
Translate this page into:
Is dislocation rate higher in total hip arthroplasty done for acute displaced fracture neck of femur?
Address for correspondence: Dr. Ganesan Ram Ganesan, Department of Orthopaedics, B2, Sri Ramachandra Medical Centre, Porur, Chennai - 600 116, Tamil Nadu, India. E-mail: ganesangram@yahoo.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Ganesan GR, Varthi VP. Is dislocation rate higher in total hip arthroplasty done for acute displaced fracture neck of femur?. J Orthop Allied Sci 2015;3:59-62.
Abstract
Background
Hip replacement has transformed the lives of hundreds of thousands of people regardless of the underlying aetiology. Debate about the role of arthroplasty for an acute displaced femoral neck fracture has been ongoing for decades. In this article we are going to evaluate whether dislocation rate is higher in total hip replacement done for acute displaced fracture neck of femur.
Materials and Methods:
Retrospective study of sixty two patients who underwent total hip replacement in Sri Ramachandra medical center. The minimum follow-up was taken as 5 years. Patients were divided into two group; traumatic and non traumatic group. We had 38 patient who underwent hip replacement for non traumatic indications. Traumatic group had 24 patients. The inclusion criteria for the traumatic group were acute displaced fracture neck of femur above 50 years and fracture neck with fracture head with dislocation above 50 years. We used the Harris hip score (Modified) for clinical and functional evaluation.
Results:
We had 89% excellent/good results in non traumatic group 75% excellent/good result in traumatic group. We had one dislocation in non-traumatic group and four dislocations in traumatic group.
Conclusions:
There is an increase rate of dislocation in patient who underwent total hip replacement for a traumatic condition when compared to their non traumatic counterpart.
Keywords
Dislocation
fracture neck of femur
posterior approach
total hip replacement

Introduction
Total hip replacement is one of the most successful and cost-effective interventions in medicine.[1,2] Hip replacements has transformed the lives of hundreds of thousands of people regardless of the underlying etiology.[3] Total hip arthroplasty is often indicated to relieve pain and increase range of motion in patients with arthritis and other collagen diseases.[4] Debate about the role of arthroplasty for an acute displaced femoral neck fracture has been ongoing for decades.[5] Although there is little doubt that arthroplasty is appropriate treatment for many patients with a displaced femoral neck fracture, there is ongoing controversy about the relative merits of different types of arthroplasty among specific groups of patients. In this article we are going to evaluate whether dislocation rate is higher in total hip replacement done for acute displaced fracture neck of femur.
Materials and Methods
Retrospective study of 62 patients who underwent total hip replacement in Sri Ramachandra medical center. The minimum follow-up was taken as 5 years. Patients were divided into two group's traumatic and non traumatic group. We had 38 patients who underwent hip replacement for non-traumatic indications like avascular necrosis of femoral head (14), rheumatoid arthritis (nine), ankylosing spondylitis (two) and osteoarthritis (13). Traumatic group had 24 patients. The inclusion criteria for the traumatic group were acute displaced fracture neck of femur above 50 years and fracture neck with fracture head with dislocation above 50 years. The exclusion criteria were nonunion fracture neck of femur, failed cancellous screw Fixation, intertrochantric fractures and assosciated acetabulum fractures. We had twelve patients with garden type III fracture, ten patients with garden type IV fracture and two patients with neck of femur fracture with head of femur fracture. We did the uncemented hip replacement in males below 60 yrs and females below 55 yrs of age.[6] However the cemented hip replacement was used in patients for whom economy was a constraint. All patients underwent surgery by posterior approach only. Informed consent was obtained from patients after discussion of the advantages and risks.
We used the Harris hip score[7] (Modified) for clinical and functional evaluation and plain X-ray pelvis with both hips and proximal femur—AP view and X-ray of the operated hip lateral view for radiological evaluation. The Andrew Whaley and Daniel et al., criteria[8] for uncemented cups and the De Lee and Charnley criteria for cemented cups were used to assess cup loosening. The Gruen zones[9] for cemented stems and the Enghs criteria for uncemented stems were used to assess femoral stem loosening. Other radiological components that were taken into consideration were cup inclination, femoral stem position, vertical subsidence of femoral component, vertical migration of acetabular component and heterotrophic ossification. The Brookers Classification[10] was used to assess Heterotropic Ossification.
Results
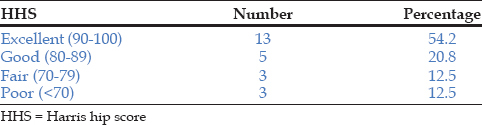
We had 89% excellent/good results in non traumatic group 75% excellent/good result in traumatic group as per Tables 1 and 2 respectively.

