
Translate this page into:
Kummell’s disease treated with posterior instrumented stabilization and transpedicular biopsy: A case series
Address for correspondence: Dr. Prasad T. M. Suhruth, Department of Orthopedics, A J Institute of Medical Sciences and Research Centre, Mangalore 575004, Karnataka, India. E-mail: suhruthprasad392@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Suhruth PT, Ahamed TC, Nehal N, Gowda HM, Vaishakh BV, Pinto FA. Kummell’s disease treated with posterior instrumented stabilization and transpedicular biopsy: A case series. J Orthop Spine 2023;11:24-34.
Abstract
Kummell’s disease is avascular necrosis of vertebral body caused by a vertebral compression fracture. It is an osteonecrosis-related disease that can cause severe vertebral collapse, with severe pain, and may progress to kyphosis and neurological deficit. In this case series, we have reported five cases of Kummell’s disease. All the five patients were preoperatively bedridden due to pain in low back while mobilizing. Case 1 complained of low back pain radiating to left lower limb and had neurological deficits in L5 myotome. Other four cases complained of axial type of low back pain. All five patients underwent posterior instrumented stabilization and transpedicular aspiration of fluid along with biopsy; they were diagnosed as Kummell’s disease by exclusion. Postoperatively all five patients improved symptomatically and were able to walk with assistance. We found that posterior instrumented stabilization offered good patient-related outcomes in terms of pain and postoperative rehabilitation on short-term follow-up. Kummell’s disease is overlooked on X-ray when a patient presents at an early stage and hence a thorough knowledge of Kummell’s disease is required for the early treatment of these patients and prevention of complications.
Keywords
Kummell’s disease
posterior instrumented stabilization
transpedicular biopsy

Introduction
With an increase in life expectancy, osteoporosis and osteoporotic vertebral compression fractures are becoming more common. Few vertebral compression fractures progress to produce osteonecrosis, commonly known as Kummell’s disease, and the majority heal without problems.
