
Translate this page into:
Intradural epidermoid cyst with atypical magnetic resonance imaging and clinical presentation
Address for correspondence: Dr. Uday Pote, C/O, Prakash B. Wankhede, Flat No. 3, Deepjyoti Apartment, Near BSNL Office, Left Bhusari Colony, Paud Road, Kothrud Depo, Pune - 411 038, Maharashtra, India. E-mail: dr.udaypote@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Pote U, Parasnis R, Pathak S, Bisht A. Intradural epidermoid cyst with atypical magnetic resonance imaging and clinical presentation. J Orthop Allied Sci 2016;4:91-4.
Abstract
Epidermoid cysts are a rare benign neoplasm of spine. They account for only 1% of all benign spinal tumors. These cysts are either congenital or acquired, like after repeated lumbar puncture. They can present anywhere in the spinal cord, and are intradural. They can be intra- or extra-medullary. As the cysts are slow growing, they are mostly reported after some sensorimotor or in some cases after bowel and bladder involvement. Typical magnetic resonance imaging (MRI) findings are a hyperintense signal on T2-weighted (T2W) and hypointense T2W images. Diagnosis is confirmed on histopathologic examination. The treatment is complete excision and if not then maximum debulking of the tumor. We present a case of 27-year-old male with only tingling and mild weakness in the left lower limb. He was diagnosed with intradural tumor with MRI findings showing hyperintense signal on T1-W and isointense signal on T2W images. This is an uncommon presentation. It was enmeshing around rootlets so had to be debulked. The diagnosis was confirmed on histopathologic examination. Postoperatively recovery was excellent with no neurological deficit.
Keywords
Epidermoid cyst
intradural epidermoid tumor
lumbar spine
surgery
total excision

Introduction
Epidermoid cysts are rare benign neoplasm within the neuraxis, which are commonly located in the intracranial region and account for <1% of all intraspinal tumors.[1,2] In 1835, Cruveilhier was the first to describe epidermoid cysts, calling them tumeurs perlées (pearly tumors).[3,4] Epidermoid cysts can be congenital or acquired. Congenital epidermoid cysts are frequently found in association with spinal dysraphisms such as syringomyelia, dermal sinus, and spina bifida, while the most common etiology for an acquired cyst is repeated lumbar puncture.[2,5]
Although epidermoid cysts can be extradural, intradural or extramedullary, or intramedullary in the spine, the tumors are often intradural and extramedullary in the lumbosacral region.[6]
Neurologic symptoms such as progressive paraparesis, motor-sensory complaints, and sphincter troubles cause great distress.[2,4,5,7,8] Patients with an epidermoid cyst usually suffer for a long time with symptoms, for an average time of 6 years, due to their slow-growing nature.[2,4]
Magnetic resonance imaging (MRI) is an effective tool in the diagnosis of intraspinal epidural cyst. On MRI, the tumor is usually isointense or hypointense in T1-weighted (T1W) images and hyperintense in T2-W images, and the cyst content has the same signal as the cerebrospinal fluid.[9,10,11]
We present a case with atypical clinical findings and MRI shows finding of being hyperintense in T1W image and isointense in T2W images.
Case Report
A 27-year-old male presented with tingling and weakness of the left lower limb since last 6 months. Tingling appeared 6 months back and for last 2 months felt weakness and limp while walking in the left leg. On examination, he had no cutaneous lesions on back; he had power Grade 5 in bilateral lower limbs. Sensations were intact. Left lower limb toe walking was unsteady. Reflexes of both ankle and knee were depressed bilaterally. No sensory involvement. No bowel bladder involvement. Perianal sensations were intact.
His MRI showed heterogeneous hyperintense lesion at cauda equina of spine at L1-L2 level on T1W and isointense on T2W. It showed minimal heterogeneous postcontrast enhancement. It was displacing spinal nerve roots at this level. Screening of spine revealed no lesions anywhere else in the spine and no spinal dysraphisms [Figures 1-3 and 4].
