely under local anesthesia and elderly patients with medical co morbidities can tolerate it well
MOST important tip is to stay dorsal to the transverse process and along its upper medial border.
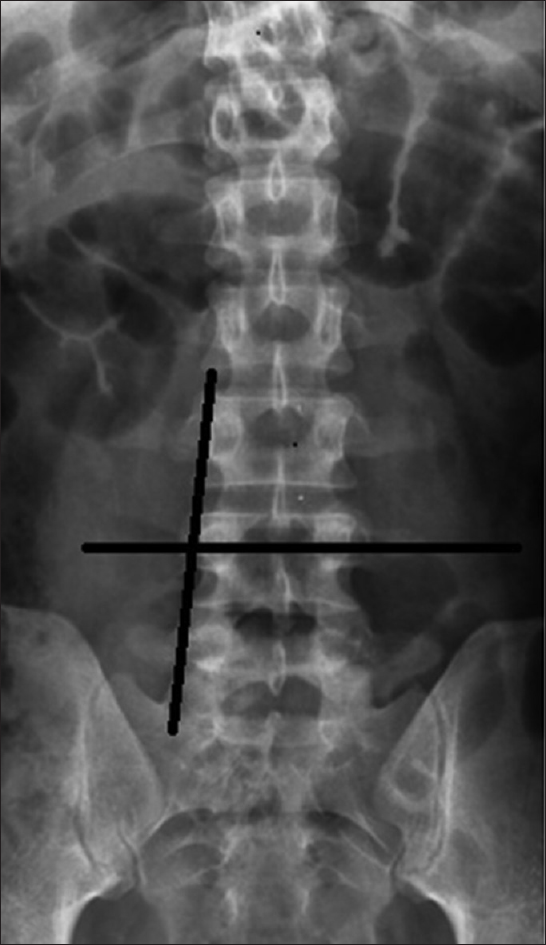
- Line drawn to land precisely on the medial branch of RT L45 level
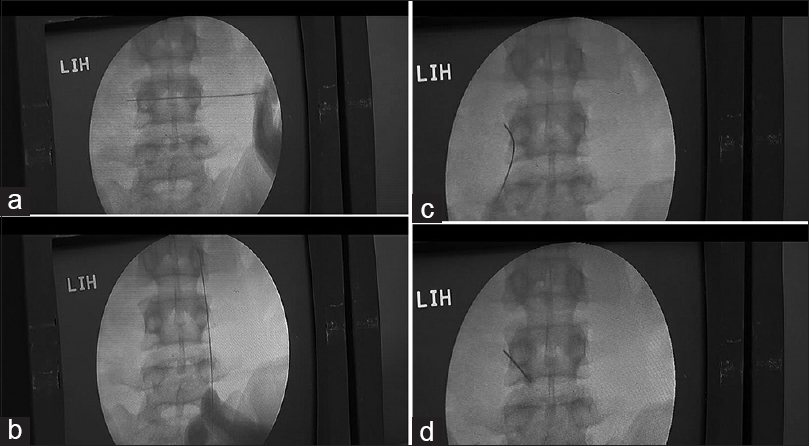
- (a-d) marker along, bisection of pedicles at L45 and lateral pedicle line, next 2 images show the needle inserted over the transverse process over its upper border and then the mid portion of the transverse process
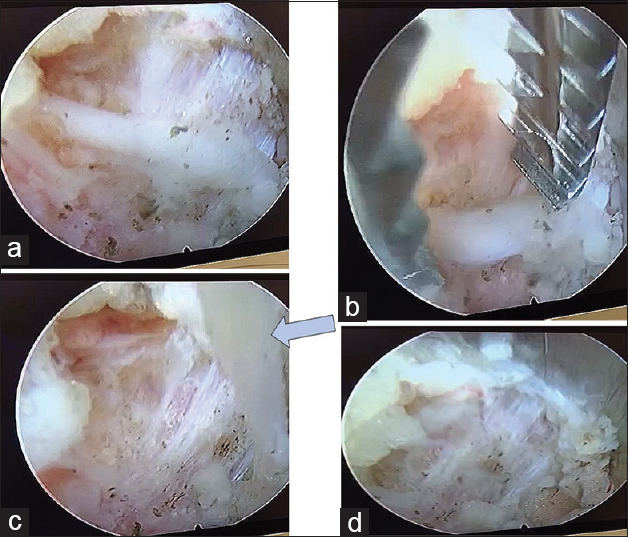
- (a-d) Intraop pics of transverse process of right side, head towards left. Midline is up
Complications
In fluoroscopically guided blind RF, denervation of the medial branch was associated with a 1% complication rate as sensory-motor deficit for 2 or more weeks.[12] The procedure, if done under endoscopically guided vision has no complications if proper protocol is followed, and the RF probe does not get ventral to the transverse process plane and does not penetrate the intertransverse ligament or go toward lower border of the transverse process. In our cases, when the thermal probe causes pain under local anesthesia, there can be a temporary dysesthesia only experienced in surgery or for a few hours or days postoperative. Staying away from the lower border of the transverse process helps in avoiding vascular injury. In osteoporotic patients extra care is needed to avoid breaking transverse process. It is important to remember that dilator used to land on transverse process is used manually and there is never need to use a mallet to drive it deep. This surgery is outside the facet joint cavity.