Despite the high occurrence (varying from 7% to 37%),[1] there are not many instances that have been recorded. This is due to a number of issues, including a lack of awareness and the use of terms like “vertebral compression fracture nonunion,” “intervertebral vacuum cleft,” “delayed vertebral collapse,” “post-traumatic vertebral osteonecrosis,” “avascular necrosis,” and “vertebral pseudoarthrosis.”
Kummell’s disease typically affects middle-aged and elderly people. Patient experiences minor trauma with mild back pain. After a few weeks to months of no symptoms, the pain typically returns and is much worse. Sometimes a patient may exhibit considerable neurological involvement as well as kyphotic deformities. For the diagnosis of Kummell’s disease, radiographs and an magnetic resonance imaging (MRI) are necessary. Treatment options include conservative management and surgical intervention, which may include decompression and stabilization or vertebral augmentation therapies.
In this case series, five patients who had back pain and were unable to walk were included. They were identified as having Kummell’s disease, and they underwent surgical management with posterior instrumented stabilization and transpedicular biopsy.
Case Series
Case 1
An 82-year-old male patient with a history of regular yoga practice presented with a history of low back pain radiating to the left lower limb for 3 months. The patient was advised lumbar corset at a local hospital. The pain worsened and the patient developed difficulty in walking and was bedridden.
He had no h/o fever, chronic cough, h/o contact with tuberculosis, and no history suggestive of carcinoma.
On examination, there was kyphotic deformity with tenderness over the lumbar vertebra. Neurological examination revealed motor weakness of B/L L5 myotome. B/L ankle reflexes were mute.
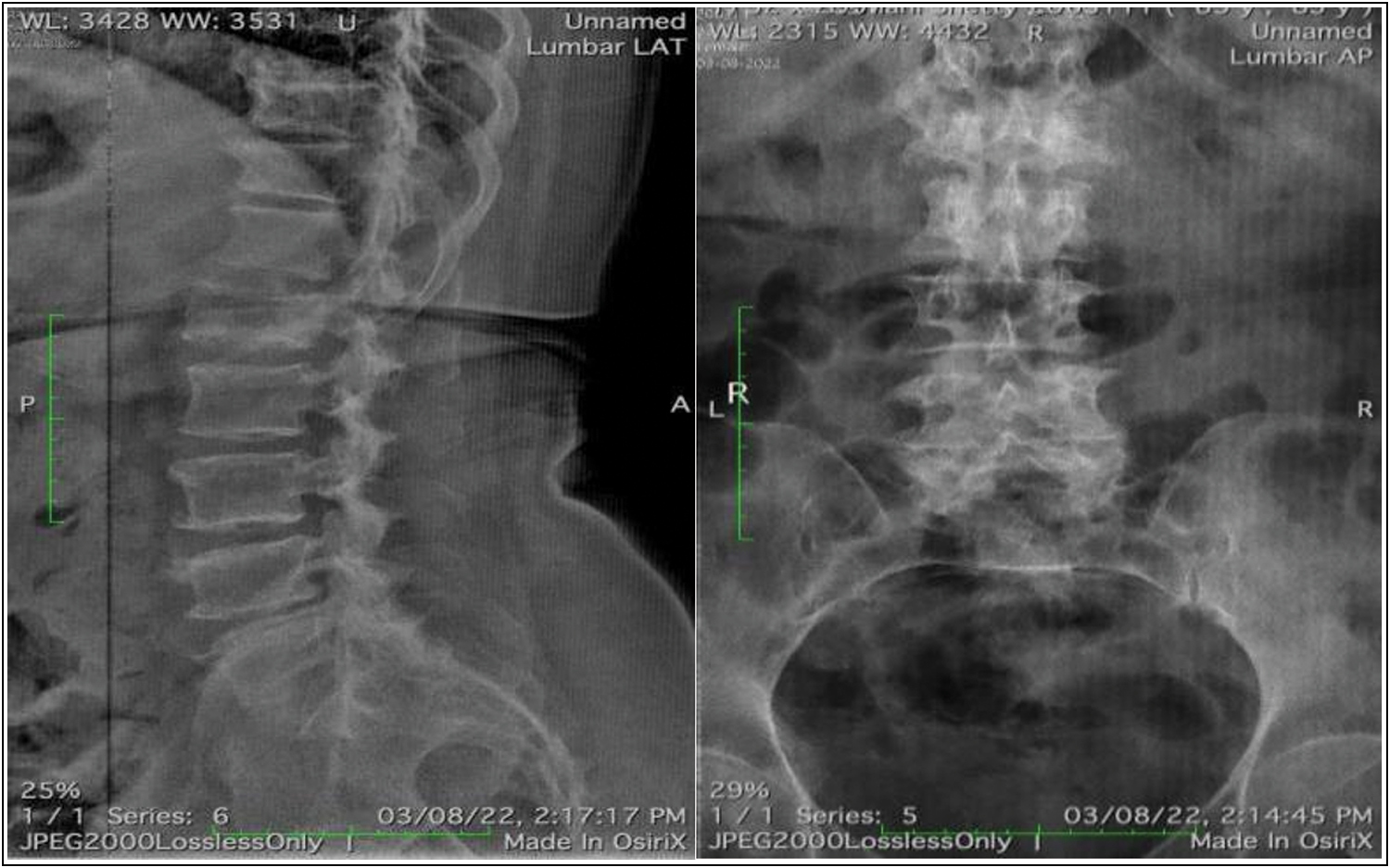
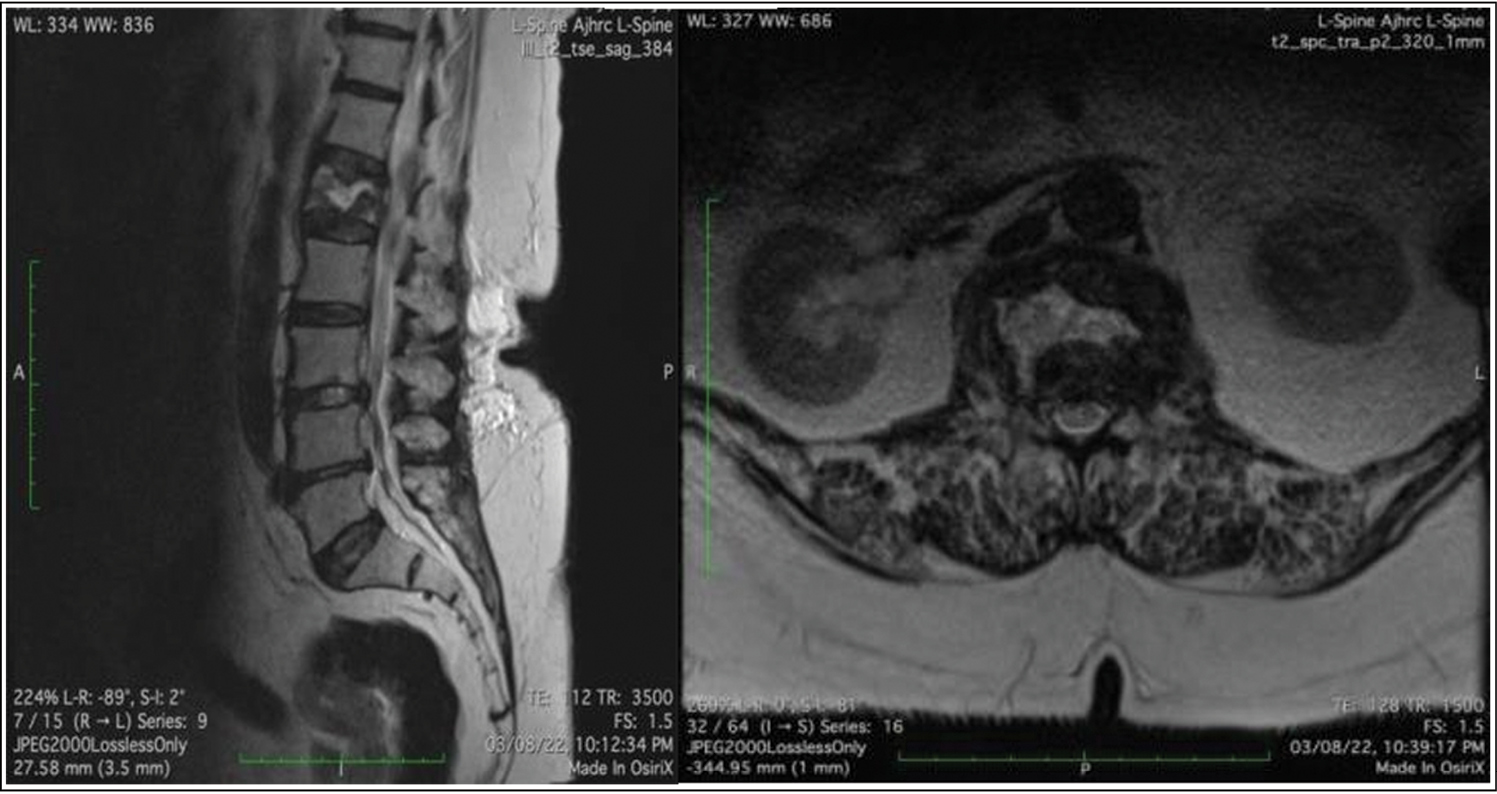
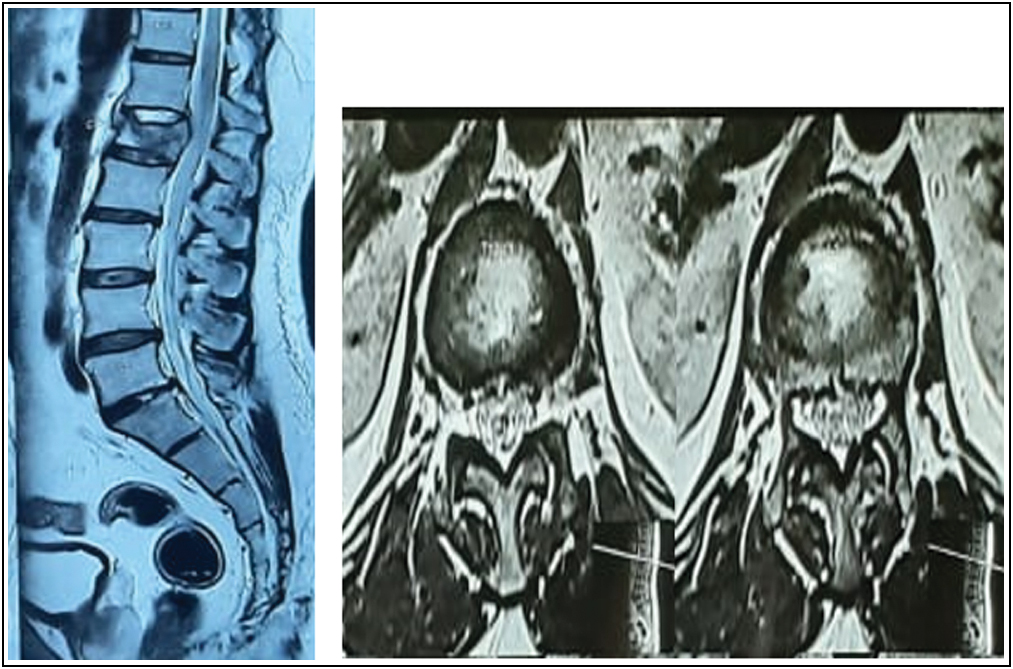
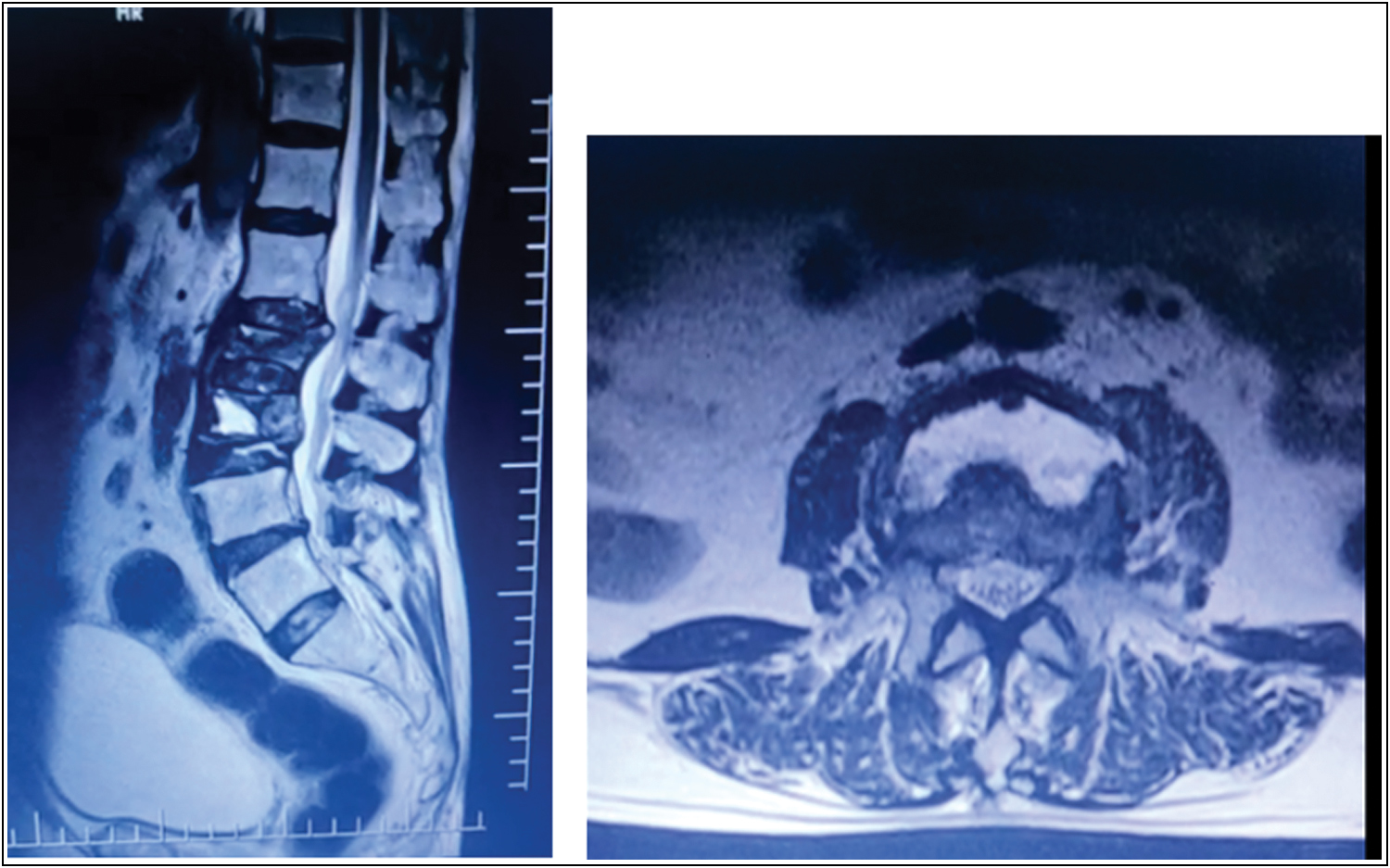
Radiological evaluation of anterior-posterior (AP) and lateral radiographs revealed a compression fracture of the L2 vertebra and compression of the spinal canal with radiolucency noted in the body of vertebra [Figure 1]. MRI revealed hypointensity in T1 weighted image and hyperintensity in T2 weighted image. “Fluid sign” was visible at the L2 vertebra [Figure 2]. A small area of altered signal intensity was noted along the left psoas muscle. Hematological and biochemical parameters were within normal limits and were not suggestive of infection or malignancy.