Complication
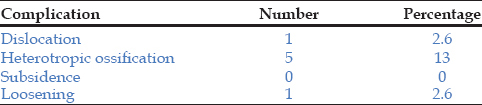
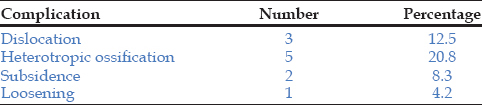
In non traumatic group [Table 3] we had a dislocation rate of 2.6% (one hip), 2.6% incidence of aseptic acetabular loosening (one hip), 16% incidence of anterior thigh pain (6 patients) and a 13% incidence of heterotrophic ossification (five hips). In traumatic group [Table 4] we had 4 (16.6%) dislocation, 5 (20.8%) heterotopic ossification. Loosening of acetabulum was observed in one (4.2%) patient and two (8.3%) patients had subsidence. We had no infection in our series.
Discussion
Total hip arthroplasty is an operation to restore motion and stability to a joint and function to the muscle, ligaments and other soft tissue structures that control the joint. Implanting an artificial head and socket to replace the degenerated head, fractured head exerted such a profound social impact and enjoyed such a dramatic early success. Various immediate and long term complications may compromise this procedure, but it still remains the greatest boon available to orthopedic patients, and has proved to be the greatest advancement in the field of orthopaedic surgery in the twenty first century. There are many controversial topics surrounding total hip arthroplasty including replacement for traumatic condition like acute facture neck of femur.
Total hip replacement itself is a procedure riddled with a large number of long-term complications ranging from dislocations including recurrent dislocations. Primary endoprosthetic replacement has been advocated to improve survival by eliminating fracture fixation and healing problems and by allowing early mobilization. Conventional treatment for fracture neck of femur, grade 1 and 2, is open reduction and internal fixation, whereas, that for grade 3 and 4 is still controversial.
In non-traumatic group on analysing the difference in pre operative and latest Harris hip score for various indications, our study showed no difference in gain of harris hip score for various indication like avascular necrosis, osteoarthritis and rheumatoid arthritis. Our series of patient with osteoarthritis have pre and latest Harris hip score as 49 and 92. It is evident from Tables 1 and 2 that functional outcome of total hip replacement for patient in non traumatic group had better outcome than the traumatic one.
In non traumatic group we had one case of dislocation (2.6%). The dislocation occurred during the first month of the surgery at home. For this patient the cup was placed vertically and posterior approach was used. The patient was treated by open reduction and trochantric osteotomy. The study of Wayne M. Goldstein et al.,[11] which shows a increased rate of dislocation following posterior approach. His study shows dislocation rate of 2.8% following posterior approach which is correlating with our study. Charlotte B. Philips et al.,[12] study shows a dislocation rate of 3.9%. The incidence of dislocation were highest during the immediate post-operative period but remain elevated throughout the first three post operative months.
In traumatic group we had four case of dislocation. One patient had a fall from height 1.5 years after the surgery leading to dislocation. Hence, this patient is being excluded from this part of the discussion. Out of the remaining three patients, one had a dislocation within 3 days of surgery and the other had a dislocation on the twelfth post-op day and other within 3 weeks following the surgery. Studies have shown that total hip arthroplasty done for fracture neck of femur has a higher dislocation rate than total hip arthroplasty done for other causes Yuan et al.[13] In our study the dislocations occurred within a month after surgery. This concurs with the findings of others which have reported a higher rate of dislocations in the first month following surgery.
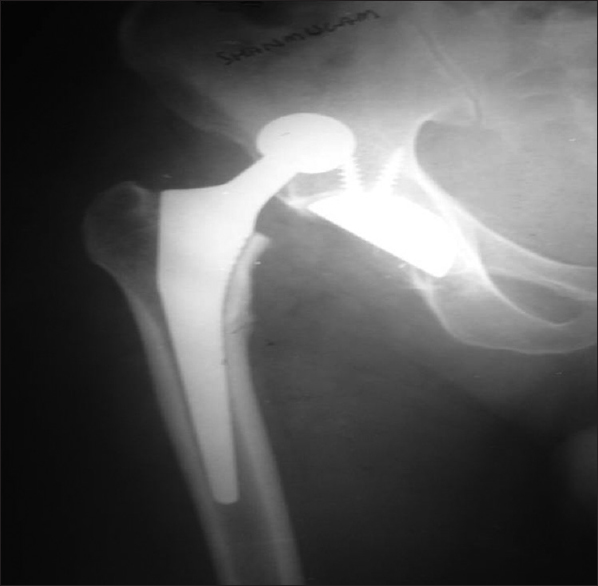
One of the patients' who had dislocation after 12 days was a psychiatric patient, suffering from alcohol withdrawal and was non compliant [Figures 1-3]. He tried to lie in prone position and dislocated his hip. In the second and third patient the cause of dislocation was unknown. The fourth patient had a fall from height after 1.5 years resulting in dislocation [Figures 4-6]. All the four patients were managed by open reduction and kept on abduction splint for 6 weeks. Khan et al.,[14] in his study found that the incidence of dislocated prosthetic hip could be reduced by greater attention to certain details of patient selection and technique of insertion. Factors predisposing to dislocation include mentally confused patient, uncontrolled epileptic and weakness of hip muscles due to neurological disorder and previous operation of the hip. Sixty-nine patients who dislocated, the precipitating cause were rotation combined with flexion and extension (bending to cut toe nails, leaning forward from sitting position etc). In 10 cases trauma was the cause and in 55 patients cause was unknown. Studies conducted by Yuan et al.,[13] Morreys[15] showed that smaller head size and posterior approach was the most common cause of dislocation. One of the dislocated patient had a small head size (22 mm). Our study concurs with that of Yuan et al., that posterior approach and small head size is associated with a higher dislocation rate.
- 12th post operative day