Postoperative Care
The patient is under local anesthetic and mild sedation. Once the patient is comfortable within a few hours, he/she can mobilize. Mild oral pain relievers are given for a few days. The patient can be active but should avoid twisting the back and extension movement for about 2–3 weeks to allow for soft-tissue healing. Core strength building exercises can be utilized to improve posture and mobility. There is no need for any postoperative imaging studies or lumbar support.
Outcome of Fluoroscopic Radiofrequency
Introduction of RF denervation was reported in 1975 by Shealy. In his study, 207 patients followed 6–21 months (mean 31 months). relief of pain was achieved in 79% of previously unoperated patients, in 41% of those with laminectomy but no fusion, and in 27% of those with an earlier fusion. No neurological complications were encountered.[13] If we can clinically identify that pain is of facet origin, then visualized endoscopic facet rhizotomy provides good/excellent results by Mac Nab criteria over 90% after 1-year follow-up. Ten percent have some pain returning after 1 year, but not to the index intensity level. The patient can avoid a hardware-assisted fusion in most of the cases. We have been able to relieve the pain in 85% patients when there is more than 50% relief on blocks given at index and level above. These have been visualized surgeries and not blind fluoroscopically guided. In summary, there is good evidence for the use of conventional RF neurotomy.[14] RF Denervation provides safe and significant short-term improvement in pain, analgesic requirements, function, satisfaction, and direct costs in patients with chronic LBP of facet origin.[15]
Among patients presenting with axial LBP, facet arthropathy accounts for approximately 10%–15% of cases. Currently, there are no uniformly accepted criteria regarding how best to select patients for RF denervation. By multivariate statistical analysis, patients undergoing bilateral blocks for bilateral or axial symptoms were significantly more likely to achieve temporary relief and to proceed to permanent denervation.[16] There was no difference, however, between the long-term results of bilateral denervation for bilateral or axial pain and those of unilateral denervation for unilateral pain. There was no significant difference in the rate of response between the 56 patients who had undergone prior lumbosacral spine surgery and the 26 who had not in this report.[17]
RF facet denervation is not a placebo and could be used in the treatment of carefully selected patients with chronic LBP.[18] RF lumbar zygapophysial joint denervation results in a significant alleviation of pain and functional disability in a select group of patients with chronic LBP, both on a short- and a long-term basis.[19] Large, prospective clinical audit as reported here indicates that proper patient selection and anatomically correct RF denervation of the lumbar zygapophysial joints provide long-term pain relief in a routine clinical setting.[20] Comparison of continuous RF and Pulsed RF suggests CRF is more effective and long-lasting.[21]
Medial branch may be covered with an osseous ligament over the transverse process that would require more effective visualized ablation than by conventional RF techniques
One joint has supply from 2 nerves one level above and same level so a bilateral 4-point surgery may be a norm
The dorsal ramus and its branches can be ablated from the foramen before it gets to the transverse process. There are also branches that go to the facet from the foramen and there are branches that do not cross the transverse process, but traverse the facet wall and pedicle. It is difficult to see, and are often stripped and ablated during foraminoplasty
Foraminoplasty will likely involve ablation of branches of the dorsal ramus before they exit the foramen to the facet joint. Ablation of the nerves by the superior articular process will provide axial back pain relief through rhizolysis in addition to foraminal decompression for sciatica.