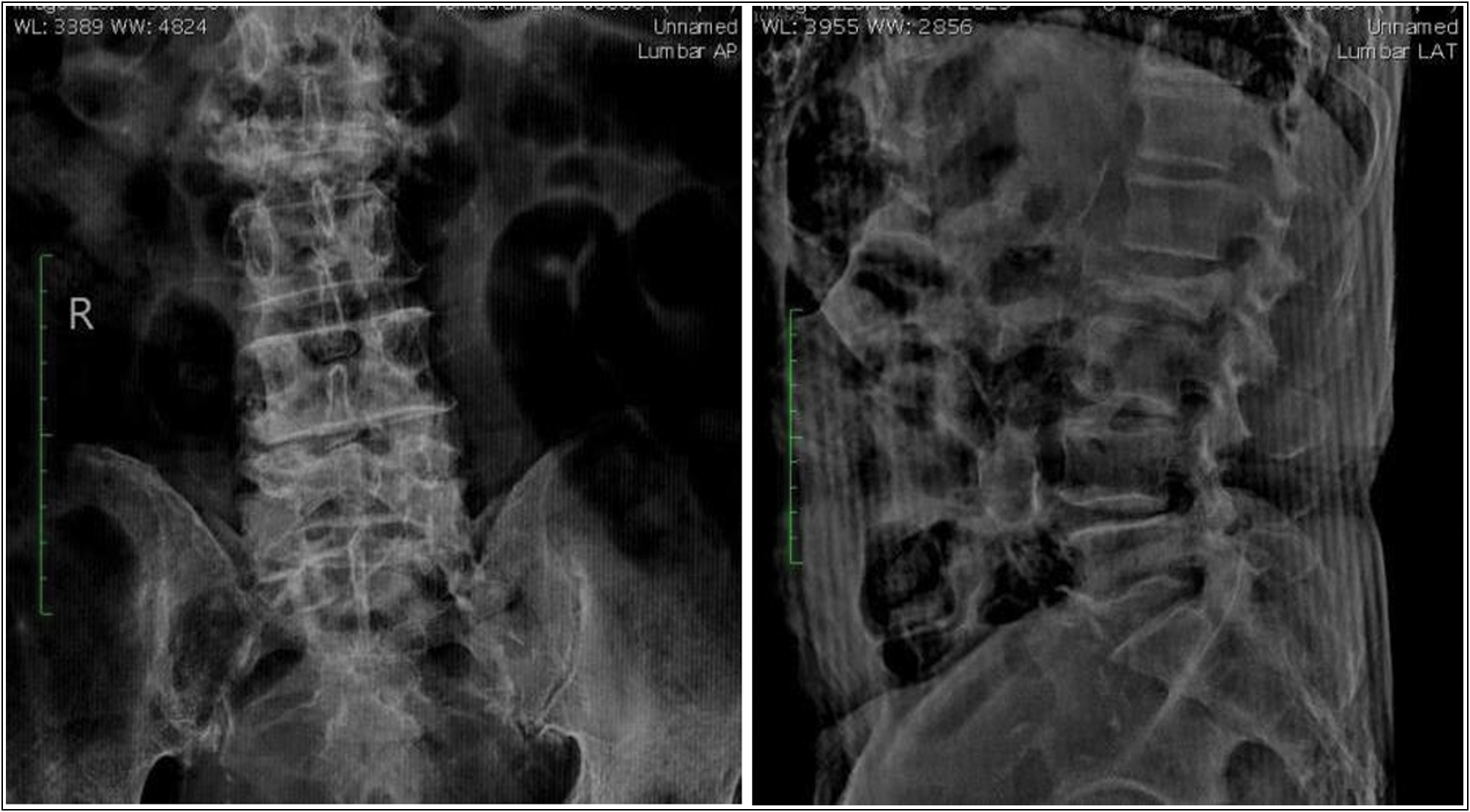
- Plain radiograph showing fractured L2 vertebra
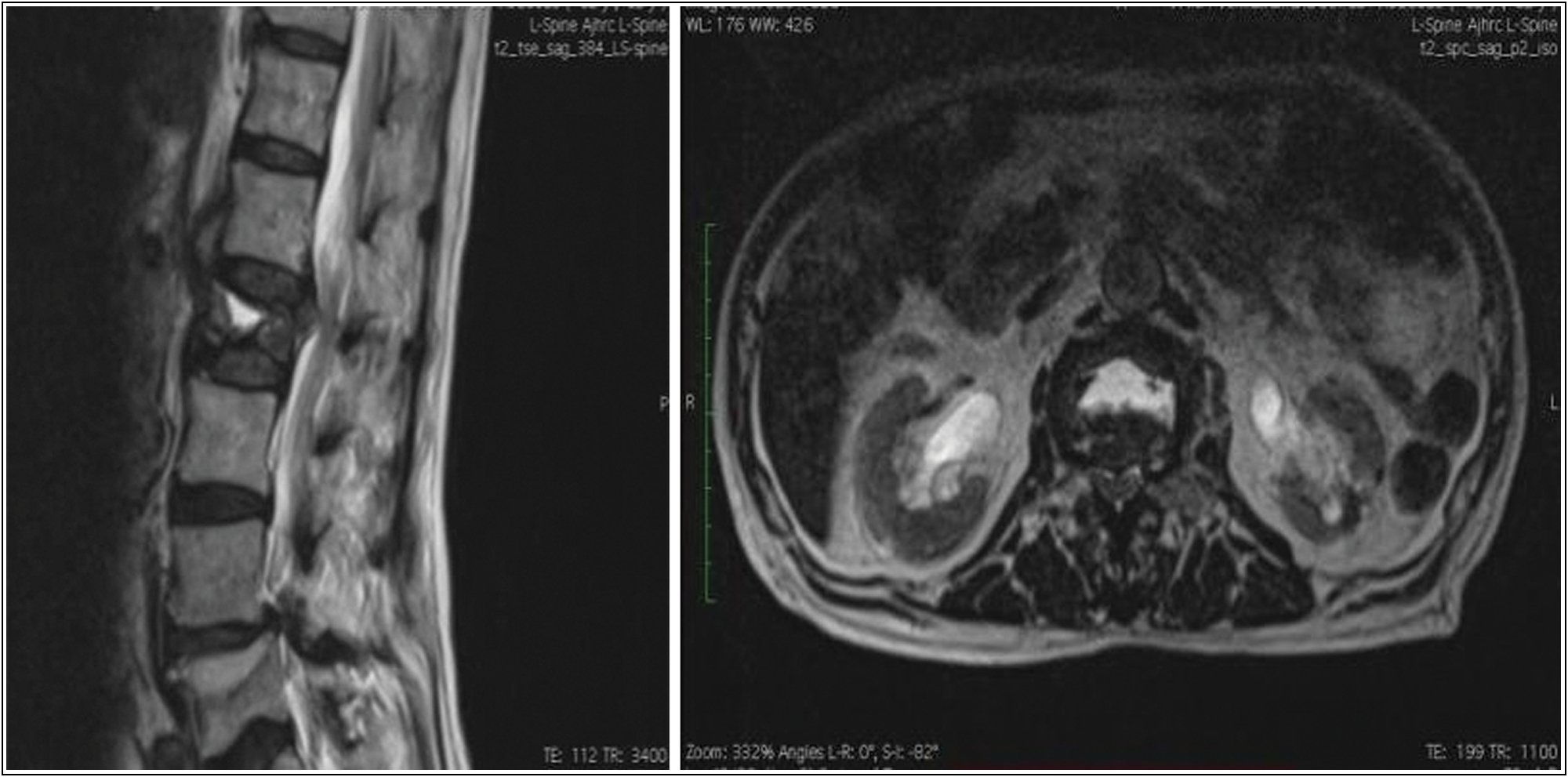
- “Fluid sign” seen in L2 vertebra on T2 weighted MRI images
