
Translate this page into:
Intraosseous ganglion of the talus with extension in the subtalar joint
Address for correspondence: Dr. Pulak Sharma, Department of Orthopaedics and Traumatology, Gandhi Medical College, Bhopal 462 001, Madhya Pradesh, India. E-mail: drpulaksharma@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Sharma P, Gohiya A, Jain S, Gaur S. Intraosseous ganglion of the talus with extension in the subtalar joint. J Orthop Allied Sci 2014;2:14-6.
Abstract
Intraosseous ganglion is a benign bony cyst that mainly involves the epiphysis and metaphysis of long bones. Intraosseous ganglions are rare in talus, and in all the cases reported in literature, the patients had symptoms pertaining to the ankle joint. No case has been reported where the lesion in the talus has caused symptoms specific to the subtalar joint. A 20-year-old female presented to our hospital with pain in the right foot from last 6 months. Ankle joint movements were within normal limits, but the subtalar movement were significantly reduced. Plain radiographs of the foot and ankle were normal. Computed tomography (CT) scan of the foot and ankle showed a cystic lesion (0.5 × 0.5 cm) involving the base of the talar body which communicated with the subtalar joint. The patient was treated by curettage of the lesion through a curvilinear incision over the medial aspect of the subtalar joint. The clinical results after 3 months were excellent. The patient returned to her regular and light recreational activities with full, painless range of motion. There was no recurrence of symptoms at 6 months. Intraosseous ganglion is of talus is a rare entity. Symptomatic patient should be treated surgically.
Keywords
Curettage
intraosseous ganglion
talus

Introduction
Intraosseous ganglion is a benign, bony cyst that mainly involves the epiphysis and metaphysis of long bones.[1] The wrist; the femoral head, medial malleolus, and carpal bones are the most common locations where these lesions have been reported.[2,3,4] These lesions become symptomatic in patients when they are located close to the neurovascular structures or articular surfaces. They present with pain, neurologic dysfunction, or articular fractures. In as many as 40% of patients they may be asymptomatic.[5] There are very few cases that have been reported in the talus. Intraosseous ganglions are rare in talus, and in all the cases the patient had symptoms pertaining to the ankle joint.[6,7,8,9] No case has been reported where the lesion in the talus has caused symptoms specific to the subtalar joint.
We report a rare case of intraosseous ganglion of the talus that presented with pain and discomfort pertaining to the subtalar joint. The patient was successfully treated with curettage of the lesion and was relieved of her symptoms.
Case Repor
A 20-year-old female presented to our hospital with pain in the right foot pain from last 6 months. The pain had been of mild to moderate intensity and located on the inner aspect of the foot, aggravated on activity and relieved on rest. She was able to do her daily activities but anything beyond that caused great discomfort. There was no history of any significant trauma or fever nor any history of similar complaint in any other joints.
On examination, she did not have any wasting of muscles, erythema, redness, or inflamation around her foot. Ankle joint movements were within normal limits, but the subtalar movement were significantly reduced. Also, her sensory and motor examinations were normal.
Plain radiographs of the foot and ankle were normal [Figure 1]. The patient was treated conservatively but had little benefit and so a CT scan of the foot and ankle was obtained which showed a cystic lesion (0.5 × 0.5 cm) involving the base of the talar body which communicated with the subtalar joint [Figure 2].

- X-ray of the patient
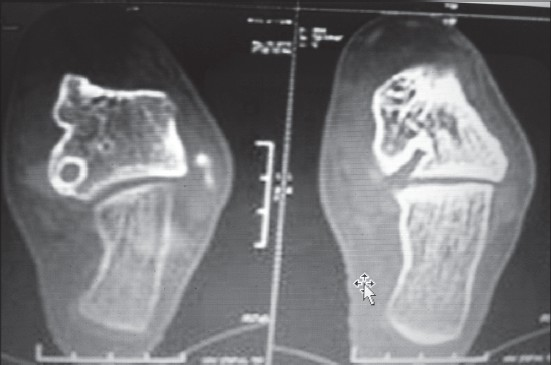
- Computed tomography scan showing a cystic lesion communicating with the subtalar joint
Because the cyst was symptomatic, it was decided to treat the patient surgically and also to take a biopsy of the lesion. Surgical exploration was performed using a 2 cm curvilinear incision over the medial aspect of the subtalar joint. The subtalar joint was opened. Upon opening the joint, thick gelanitous fluid was obtained which was collected for pathological examination. The cyst was identified and its walls were enlarged using appropriate-sized curets. Final placement of an angled curet enabled complete curettage of the lesion. Postoperatively the leg was placed in a removable cast splint for 10 days. There were no intraoperative or postoperative complications. Diagnosis of intraosseous ganglion was confirmed by means of pathological examination. Partial weight bearing was permitted 1 week after the splint was abandoned. Full weight bearing was started 1 month after the operation. The clinical results after 3 months were excellent. She was able to do all her activities without discomfort. There was no pain even on activities involving exertion. The patient returned to her regular and light recreational activities with full, painless range of motion. There was no recurrence of symptoms at 6 months.