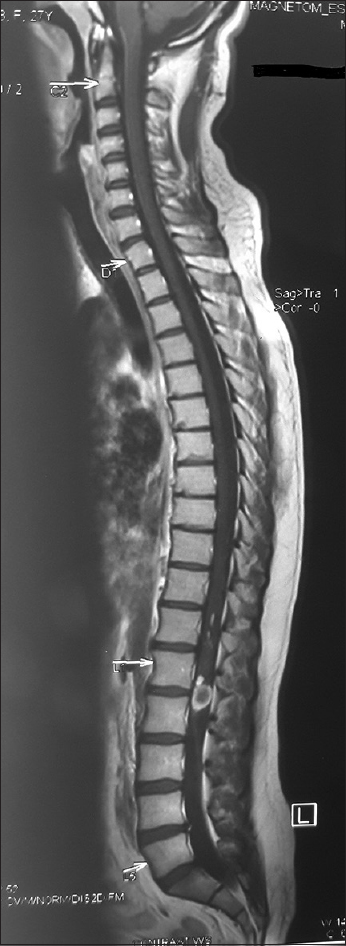
- T1-weighted sagittal magnetic resonance imaging showing a solitary lesion
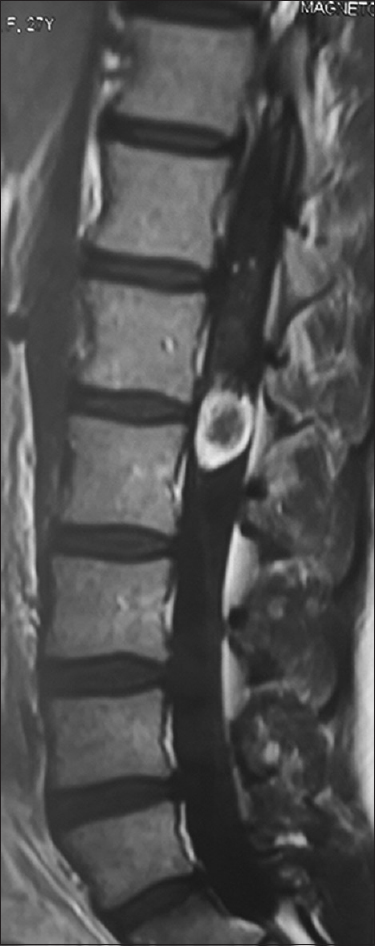
- T1-weighted sagittal magnetic resonance imaging showing hyperintense isolated lesion behind L1-L2 bodies

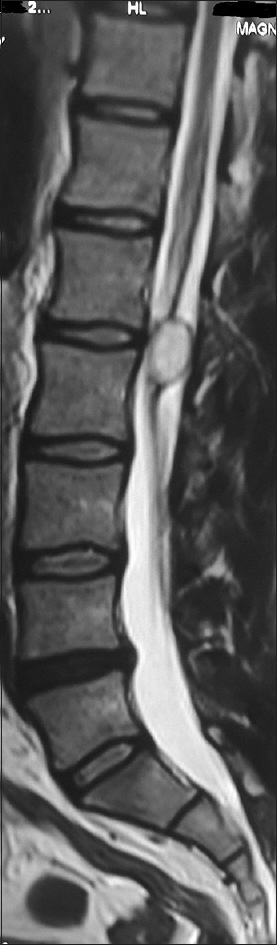
- T2-weighted sagittal magnetic resonance imaging showing isointense lesion
- Postcontrast minimal heterogeneous enhancement
Intraoperatively, L1-L2 midline laminectomy was done, an obvious bulging of the cord was seen at the involved level. Durotomy was done; the tumor sheath was attached to nearby rootlets. We tried to separate the sheath from the roots, but they were intimately attached and removing the attachment threatened severing the roots. Hence, we opened the sheath and debulking was done. Pearly white and flaky pieces of tumor pieces were removed. After near complete removal, durotomy was closed, and layer by layer skin closure was done.
Histopathologic examination showed cystic lesion lined by keratinized stratified squamous epithelium and lumen filled with keratinous material. The stroma showed fibro-adipose tissue [Figure 5].