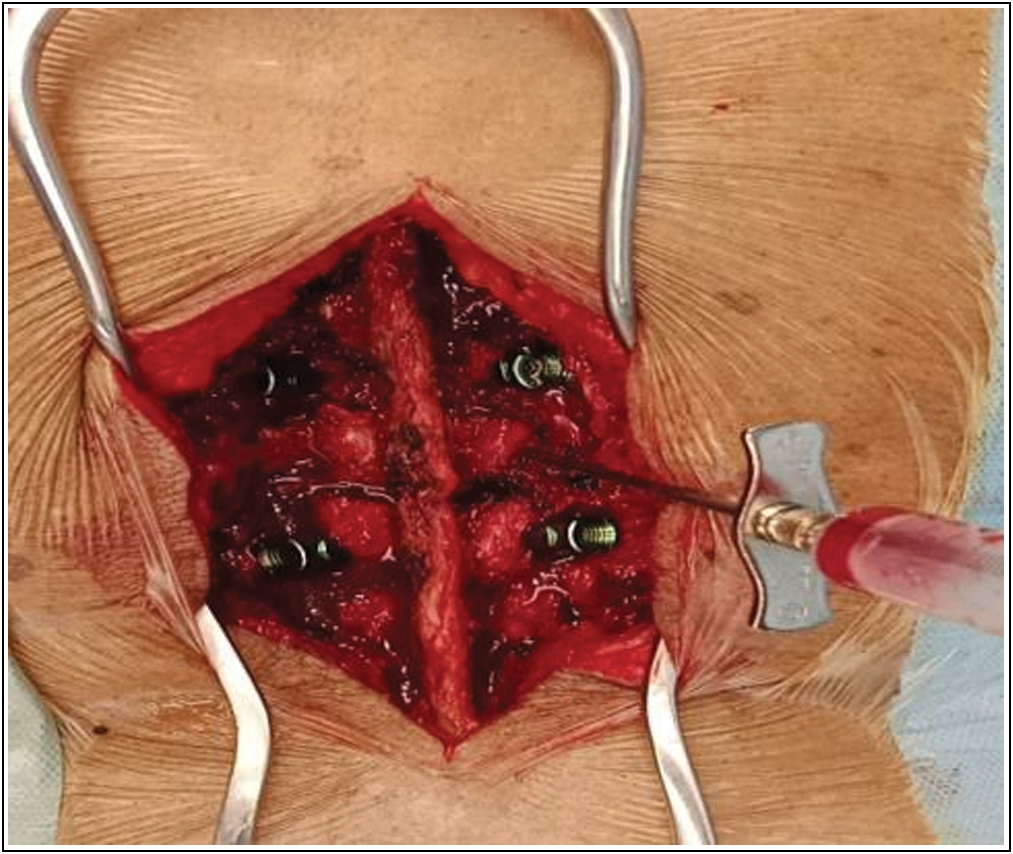
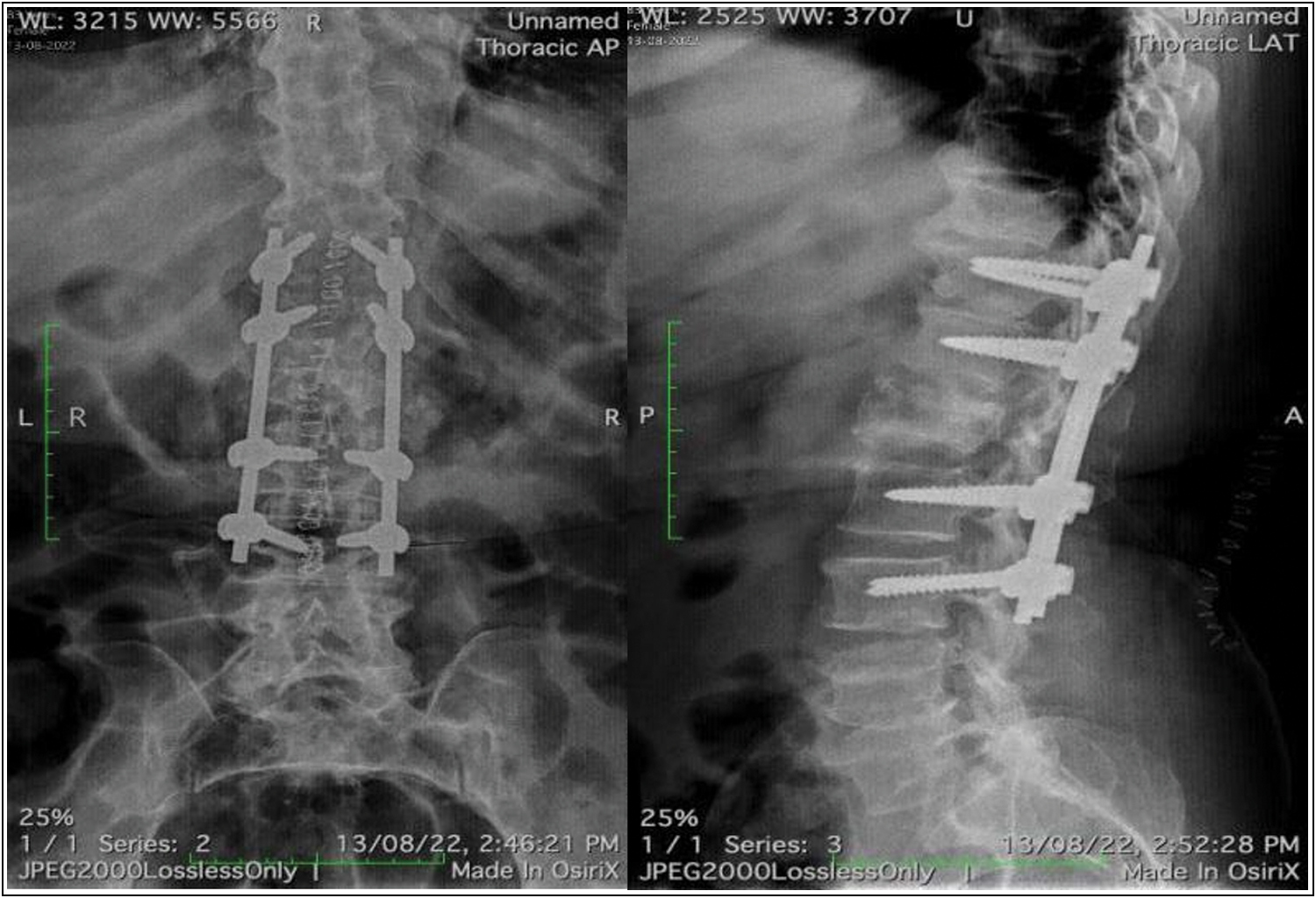
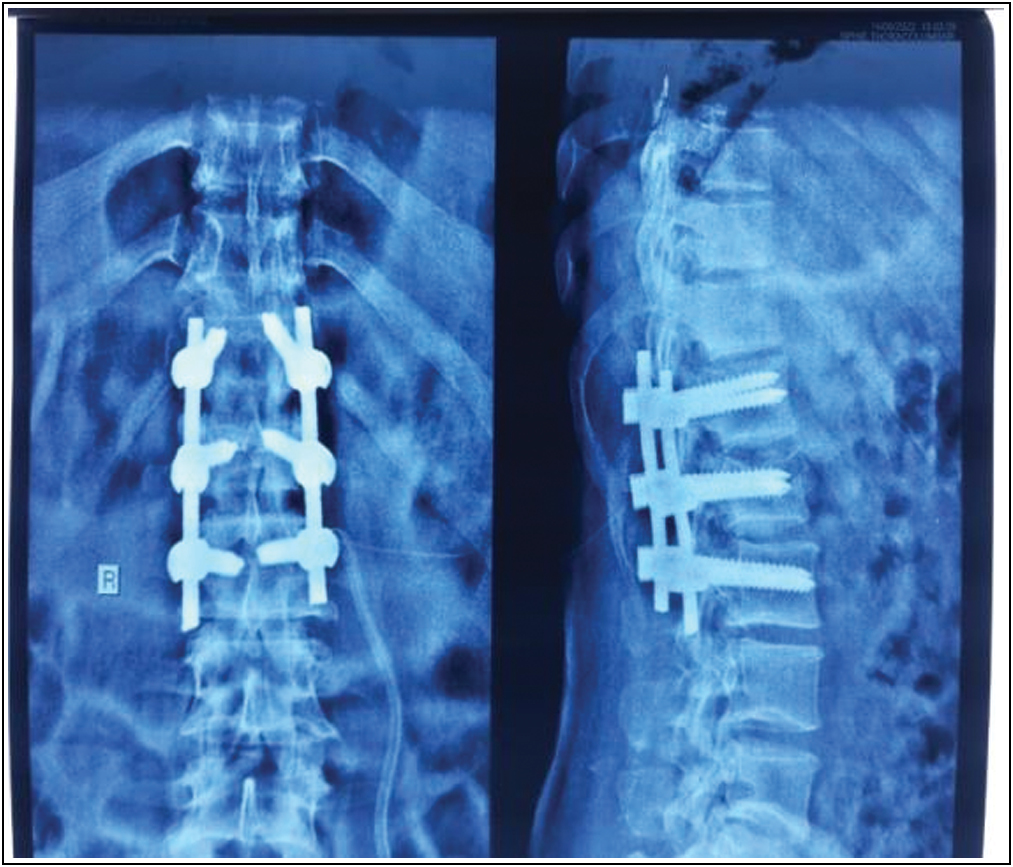
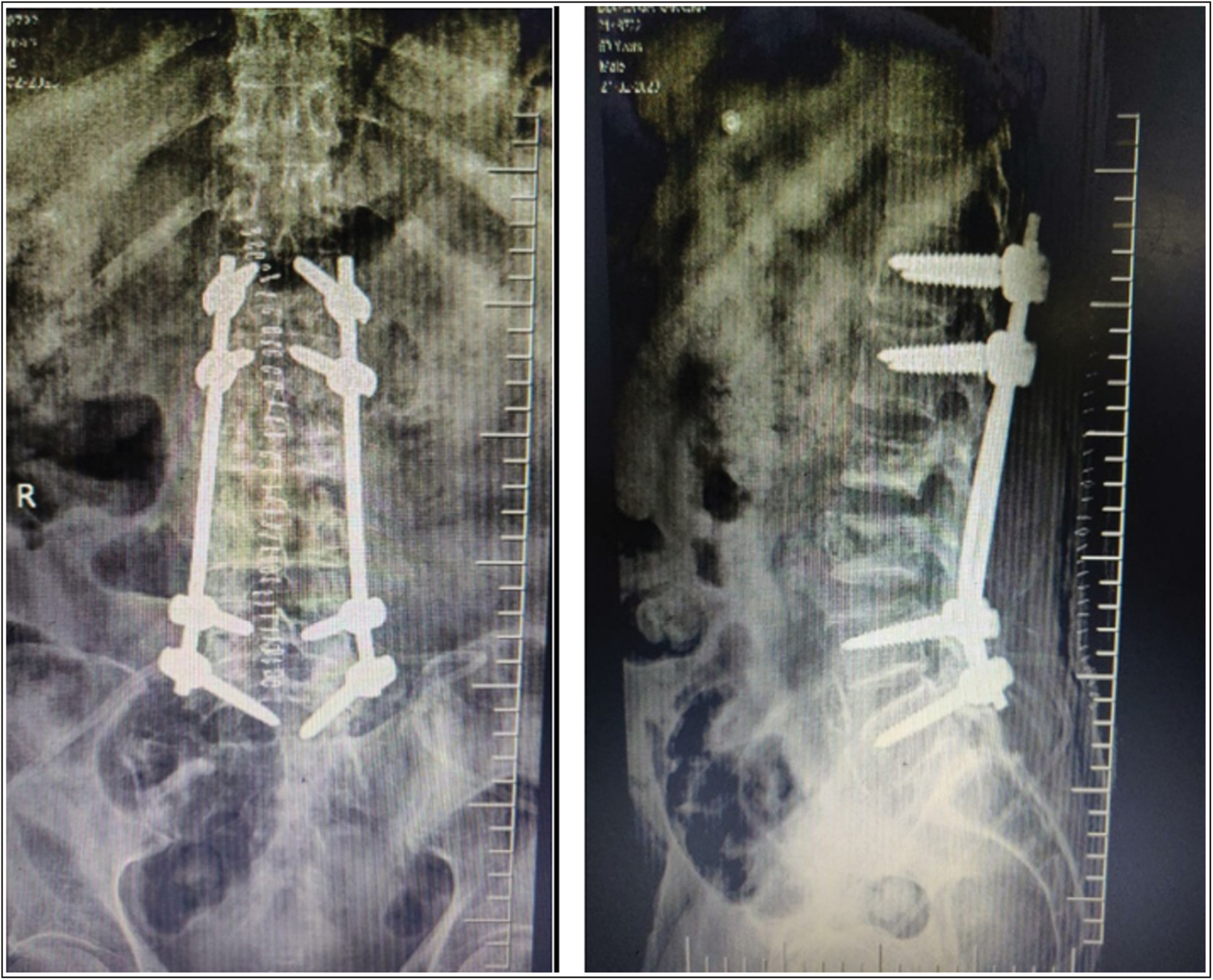
As the pain was severe and affected the mobility of the patient, aspirated fluid from L2 vertebrae which was later sent for culture [Figure 3] and then performed T12-L4 posterior stabilization with L2 transpedicular biopsy [Figures 4 and 5].

