
Translate this page into:
Hip-spine syndrome: A contemporaneous double surgery
Address for correspondence: Dr. Christian Capuano, Department of Orthopedic Surgery and Spinal Surgery, Garofolo Health Care, Vicenza, Italy. E-mail: info@christiancapuano.it
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Capuano C, Parisotto R, Carnini F, Rasia Dani E. Hip-spine syndrome: A contemporaneous double surgery. J Orthop Spine 2023;11:40-2.
Abstract
The incidence of symptomatic osteoarthritis of the hip and degenerative lumbar spinal stenosis is increasing in our aging population. The movements between the spine, pelvis, and hip joints are coordinated to allow for a physiological balance of the upper body and the pelvis during sitting and standing positions. Degenerative changes or spondylolisthesis of the spine result in decreased pelvic mobility and can lead to increased rates of instability and the necessity of total hip arthroplasty. This case report aims to determine the importance of communication between surgeons, in this case, a neurosurgeon and an orthopedic surgeon, which in our experience is very limited in clinical practice. We believe this lack of communication and collaboration is far from ideal for patients; their pathologies are not always put before functional aspects of the hospital or clinic, surgeon’s schedules, etc. This case represents the criterion standard of how a disease such as hip-spine syndrome, in certain cases, must be operated on in two parts of the body during the same surgical session.
Keywords
Coxarthrosis
lumbar arthrodesis
spine
spondylolisthesis
total hip replacement

Introduction
Hip-spinesyndrome is an often-disabling degenerativediseaseaffecting both the spine and the hip joint. A 71-year-old patient suffering from clearly diagnosed hip-spine syndrome required lumbosacral surgery to correct evident extensive osteoligamentous decompression and lumbar arthrodesis with microsurgical technique and a total hip joint reconstruction.
Two surgeons operating at the same clinic decided to perform the two needed surgeries under a single application of anesthesia, thus subjecting the patient to one operation instead of two. The total time of surgery was 4.5 h.
Case Report
Clinical and diagnostic exams
General condition: Male, age 71; cardiopathic and hypertensive; walking autonomy of 20 m. The patient complained of progressive difficulty in movement with a decline in the quality of life. Patient’s visual analog scale (VAS) was 10.
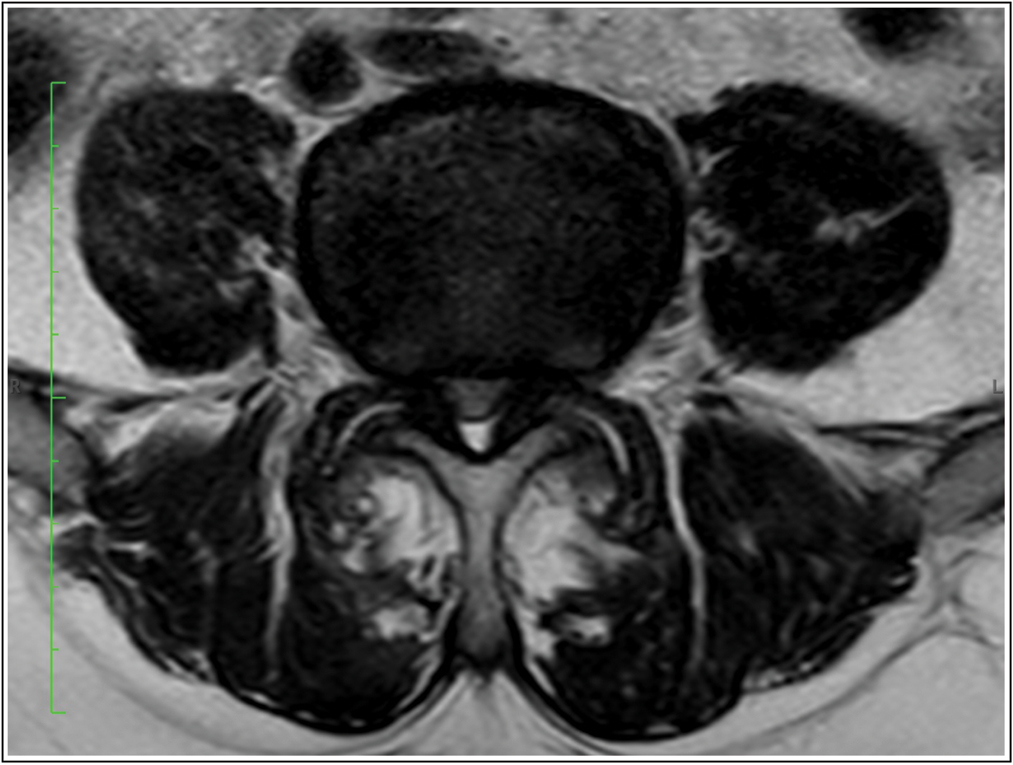
A lumbosacral magnetic resonance imaging exam showed degenerative L4–L5 spondylolisthesis complicated by severe disc disease and foraminal stenosis with evident radicular conflict on the right side [Figures 1 and 2]; these pathologies created a condition of functional impotence with regard to pain management. This clinical picture was associated with a painful symptomatology in the right hip due to coxarthrosis; an advanced state of arthrosis which was clearly observable in a diagnostic radiograph [Figure 3].