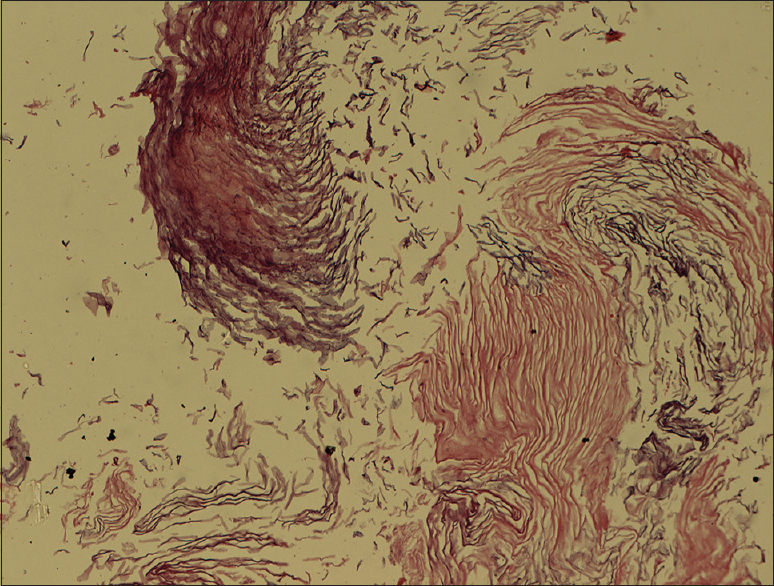
- Histopathologic examination showed cystic lesion lined by keratinized stratified squamous epithelium and lumen filled with keratinous material. The stroma showed fibro-adipose tissue
Postoperatively, the patient had no new neurological deficit. One month later, his power in bilateral lower limbs remained Grade 5. His limp reduced but still he has difficulty to toe walk over left limb. His tingling has reduced only mildly.
Discussion
Epidermoid cysts in the spine are thought to arise from one to two possible origins: congenital or acquired.[12] Congenital epidermoid cysts, which are more common and often associated with other spinal dysraphisms, are caused by the anomalous implantation of ectodermal cells during closure of the neural tube between the 3rd and 5th weeks of embryonic life.[2,13,14] The number of acquired cysts has decreased significantly in recent years. They are attributed to the displacement of epithelial tissue secondary to a previous lumbar puncture or trauma.[15,16,17]
The case we present is of congenital in origin as he had no history any trauma or lumbar puncture. He neither had evidence of other spinal abnormalities.
Symptoms arising from epidermoid cysts vary with the level of involvement but do not differ from other space-occupying lesions in the spinal column. Signs and symptoms at presentation are usually neurological such as progressive paraparesis, sensory loss, urological manifestations, and back/leg pain. The slow growth of epidermoid cysts often leads to a delay in their diagnosis: Duration of symptoms before diagnostic recognition may extend for many years. Due to this, the symptoms may often arise in early or middle adult life.[12]
MRI is an effective tool for the diagnosis of an intraspinal epidermoid cyst. X-rays often show a normal image and computed tomography can only display the location and outline of the tumor. On MRI, the tumor is usually isointense or hypointense in T1-W images and hyperintense in T2-W images and the cyst content has the same signal as the cerebrospinal fluid.[9,10,11] However, these signal characteristics are not always constant, and some variations have been reported in the literature.[10,18,19] Our case shows atypical finding of being hyperintense in T1W image and isointense in T2W images. Similar MRI finding in one case was reported by Yin et al.[20]
The pathologic examination is vital for the final diagnosis of an epidermoid cyst. Histologically, epidermoid cysts are composed of lined stratified squamous epithelium supported by an outer layer of collagenous tissue. Progressive desquamation of keratin from the epithelial lining toward the interior of the cyst produces a soft white material rich in cholesterol crystals.[2,19,21,22] The absence of skin adnexa is the key to differentiate one from a dermoid cyst.[2,22]
Given their indolent, benign nature, asymptomatic epidermoid cysts should be managed conservatively. Surgical excision is essential for lesions with symptomatic progression and where imaging shows that neural elements are compressed.[19,20,23,24] Although radiotherapy has been used in one case with repeated relapses of epidermoid cysts, achieving a relatively good result, this treatment should only be used for patients who refuse surgery or are inoperable for medical reasons.[25] Undoubtedly complete excision without neural damage is the goal of treatment. Emptying of the cyst material can be performed easily, but the intimate adherence between the capsule and the spinal cord makes this goal difficult. Hence, subtotal excision tends to be the more common surgical pattern for avoiding possible neural damage.[10,11,12,21,26,27] Subtotal excision also causes great distress for patients and doctors because debris from the tumor may cause an early relapse of symptoms and the spread of cyst contents can cause foreign body reactions and severe complications.[2,9,11,21,24,25]
Conclusion
Given the atypical presentation of the MRI causes confusion in the diagnosis. Sometimes due to slow growing nature it's very late that such a tumor is diagnosed, that is after the patient has some neurological deficit. Histopathologic examination remains authoritative in confirming the diagnosis. Total excision of tumor is desired but as it may cause damage to roots and increase neurodeficit, debulking and subtotal removal may be enough. Recurrence if present must be dealt with radiotherapy.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Intramedullary epidermoid cyst: Preoperative diagnosis and surgical management after MRI introduction. Case report and updating of the literature. J Neurosurg Sci. 2002;46:122-6.