- Intra-operative image
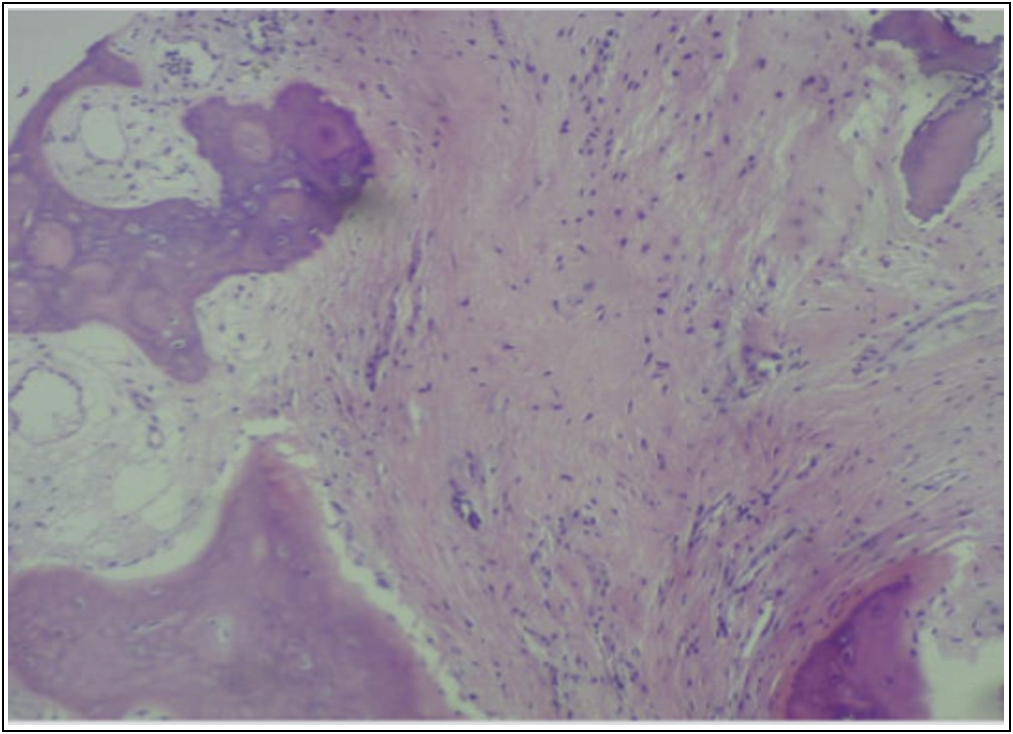
- Bony trabeculae seen with foci showing sample being collected of fibrosis on histopathology from L2 vertebra
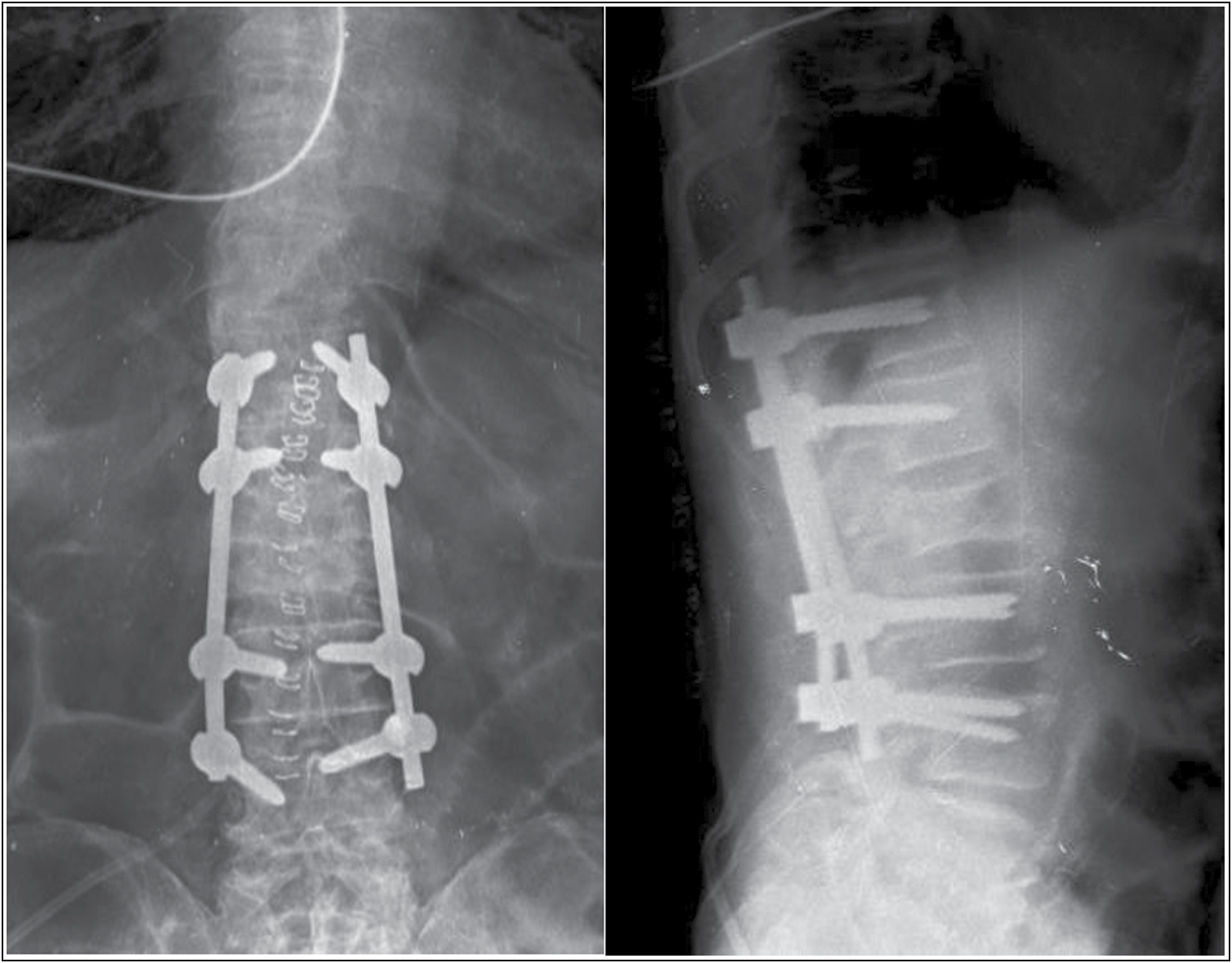
- Restored height of L2 vertebra, following T12-L4 posterior instrumented stabilization
Postsurgery there was significant pain relief and correction of kyphotic deformity. The patient was mobilized the next day with a Lumbar corset and was discharged with anti-osteoporotic medication. At 6 weeks follow-up, the patient was symptomatically better and is on walker-assisted mobilization. Culture after 6 weeks came negative for tuberculosis and fungus.
Case 2
An 83-year-old female patient presented with complaints of a non-radiating type of low back pain. There was history of multiple episodes of trivial falls and after the latest fall, that is, 1 month back, patient had been bedridden.
Her history is consistent with diabetes and hypertension.
On examination, there was no kyphosis and there were no neurological deficits.
AP and lateral radiographs showed a compression fracture of the L1 vertebra [Figure 6]. T2 weighted MRI showed “fluid cleft sign” of the L1 vertebra [Figure 7].
- AP and lateral radiograph showing L1 vertebra fracture with “vacuum cleft” inside body of L1 vertebra
- T2 weighted MRI showing “fluid sign” in L1 vertebra
The patient was managed with L1 transpedicular aspiration of fluid along with biopsy and T11-L3 posterior instrumented stabilization [Figures 8 and 9].
- Intra-operative image showing aspiration of fluid from L1 vertebra
- Post-operative radiograph after T11-L3 posterior instrumented stabilization
Immediately after the surgery, the patient’s pain improved and 2 days later she started walker-assisted mobilization.
Case 3
A 65-year-old male patient presented with complaints of low back pain, non-radiating type for 2 months. The patient gave a history of slip and fall 2 months back.
The patient had no known comorbidities.
On examination, there was tenderness over the lumbar spine and no motor or sensory deficits in bilateral lower limbs.
AP and lateral radiographs showed a compression fracture of L1 vertebra. T2 weighted MRI showed hyper intensity in the region of L1 vertebra [Figure 10].
- T2 weighted MRI images showing edema at L1 vertebra
The patient was managed with L1 transpedicular biopsy and T11-L3 posterior instrumented stabilization [Figure 11].
- Radiograph showing T11-L3 posterior instrumented stabilization after 6 weeks follow-up
The patient started walker-assisted mobilization 2 days after surgery. After a follow-up of 6 weeks, the patient is pain-free and is on walker-assisted mobilization.
Case 4
A 66-year-old female patient came with complaints of non-radiating type of low back pain after a history of slip and fall 15 days back. After which the patient went to a local hospital where she was diagnosed to have L1 vertebra fracture which was managed conservatively with a Taylor brace. The patent had a history of left hemiplegia 15 years back which was treated with local medicine and she is also a known case of hypertension.
On examination, there was tenderness over lumbar vertebra and motor weakness of 4/5 over the left side of the body. Reflexes over the left side were exaggerated.