Financial support and sponsorship
Nil.
Acknowledgement
Operative images are sourced from Dr. Daniel Hansen video share.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- The lumbar mamillo – Accessory ligament. Its anatomical and neurosurgical significance. Spine (Phila Pa 1976). 1981;6:162-7.
- [Google Scholar]
- 1988 Volvo award in clinical sciences. Facet joint injection in low-back pain. A prospective statistical study. Spine (Phila Pa 1976). 1988;13:966-71.
- [CrossRef] [PubMed] [Google Scholar]
- Capacity of the clinical picture to characterize low back pain relieved by facet joint Anesthesia. Proposed criteria to identify patients with painful facet joints. Spine (Phila Pa 1976). 1998;23:1972-6.
- [CrossRef] [PubMed] [Google Scholar]
- Endoscopically guided foraminal and dorsal rhizotomy for chronic axial back pain based on cadaver and endoscopically visualized anatomic study. Available from: ijssurgery.com/10.14444/1023 (accessed )
- [Google Scholar]
- Systematic assessment of diagnostic accuracy and therapeutic utility of lumbar facet joint interventions. Pain Physician. 2009;12:437-60.
- [CrossRef] [Google Scholar]
- Lumbar zygapophysial (facet) joint radiofrequency denervation success as a function of pain relief during diagnostic medial branch blocks: A multicenter analysis. Spine J. 2008;8:498-504.
- [CrossRef] [PubMed] [Google Scholar]
- Medial branch blocks versus pericapsular blocks in selecting patients for percutaneous cryodenervation of lumbar facet joints. Reg Anesth Pain Med. 2007;32:27-33.
- [CrossRef] [Google Scholar]
- Radiofrequency facet joint denervation in the treatment of low back pain: A placebo-controlled clinical trial to assess efficacy. Spine (Phila Pa 1976). 2001;26:1411-6.
- [CrossRef] [PubMed] [Google Scholar]
- Multilevel magnetic resonance imaging analysis of multifidus-longissimus cleavage planes in the lumbar spine and clinical application to the Wiltse approach. Pak J Med Sci. 2012;28:839-41.
- [Google Scholar]
- Anatomical study of the paraspinal approach to the lumbar spine. Eur Spine J. 2005;14:366-71.
- [CrossRef] [PubMed] [Google Scholar]
- Complications of lumbar facet radiofrequency denervation. Spine (Phila Pa 1976). 2004;29:1352-4.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous radiofrequency denervation of spinal facets. Treatment for chronic back pain and sciatica. J Neurosurg. 1975;43:448-51.
- [CrossRef] [PubMed] [Google Scholar]
- An update of the effectiveness of therapeutic lumbar facet joint interventions. Pain Physician. 2012;15:E909-53.
- [CrossRef] [Google Scholar]
- A prospective outcome study on the effects of facet joint radiofrequency denervation on pain, analgesic intake, disability, satisfaction, cost, and employment. Arch Phys Med Rehabil. 2009;90:201-5.
- [CrossRef] [PubMed] [Google Scholar]
- Radiofrequency lumbar facet denervation: Analysis of prognostic factors. Pain. 1994;57:77-83.
- [CrossRef] [PubMed] [Google Scholar]
- Percutaneous lumbar zygapophysial (Facet) joint neurotomy using radiofrequency current, in the management of chronic low back pain: A randomized double-blind trial. Spine (Phila Pa 1976). 2008;33:1291-7.
- [CrossRef] [PubMed] [Google Scholar]
- Randomized trial of radiofrequency lumbar facet denervation for chronic low back pain. Spine (Phila Pa 1976). 1999;24:1937-42.
- [CrossRef] [PubMed] [Google Scholar]
- Radiofrequency denervation of the lumbar zygapophysial joints: 10-year prospective clinical audit. Pain Physician. 2007;10:291-300.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison of conventional and pulsed radiofrequency denervation in the treatment of chronic facet joint pain. Clin J Pain. 2007;23:524-9.
- [CrossRef] [PubMed] [Google Scholar]
- A randomized, double-blind, prospective study comparing the efficacy of continuous versus pulsed radiofrequency in the treatment of lumbar facet syndrome. J Clin Anesth. 2008;20:534-7.
- [CrossRef] [PubMed] [Google Scholar]




