
Translate this page into:
Functional outcome for the acromioclavicular joint disruption with or without lateral end clavicle fractures treated with hook plate
Address for correspondence: Dr. Hariprasad Seenappa, Department of Orthopaedics, Sri Devaraj Urs Medical College, Sri Devaraj Urs Academy of Higher Education and Research, Tamaka, Kolar - 563 101, Karnataka, India. E-mail: drhariprasad.ortho@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Sivanandan S, Seenappa H, Fernando C, Madanamanchi H. Functional outcome for the acromioclavicular joint disruption with or without lateral end clavicle fractures treated with hook plate. J Orthop Spine 2020;8:65-9.
Abstract
BACKGROUND:
Acromioclavicular (AC) joint dislocation is most frequently encountered in contact sports and is far more common in males. Grade-III AC dislocation involves complete loss of contact between the clavicle and acromion secondary to the total disruption of both the AC and coracoclavicular ligaments, with loss of vertical and horizontal stability, respectively. The use of hook plate on open reduction and internal fixation of the AC joint dislocation had a little adverse effect on shoulder function and is an effective method for the treatment of AC joint dislocation. Hence, this retrospective study was carried out to assess the clinical and functional outcome of AC joint injuries treated with hook plate.
AIM:
The aim of this study is to assess and document the clinical and functional outcome of AC joint dislocation with or without lateral end clavicle fracture treated with hook plate.
MATERIALS AND METHODS:
This retrospective study of patients with Rockwood Type III AC joint disruption (dislocation) who were treated in our hospital. During the period from July 2013 to July 2018, a total of 33 patients with Type III AC joint disruption with or without associated lateral end clavicle fractures were included in this study, with 26 males and 7 females. The functional outcome was assessed using the CONSTANT scoring system during follow-up after hook plate fixation at 4 weeks, 3 months, 6 months, and 12 months.
RESULTS:
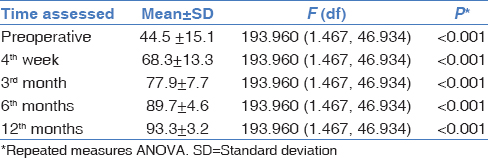
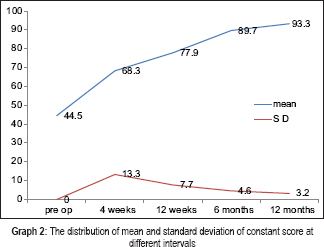
Thirty three patients with AC joint disruption were participated in the study after meeting the inclusion and exclusion criteria. There were 26 males (78.8%) and 7 females (21.2%) with a mean age of 44.7 years, eight patients had an associated lateral end clavicle fracture. All the patients were fixed with hook plate were followed up for a period of 1 year postoperatively. The mean Constant score improved progressively from a preoperative score of 44.5 to postoperative score of 68.3 at 4 weeks, 77.9 at 3 months, 89.4 at 6 months, and 93.3 at 12 months.
CONCLUSIONS:
In the current study, we conclude that the surgical and functional outcomes after AC joint stabilization with or without lateral end clavicle fractures using hook plate fixation yield satisfactory results. The hook plate also provides good horizontal, rotational, and vertical stability. Furthermore, the maintenance of reduction by the hook plate was significantly superior compared to the other modes of treatment. The hook plate also facilitates early mobilization and prevents stiffness of the shoulder joint.
Keywords
Acromio-clavicular joint disruption
CONSTANT score
hook plate
lateral end clavicle fracture

Introduction
The acromioclavicular (AC) joint is a diarthrodial joint, only 1 of the 5 joints that make up the complex arrangement of the shoulder. Together with the sternoclavicular joint, the AC joint provides the upper extremity with a connection to the axial skeleton. Injuries to the AC joint are very common in athletes and a source of significant morbidity. AC pathology, particularly athletes whose sport demands overhead upper limb activity. These problems are most frequently encountered in contact sports and are far more common in males.[1]
AC dislocations can be classified into six grades according to the extent of displacement of the clavicle in relation to the acromion. Grade-III AC dislocation involves complete loss of contact between the clavicle and acromion secondary to the total disruption of both the AC and coracoclavicular (CC) ligaments, with loss of vertical and horizontal stability, respectively. The distal end of the clavicle is displaced superiorly, secondary to the indirect force of the arm in extension, which transmits the load to the acromion through the humeral head.[2]
Conservative management is indicated for Rockwood Types I and II. In contrast, surgical intervention is reserved for more severe Types IV–VI with the involvement of the CC ligaments resulting in a relative dislocation of the clavicle. Restoration of the normal anatomy of the AC joint corrects the obvious deformity and prevents a potentially unsatisfactory outcome that may include persistent discomfort and secondary AC joint degenerative changes. The management of Rockwood Type III AC joint dislocation remains controversial, with most authors recommending an operative approach in case of manual workers.[3]
Different approaches have been described for the management of these injuries ranging from conservative management with bandages and slings to multiple surgical options including fixation of the AC joint with pins, tension band wiring, the modified Weaver–Dunn procedure, fixation with washer and screw, suspensory fixation devices and clavicular hook plate.[4]
The hook plate is a precontoured plate in a variety of sizes with a hook of varying depths to suit different patients' anatomy. The hook is situated posteriorly; hence, it is a right or left-sided implant. Various companies make the implant, including the AO synthesis system. The hook plate system enables early rotational mobility of the shoulder.[5]
The use of hook plate on open reduction and internal fixation of the AC joint dislocation had a little adverse effect on shoulder function and is an effective method for the treatment of AC joint dislocation.[6] Hence, this retrospective study was being taken.