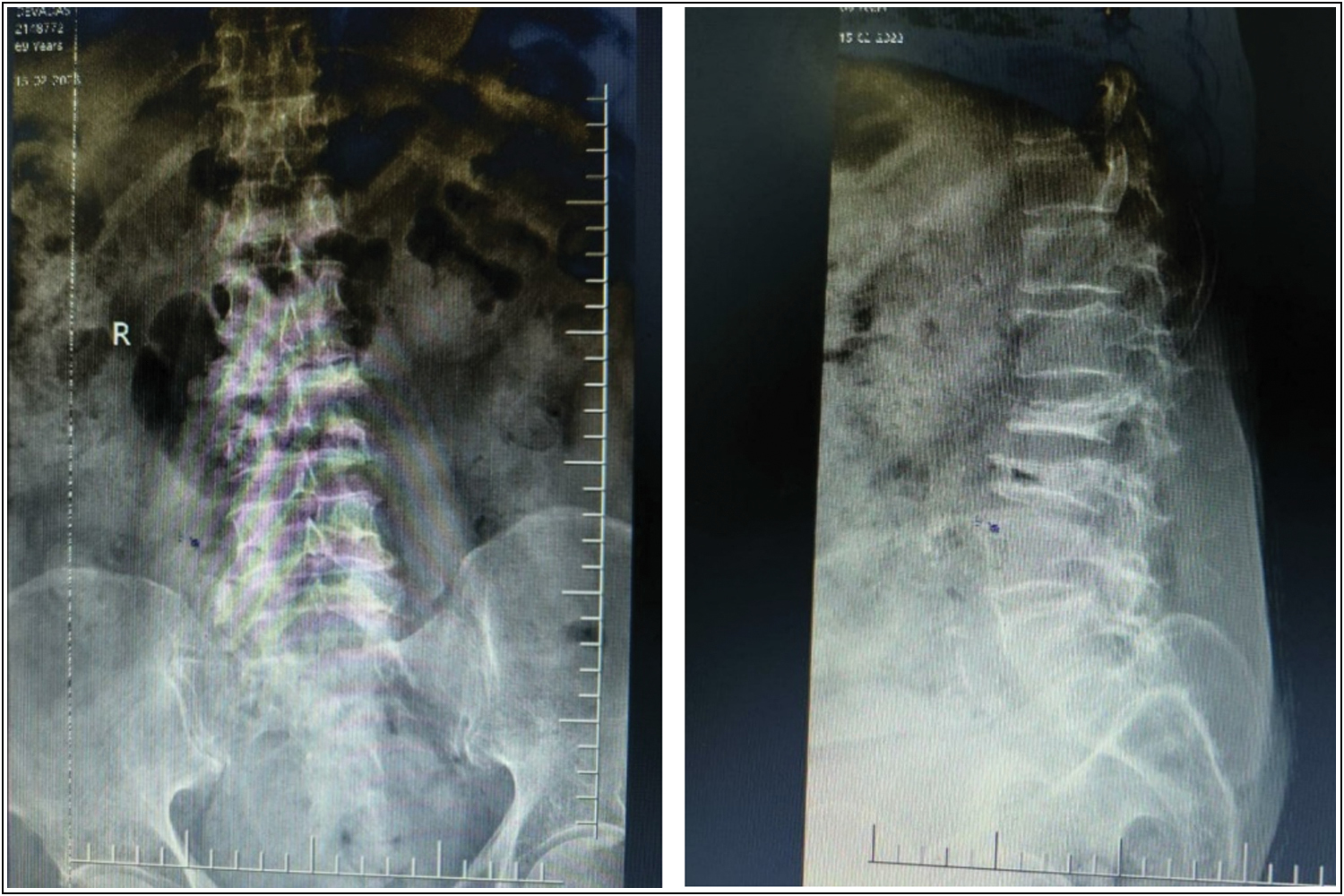
Radiographs showed osteoporotic compression fracture of D12 and L1 vertebrae [Figure 12]. T1 weighted MRI showed hypointensity over D12 and L1 vertebrae. T2 weighted MRI showed hyperintensity over D12 and L1 vertebrae. There was lumbarization of S1 seen on MRI [Figure 13].

- Plain radiographs showing fracture of D12 and L1 vertebra. “Vacuum cleft” sign visualized over L2 vertebra
- “Fluid sign” seen in L1 vertebra on T2 weighted MRI
The patient was managed with D10 to L3 posterior instrumented stabilization and T12 transpedicular biopsy and aspiration of fluid from L1 [Figure 14].

- Post-operative radiograph after D10 to L3 posterior instrumented stabilization
Immediately after the surgery, the patient’s pain reduced and was started on walker-assisted mobilization. After 6 weeks of follow-up, the patient is without discomfort or complaints [Figure 15].

- AP and lateral radiograph taken after 6 weeks of follow-up
Case 5
A 69-year-old male patient presented with complaints of low back pain, non-radiating type for 1 month. The patient gave a history of slip and fall 1 month back. The patient had been bedridden for 1 month.
On examination, there was tenderness over the lumbar spine and no motor or sensory deficits in bilateral lower limbs. The patient did have mild kyphotic deformity of spine proximal to fracture segment.
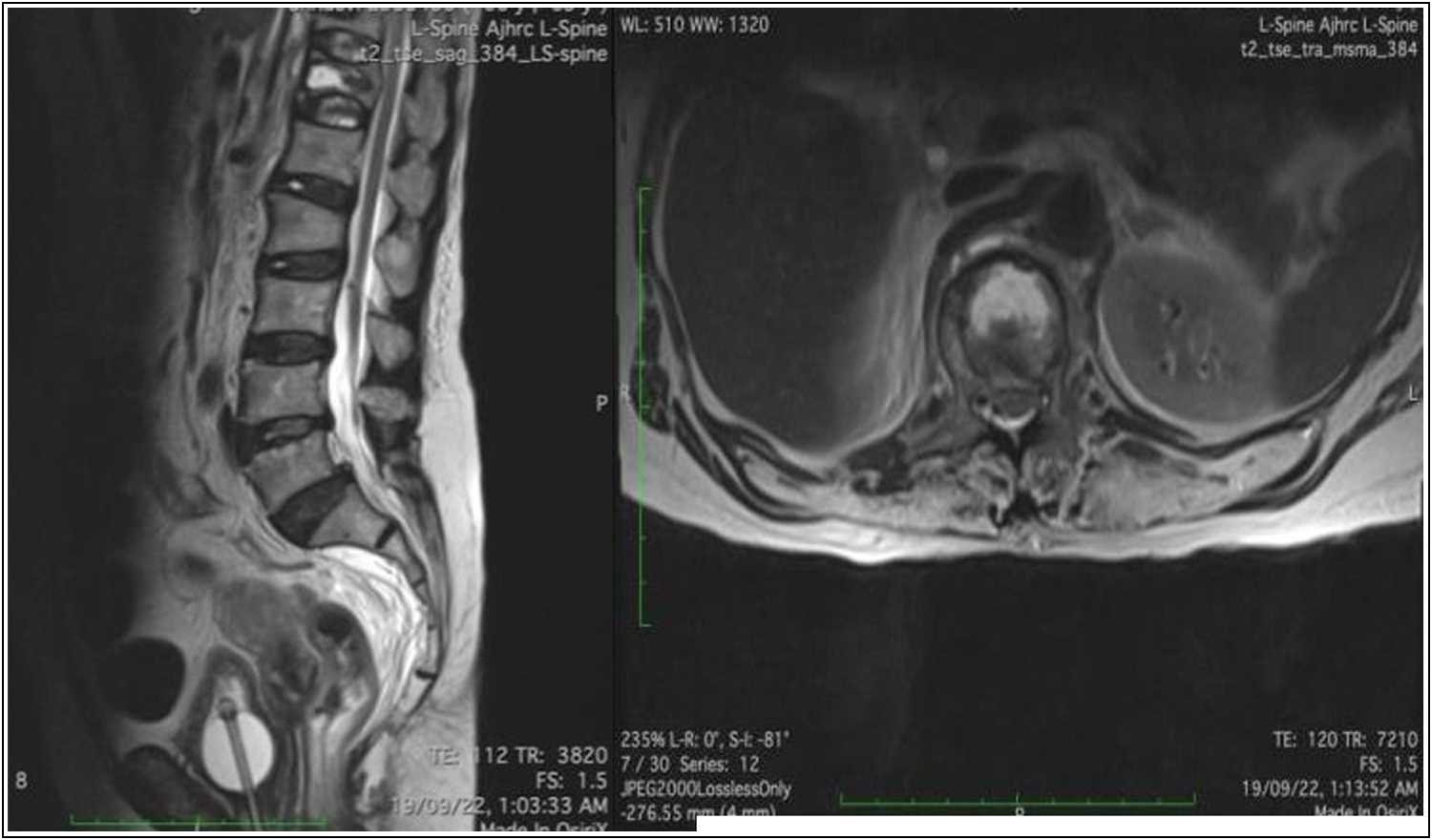
AP and lateral radiographs showed a compression fracture of L2 and L3 vertebra [Figure 16]. T2 weighted MRI showed hypointensity in the region of L2 vertebra and “Fluid sign” was noted over L3 vertebra [Figure 17].
- AP and lateral radiograph showing L2 and L3 compression fracture
- “Fluid sign” noted over L3 vertebra on T2 weighted MRI
The patient was managed with L2 transpedicular aspiration of fluid along with biopsy and T12-L5 posterior instrumented stabilization [Figure 18]. All necessary investigations were sent and the patient was diagnosed with Kummell’s disease by exclusion. The patient was started on walker-assisted mobilization from post-op day 2.
- T12 to L5 posterior instrumented stabilization
Discussion
This disease was first described by Schede[2,3] in 1881. He described the condition as a gradual weakening of the vertebral body that was followed by the development of an angular kyphosis.