- Clinical picture posterior dislocation

- X ray following open reduction

- Fall from height

- Dislocated hip

- Following open reduction
Conclusion
There is an increase rate of dislocation in patient who underwent total hip replacement for a traumatic condition when compared to their non traumatic counterpart. Dislocation is multifactorial. Dislocation can be minimized by careful patient selection, adherence to postoperative protocol and use of a lateral approach with large head in susceptible patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Cost-effectiveness of total joint arthroplasty in osteoarthritis. Arthritis Rheum. 1986;29:937-43.
- [CrossRef] [PubMed] [Google Scholar]
- Functional improvement and costs of hip and knee arthroplasty in destructive rheumatoid arthritis. Scand J Rheumatol. 1991;20:351-7.
- [CrossRef] [PubMed] [Google Scholar]
- Total hip replacement: Indications for surgery and risk factors for failure. Ann Rheum Dis. 1997;56:455-7.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis of functional and radiological outcome of total hip replacements in rheumatoid and osteoarthritis patients. Open J Rheumatol Autoimmune Dis. 2013;3:246-50.
- [CrossRef] [Google Scholar]
- Optimal arthroplasty for femoral neck fractures: Is total hip arthroplasty the answer? J Orthop Trauma. 2009;23:428-33.
- [CrossRef] [PubMed] [Google Scholar]
- Total hip arthroplasty for primary osteoarthritis in patients fifty-five years of age or older. An analysis of the Finnish arthroplasty registry. J Bone Joint Surg Am. 2008;90:2160-70.
- [CrossRef] [PubMed] [Google Scholar]
- Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am. 1969;51:737-55.
- [CrossRef] [Google Scholar]
- Walking ability after total hip replacement. A comparison of gait analysis in unilateral and bilateral cases. J Bone Joint Surg Br. 1992;74:53-6.
- [CrossRef] [PubMed] [Google Scholar]
- Modes of failure of cemented stem-type femoral components: A radiographic analysis of loosening. Clin Orthop Relat Res. 1979;141:14-7.
- [CrossRef] [Google Scholar]
- Ectopic ossification following total hip replacement. Incidence and a method of classification. J Bone Joint Surg Am. 1973;55:1629-32.
- [CrossRef] [Google Scholar]
- Prevalence of dislocation after total hip arthroplasty through a poster lateral approach with partial capsulotomy and capsulorrhaphy. J Bone Joint Surg 2001:83.
- [CrossRef] [PubMed] [Google Scholar]
- Incidence rates of dislocation, pulmonary embolism, and deep infection during the first six months after elective total hip replacement. J Bone Joint Surg 2003:85.
- [CrossRef] [PubMed] [Google Scholar]
- Dislocation after total hip arthroplasty. Arch Orthop Trauma Surg. 1999;119:263-6.
- [CrossRef] [PubMed] [Google Scholar]
- Dislocation following total hip replacement. J Bone Joint Surg Br 1981:214-8.:63-8.
- [CrossRef] [PubMed] [Google Scholar]
- Instability after total hip arthroplasty. Orthop Clan North Am. 1992;23:237-48.
- [CrossRef] [PubMed] [Google Scholar]