Discussion
Soft tissue ganglia are commonly encountered in orthopedics, but their intraosseous counterparts have been less frequently been reported.[10] Intraosseous ganglion is a benign cystic tumor pathologically identical to its softtissue counterpart. Mean average age of presentation is 42 years.[11] The lesion is usually in close proximity to a joint, but rarely has any interaction with it. The contents of the cyst have a gelatinous consistency, and the cyst has a yellowish mucoid center.[12] Patients commonly present with intermittent pain that increases with activity. Asymptomatic intraosseous ganglia can erode the joint cartilage and thus invade a joint over time and become symptomatic.[7]
There are various theories behind the origin of intraosseous ganglion. Some scientists believe intramedullary metaplasia as a cause of intraosseous ganglion cyst.[1,13,14] Some others think it makes secondary to degeneration. Also, trauma was mentioned as one of probably etiology of intraosseous ganglion cyst.[14]
Radiographs show an eccentric intraosseous radiolucent lesion that should be differentiated from enchondroma, osteoarthritic cyst, posttraumatic cyst, osteoidosteoma, and osteoblastoma. The patient reported in here had no additional radiologic signs of osteoarthritis, and her age was inconsistent with that diagnosis. There was no history of trauma, a classic nidus, or reactive sclerosis that would indicate osteoid osteoma. CT imaging was used for differential diagnosis because it shows the intraosseous lesion and identifies any connection between the intraosseous lesion and the joint space and the presence of any pathologic fracture. In this patient, the cystic lesion was located in the subchondral region at the base of the talus with connections between the lesion and the subtalar joint space.
Intraosseous ganglions are extremely rare in talus. The preferred treatment of a large, symptomatic intraosseous ganglion is debridement of the cyst, drilling the cystic wall and the surrounding sclerotic bone, and filling the defect with an autologous bone graft.[3,6,7,8,12] However, bone grafting is not a necessary adjunct to the curettage of talar lesions.[15] There lesions in the talus can be approached by arthroscopy[6,7] and arthrotomy. The cartilage lesion has also been treated by transplantation of cultivated chondrocytes[7] after curettage.
This case is rare because an intraosseous ganglion is a very rare and above that in all the cases reported the ganglion had caused symptoms pertaining to the ankle joint.[6,7,8,9] No case has been reported in literature in which an intraosseous ganglion had caused symptoms related to the subtalar joint.
Conclusion
Intraosseous ganglion of talus is a rare entity. Symptomatic patient should be treated surgically. Surgical removal, curettage with or without bone graft insertion shows good clinical as well as radiological results. Intraosseous ganglion should always be considered as a differential diagnosis in a patient with persistent foot or ankle pain which is not being relieved on symptomatic treatment.
Source of Support:
Nil
Conflict of Interest:
None declared.
REFERENCES
- Juxta-articular bone cysts (intra-osseous ganglia): A clinicopathological study of eighty-eight cases. J Bone Joint Surg Br. 1979;61:107..
- [CrossRef] [PubMed] [Google Scholar]
- Ganglion cysts of the lower extremity: An analysis of 54 cases and review of the literature. Orthopedics. 1998;21:141-8.
- [CrossRef] [PubMed] [Google Scholar]
- Relationship between dorsal ganglion cysts of the wrist and intraosseous ganglion cysts of the carpal bones. Acta Orthop Belg. 2005;71:535-9.
- [Google Scholar]
- Intraosseous ganglion of the greater trochanter. Orthopedics. 1999;22:1089-90.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of a large intraosseous talar ganglion by means of hindfoot endoscopy. Arthroscopy. 2003;19:96-100.
- [CrossRef] [PubMed] [Google Scholar]
- Massive intraosseous ganglion of the talus: Reconstruction of the articular surface of the ankle joint. Arthroscopy. 2000;16:E14..
- [CrossRef] [PubMed] [Google Scholar]
- Intraosseous ganglion cyst of the talus: Case report. Foot Ankle. 1993;14:538-9.
- [CrossRef] [PubMed] [Google Scholar]
- Intraosseous ganglion. Am J Roentgenol Radium Ther Nucl Med. 1973;118:328-343.
- [CrossRef] [PubMed] [Google Scholar]
- The intraosseous ganglion. A clinical-pathological report on 42 cases. Arch Orthop Trauma Surg. 1994;114:14-7.
- [CrossRef] [PubMed] [Google Scholar]
- Bone cyst in the cervical spine due to secondary amyloidosis. A case report. Acta Orthop Scand. 1992;63:221-2.
- [CrossRef] [PubMed] [Google Scholar]
- Morphology and topography of intraosseous ganglion cysts in the carpus: An anatomic, histopathologic, and magnetic resonance imaging correlation study. J Hand Surg Am. 2003;28:52-61.
- [CrossRef] [PubMed] [Google Scholar]
- The natural history of ungrafted bone defects of the talus. J Bone Joint Surg Br Proceedings. 2008;90-B:401.
- [Google Scholar]