Kümmell[2,4] outlined a clinical condition characterized by minimal spinal injuries, a brief, indeterminate asymptomatic phase and then a symptomatic increasing angular kyphosis.
Schmorl[5] revealed autopsy evidence in support of Kummell’s account. The vertebral body’s spongiosa were damaged, which led to collapse and gibbus development. No evidence of an underlying pathogenic process was found.
Lichtenstein,[6] claimed that after the first trauma, there is a vasomotor reflex spasm that causes damage to one or more bones. This is followed by a loss of neurovascular tone, chronic vasodilation, and fast vascular resorption of bone as a result.
Jaffe[7] suggested that although it could not be observed on a radiograph, a linear fracture may have been present at the time of the event. He suggested that the vertebral collapse may have been caused by a second, minor trauma to this area.
Steel[8] categorized KD into five stages in 1951 based on clinical characteristics:
Stage 1: Primary injury with normal radiograph.
Stage 2: Asymptomatic phase with episodes of back pain.
Stage 3: Asymptomatic for few months to years.
Stage 4: Recurrence and progression of pain at fracture level.
Stage 5: Stage with kyphosis and neurological deficits.
Patients who have Kummell’s disease tend to be middle-aged or older, with male predominance.[8]
There is frequently a history of minor trauma, which results in mild pain that has little impact on the patient’s everyday activities. The patient remains asymptomatic for several weeks to months before experiencing pain that is worse than the first episode. Slowly, the patient develops a kyphotic deformity and neurological symptoms that rarely affect bowel and bladder control.
The “intraosseous vacuum cleft” was one of the specific radiographic changes that Maldague et al.[9] used to identify the ischemic nature of the underlying disease process.
According to Jang et al.,[10] two radiologic signs of avascular necrosis of a vertebral body are the intravertebral vacuum phenomena and fluid build-up, as well as a collapsed vertebra. Because of intravertebral pseudoarthrosis, this disease can occasionally produce dynamic instability.
An MRI examination shows isolated fluid collections that are relatively hypointense on T1-weighted sequences and noticeably hyperintense on T2-weighted images in the vicinity of the vacuum cleft and trabecular damage.[11] When osteomyelitis and malignant tumor are present, the high signal intensity on T2-weighted sequences is more diffuse and less intense than when avascular necrosis is present.[12,13]
All five of the patients in our case series complained of excruciating back pain and were unable to walk. Cases 1 and 5 exhibited a mild kyphotic deformity of the spine secondary to compression at fracture. Case 1 also had L5 myotome motor weakness. Because of a history of hemiplegia, Case 4 had power of 4/5 (MMRC) over her left upper and lower limbs. Cases 1 and 2 had mild fluid accumulation in the psoas muscle on the MRI, which led to the differential diagnosis of Tuberculosis of spine.
Four patients were managed with posterior instrumented stabilization using long construct and 1 patient with 3 level construct. Transpedicular aspiration of fluid along with biopsy was done following stabilization. Intra-operative samples were sent for histopathological study and culture and sensitivity.
Diagnosis of Kummell’s was made after excluding differential diagnosis such as Spondylodiscitis, Metastasis, Chronic granulomatous diseases. All patients were given bisphosphonates prior to discharge from hospital.
The severity of the pain, the existence of neurological abnormalities, comorbidities, the amount of the kyphotic deformity and the quality of the bones should all be taken into account when selecting a treatment strategy.[14,15]
Minimally invasive techniques, including vertebroplasty, are appealing and successful options for treating acute vertebral collapse with back pain and allow early mobilization.[16]
Deng et al.[17] in a 5-year follow-up period discovered that transpedicular intracorporeal cement augmentation and short segmental posterior instrumentation could not effectively provide long-term stability and extended alleviation of back pain.
For Kummell’s disease with compromised canal function and neurological sequelae, decompression with instrumentation and fusion has historically been an option. When decompression is performed solely, as with laminectomy, there is a chance that the kyphotic deformity will progress and cause new problems.
Decompression can be made either anteriorly or posteriorly. In order to reduce the danger of entering the thoracic cavity or the retroperitoneal space, it would also be desirable to do an exclusively posterior instrumentation in a patient group where age and comorbidities may be significant.
In our study, 2 days after surgery patients were able to walk with the help of a walker after experiencing a considerable reduction in pain. Aspiration of fluid from diseased vertebrae also helped in decreasing nerve root irritation as seen in case 1. It also helped in better healing of fracture. After 6 weeks of follow-up, all five patients are pain-free and are on walker-assisted mobilization.
Strengths of this case series are as follows: although there are many case reports, this is the first case series where posterior instrumented stabilization with a long construct and transpedicular biopsy is used to treat Kummell’s disease. Second, we found the above management provides good outcomes in terms of pain relief and post-operative rehabilitation.
Few of limitations are: first, we have not included patients with significant kyphotic deformity secondary to Kummell’s disease. Second, this series does not compare two treatment modalities. Third, substantial numbers of patients were not included, which may be a source of biased results.
Conclusion
In conclusion, this is the first case series discussing the treatment of Kummell’s disease with posterior instrumented stabilization with a long construct and transpedicular aspiration of fluid along biopsy. We found that posterior instrumented stabilization offered good patient-related outcomes in terms of pain and post-operative rehabilitation on short-term follow-up. Kummell’s disease is overlooked on X-ray when patient presents at an early stage and hence a thorough knowledge of Kummell’s disease is required for the early treatment of these patients and prevention of complications.
Informed consent
The informed consent was obtained from patients to publish the information, including pre-operative, intra-operative and post-operative photographs.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Financial support and sponsorship
Nil.
Acknowledgement
The authors are grateful to Dr Dheeraj Kumar V, Associate professor, Department of Orthopedics, A J Institute of Medical Sciences and Research Centre for the support.
Conflicts of interest
There are no conflicts of interest.
References
- Die posttraumatische Wirbelerkrankung (Kümmellsche Krankheit) Arch F Klin Chir. 1921;18:876-901.
- [Google Scholar]
- Wirbelfraktur durch Muskelzug. Bericht iiber die Verhandlungen des Deutschen Ger. F. Chirurgie x. Kongress 1881. Zentralbl. f. Cbir. 1881
- [Google Scholar]
- Die rarefizierende ostitis der wirbelkörper. Deutsche Med. 1895;21:180-1.
- [CrossRef] [Google Scholar]
- The Human Spine in Health and Disease 1971:xi-504.
- Disease of Bone and Joints. St. Louis: CV Mosby Co; 1975.
- Metabolic, Degenerative, and Inflammatory Diseases of Bones and Joints. Philadelphia: Lea and Febiger; 1972. p. :621.
- The intravertebral vacuum cleft: A sign of ischemic vertebral collapse. Radiology. 1978;129:23-9.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of percutaneous vertebroplasty in the treatment of intravertebral pseudarthrosis associated with noninfected avascular necrosis of the vertebral body. Spine. 2003;28:1588-92.
- [CrossRef] [PubMed] [Google Scholar]
- Vertebral fluid collection associated with vertebral collapse. Am J Roentgenol. 1996;167:1535-8.
- [CrossRef] [PubMed] [Google Scholar]
- Magnetic resonance imaging in the evaluation of patients for percutaneous vertebroplasty. Top Magn Reson Imag. 2000;11:235-44.
- [CrossRef] [PubMed] [Google Scholar]
- Kummell’s disease: Delayed post-traumatic osteonecrosis of the vertebral body. Eur Spine J. 2010;19:1065-70.
- [CrossRef] [PubMed] [Google Scholar]
- Kümmell’s disease: A case report and literature review. Spine. 2008;33:E152-5.
- [CrossRef] [PubMed] [Google Scholar]
- Kümmell’s disease, an uncommon and complicated spinal disorder: A review. J Int Med Res. 2012;40:406-14.
- [CrossRef] [PubMed] [Google Scholar]
- Kummell’s disease: Delayed post-traumatic osteonecrosis of the vertebral body. Eur Spine J. 2010;19:1065-70.
- [CrossRef] [PubMed] [Google Scholar]
- Therapeutic efficacy of transpedicular intracorporeal cement augmentation with short segmental posterior instrumentation in treating osteonecrosis of the vertebral body: A retrospective case series with a minimum 5 year follow-up. BMC Musculoskelet Disord. 2019;20:1-7.
- [CrossRef] [PubMed] [Google Scholar]