- A degenerative L4–L5 anterolisthesis complicated by severe and tight stenosis of the spinal and foraminal canals. Source: Photo property of C. Capuano
- This clinical picture was associated with a painful symptomatology in the right hip due to coxarthrosis; an advanced state of arthrosis was clearly observable in a diagnostic radiograph. Source: Photo property of C. Capuano
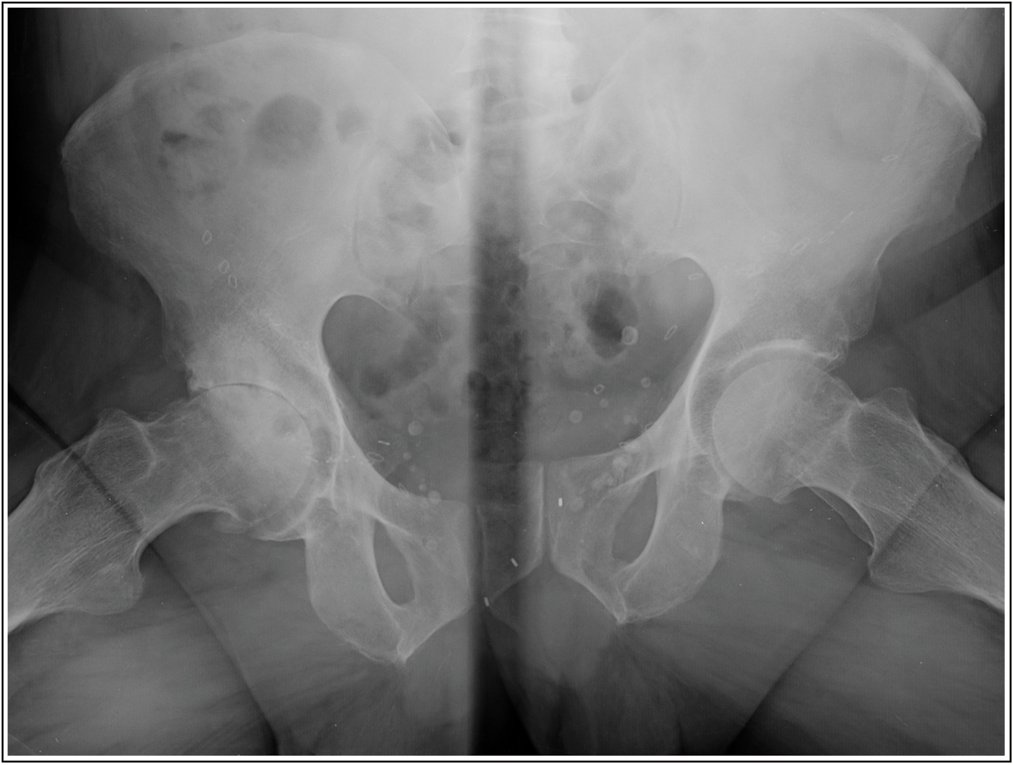
- Presence of grade III coxarthrosis according to the Tonnis classification, clinically symptomatic with functional impotence to load and limitation of range of movement. Source: Photo property of C. Capuano
Treatment plan
The patient would undergo physiotherapy to relieve symptoms and strengthen the body in a general way as preparation for surgery.
Most importantly, he was found suitable to undergo two surgeries in different parts of the body while under the same application of anesthesia:
Decompression microsurgery of the spinal canal and a discectomy, including the interposition of a titanium oblique cage for fusion and vertebral stabilization;
Reconstruction of the hip joint, utilizing a minimally invasive anterior approach (anterior minimally invasive surgery).
The patient would undergo conventional postsurgical physiotherapy [Figures 4-7].