- [Google Scholar]
- Intramedullary epidermoid cysts of the spinal cord. Case report. J Neurosurg. 1992;76:528-33.
- [CrossRef] [PubMed] [Google Scholar]
- A cervico-dorsal intramedullary epidermoid cyst. Case report and review of the literature. J Neurosurg Sci. 1991;35:111-5.
- [Google Scholar]
- Long-term results of the surgical treatment of spinal dermoid and epidermoid tumors. Neurosurgery. 1989;25:860-4.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging for spine tumors and new applications. Top Magn Reson Imaging. 2006;17:69-87.
- [CrossRef] [PubMed] [Google Scholar]
- Intramedullary epidermoid cyst in cervicodorsal spinal cord. J Neurosurg. 1999;90(1 Suppl):161.
- [CrossRef] [PubMed] [Google Scholar]
- Intramedullary epidermoid cyst of the cervical spinal cord associated with an extraspinal neuroenteric cyst: Case report. Neurosurgery. 1992;31:121-5.
- [CrossRef] [PubMed] [Google Scholar]
- Spinal epidermoid cyst with sudden onset of paraplegia. J Cancer Res Ther. 2009;5:290-2.
- [CrossRef] [PubMed] [Google Scholar]
- Unusual magnetic resonance characteristics of a cerebellopontine angle epidermoid cyst with upper cervical spinal canal extension. J Clin Neurosci. 2006;13:781-4.
- [CrossRef] [PubMed] [Google Scholar]
- Epidermoid cysts associated with thoracic meningocele. Acta Neurochir (Wien). 2008;150:305-8.
- [CrossRef] [PubMed] [Google Scholar]
- Epidermoid cyst of the thoracic spine: Case history. Clin Neurol Neurosurg. 2001;103:220-2.
- [CrossRef] [PubMed] [Google Scholar]
- Ueber die pialen epidermoide. Dermoide und lipome und duralen dermoide. Zentralbl Allg Pathol. 1897;8:1-98.
- [Google Scholar]
- Intraspinal epidermoid after lumbar puncture. Int Orthop. 1994;18:116-8.
- [CrossRef] [PubMed] [Google Scholar]
- Intraspinal epidermoid tumour: Late complication of lumbar puncture. CMAJ. 1989;141:223-5.
- [Google Scholar]
- Iatrogenic intraspinal epidermoid sequestration cysts. Radiology. 1969;92:251-4.
- [CrossRef] [PubMed] [Google Scholar]
- Signal intensity patterns in intraspinal dermoids and epidermoids on MR imaging. Clin Radiol. 1993;48:405-13.
- [CrossRef] [PubMed] [Google Scholar]
- Iatrogenic intraspinal epidermoid tumor: Myelo-CT and MRI diagnosis. Neuroradiology. 1989;31:273-5.
- [CrossRef] [PubMed] [Google Scholar]
- Surgery and outcomes of six patients with intradural epidermoid cysts in the lumbar spine. World J Surg Oncol. 2014;12:50..
- [CrossRef] [PubMed] [Google Scholar]
- Intramedullary spinal epidermoid cyst of the upper thoracic region. J Clin Neurosci. 2009;16:142-4.
- [CrossRef] [PubMed] [Google Scholar]
- Intramedullary spinal epidermoid cyst of the cervicodorsal region: A rare entity. J Pediatr Neurosci. 2010;5:49-51.
- [CrossRef] [PubMed] [Google Scholar]
- Intramedullary inclusion cysts of the cervicothoracic junction. Report of two cases in adults and review of the literature. J Neurosurg Spine. 2007;7:236-42.
- [CrossRef] [PubMed] [Google Scholar]
- Recurrent intramedullary epidermoid cyst of conus medullaris. BMJ Case Rep 2011:2011. pii:Bcr1120115090
- [CrossRef] [PubMed] [Google Scholar]
- Intraspinal epidermoid cyst successfully treated with radiotherapy: Case report. Neurosurgery. 2003;53:1429-31.
- [CrossRef] [PubMed] [Google Scholar]
- Intramedullary thoracic spine epidermoid cyst with myelopathic presentations: A report of a rare case. Clin Neurol Neurosurg. 2013;115:841-3.
- [CrossRef] [PubMed] [Google Scholar]
- A giant intramedullary spinal epidermoid cyst of the cervicothoracic region. Pediatr Neurosurg. 2004;40:120-3.
- [CrossRef] [PubMed] [Google Scholar]