- Postoperative X-ray shows lumbar arthrodesis with cage insertion with TLIF approach and total hip replacement. Source: Photo property of C. Capuano
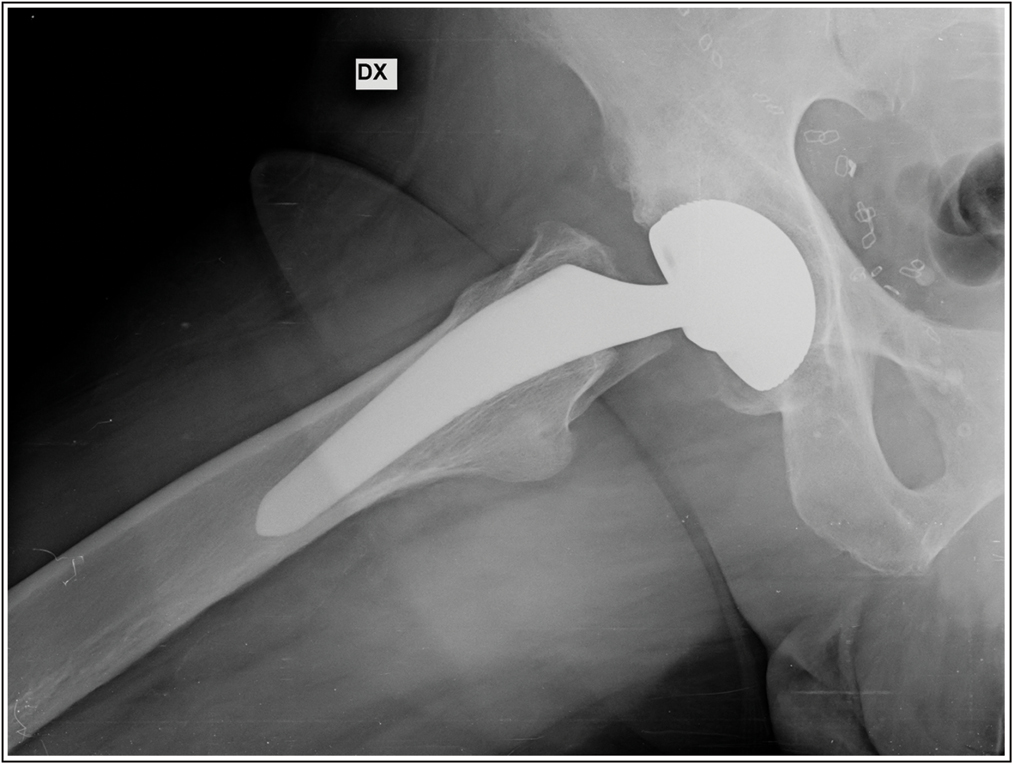
- Post-operative X-ray shows Minimally invasive total hip arthroplasty using the anterior approach. Source: Photo property of C. Capuano
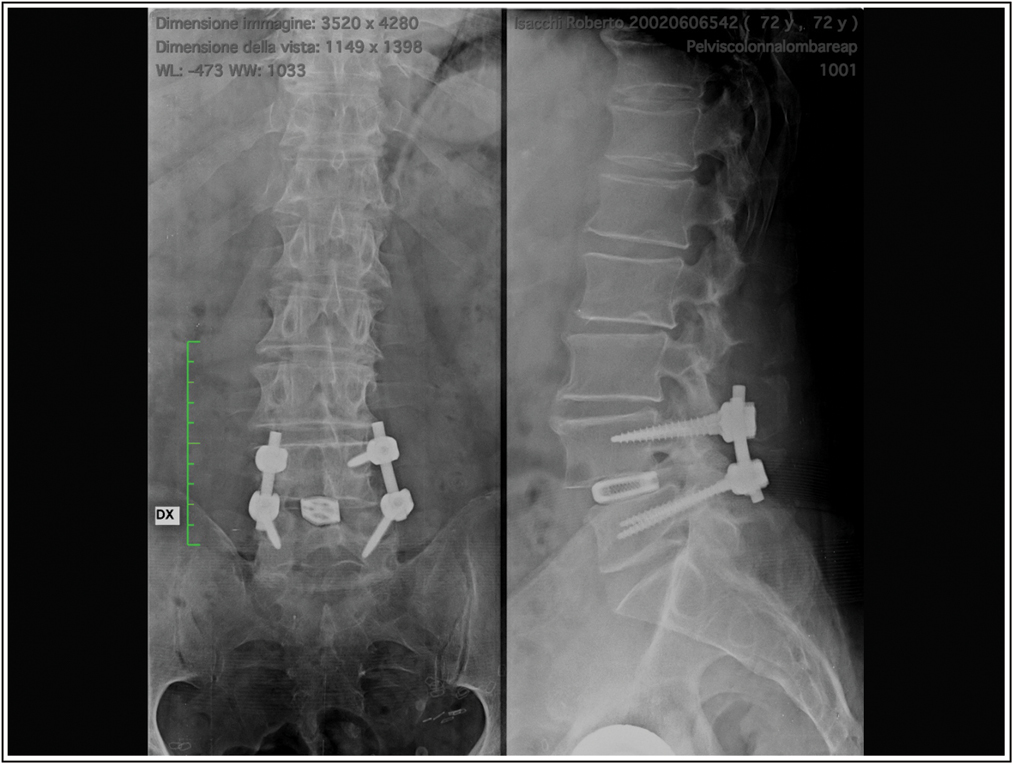
- Post-operative X-ray anterior and lateral view: Lumbar Arthrodesis L4-L5 with mini-open Transforaminal lumbar interbody fusion (TLIF) procedure. Source: Photo property of C. Capuano
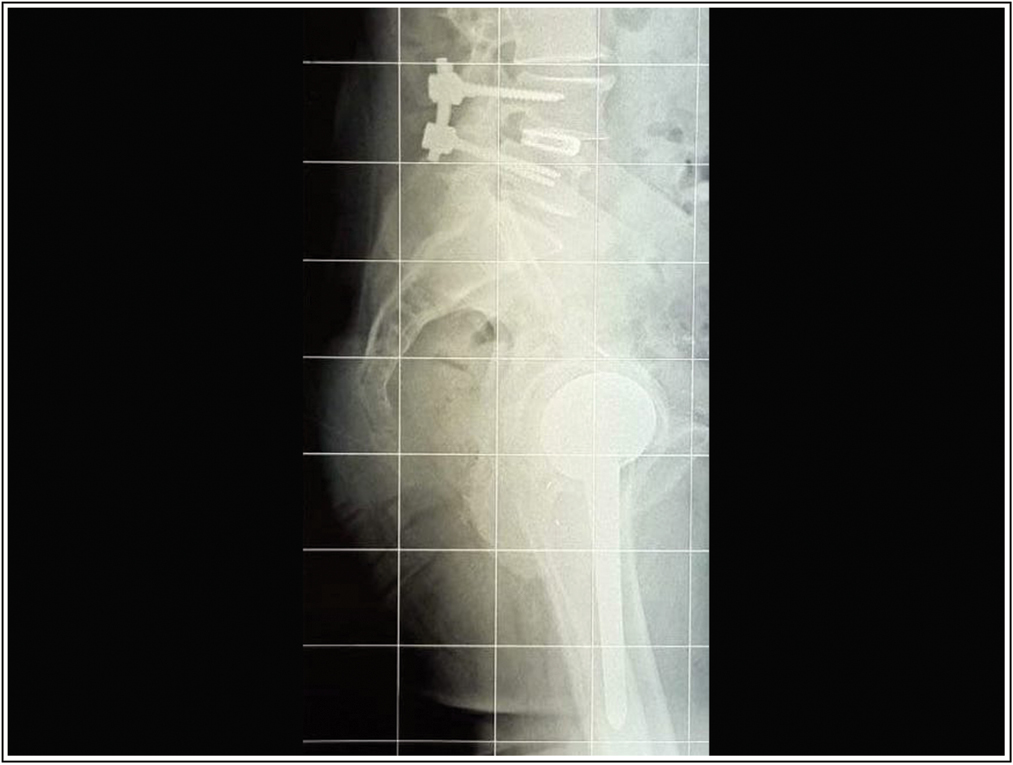
- Post-operative X-ray shows Lumbar Arthrodesis L4-L5 with mini-open Transforaminal lumbar interbody fusion (TLIF) procedure and Minimally invasive total hip arthroplasty using the anterior approach. Source: Photo property of C. Capuano
Outcome
On the first postoperative day, the patient was mobilized without any kind of support, and the clinical picture was completely resolved. The patient now walks autonomously without any pain or limitation in carrying out normal daily activities, and he is also able to take long walks.
Discussion
Hip-spine syndrome primarily affects patients with concomitant symptomatic stenosis of the spinal canal. These patients present with neurogenic claudication, describing lumbar and lower extremity pain with a marked reduction in walking range. It is well established that the underlying pathophysiology of neurogenic claudication is due to specific postural functioning; when standing up, the normal lumbar lordosis increases in order to maintain sagittal balance, leading to deformation of the yellow ligament and the subsequent narrowing of the spinal canal.
It is essential that this pathology, of interest to both orthopedic surgeons and neurosurgeons, is dealt with clinically and diagnostically by both professional figures together.
The existing literature underlines the importance of understanding which degenerative pathology to address first; however, it is considered absolutely essential to choose a surgery that will definitively solve the pain problem without prioritizing which surgery to perform first, because the etiopathogenesis of both pathologies is the same.
As such, in this clinical case, we will focus attention on physicians who have decided to intervene surgically simultaneously. This choice, which required careful preoperative and anesthesia planning, was aimed at the complete resolution of the problem and not at understanding which surgery should be performed first; especially if a patient has concomitant pathologies, which certainly exposes them to greater risks if they have to undergo multiple surgeries, and are also elderly.
Conclusion
Hip-spine syndrome is certainly a disabling disease. In recent decades, there has been a tendency to compartmentalize orthopedic surgical disciplines. The clinical case presented here is exemplary in focusing attention on the importance of continuous communication between surgeons and in taking the only rational choice for the total resolution of the problem.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.