Materials and Methods
Source and type of study
This is a retrospective study of 33 cases that were admitted and operated in the Department of orthopedics attached to R. L. Jalappa hospital, Sri Devaraj Urs Medical College, a constituent of Sri Devaraj Urs Academy of Higher Education and Research, Kolar, Karnataka, India, from July 2013 to July 2018. This study was done after the Institutional ethics committee approval (SDUMC/KLR/IEC/78/2018-19). All surgeries were conducted at our institute by three-lead surgeons from the Department of Orthopedics.
Inclusion criteria
All patients with Rockwood Type III AC injuries
Associated lateral end clavicle fractures.
Exclusion criteria
Rockwood Type I, II, IV, V, VI injuries
Open fractures
Polytrauma
Neurovascular injury.
Patients were assessed clinically and radiologically were included in the study. The functional outcome was assessed using Constant scoring system during follow-up after hook plate fixation for AC joint disruption with or without lateral end clavicle fracture at 4 weeks, 3 months, 6 months, and 12 months.
The sample size in the study was 33 and the collected data were coded in excel format; all the quantitative measures, categorical variables such as functional outcome, sex, age, side of fracture, and fracture type were compared using percentages. To compare and to assess the progress of constant score at different intervals we used repeated measures analysis of variance with Greenhouse-Geisser correction. Post hoc analysis was performed using the Bonferroni test. Value of P < 0.001 was considered statistically significant. Statistical analysis was carried out using software-SPSS version 22 (IBM, Chicago, IL, USA) and Medcalc 18.11.3.
Operative procedure
The patient was put in the supine position and transverse incision was made over the lateral end of the clavicle and extending over the AC joint measuring about 5–7 cm. After the skin incision the delto-trapezial fascia was cut and the AC joint was reduced, any associated lateral end clavicle fracture was also reduced, and the reduction was stabilized with an appropriate sized hook plate with the hook positioned posteroinferiorly to the acromion. The hook plate is fixed to the clavicle using screws along with one screw to the coracoid process (CC screw fixation). No additional reconstruction or repair of coracoclavicular and acromio clavicular ligaments were done. The surgical site was closed in layers.
Postoperative regimen
A shoulder arm pouch was given to all patients for 3 weeks. Active/passive range of movements of the shoulder was started from the 2nd postoperative day as per pain tolerance. A detailed progressive rehabilittion was started after suture removal on the 10th postoperative day. The patients were allowed to do their daily tasks, and unrestricted active shoulder movements were allowed 6 weeks postoperatively. Patients were allowed for simple weight lifting after 4 months postsurgery. The patients were regularly followed up with a protocol of 1, 3, 6, and 12 months.
Results
In this study, a total of 33 patients with AC joint disruptions were included. There were 26 males (78.8%) and 7 females (21.2%) with a mean age of 44.7 years. In these seven patients is under 30 years of age, 12 patients in a range of 30–50 years and most of the remaining patients, i.e., 14 patients were >50 years [Graph 1]. Road traffic accident was the main etiology followed by self fall. Nineteen patients had right-sided acromioclavicular joint disruptions and 14 patients had left-sided injury.
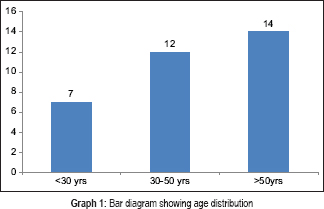
Among 33 patients, eight patients had an associated lateral end clavicle fracture. In these seven patients are <30 years of age, 12 patients are aged between 30 and 50 years and 14 patients were >50 years.
The average time to surgery after hospital admission was 2.35 ± 0.79 days. All the patients with Hook plate (3–5 holed) and the patients were followed up for a period of 1 year postoperatively [Figures 1-3]. The postoperative radiographs were obtained on the second postoperative day showed good reduction of the AC joint with stable fixation of hook plate with screws with or without a screw to the coracoid process (coraco-clavicular screw fixation). All the patients healed well except three patients who had superficial surgical site infection, which was treated conservatively. In our series, 3 patients had the prominence of the hardware, as they were thin, and four patients had discomfort while attempting movement and three patients had painful terminal range of motion (ROM) while doing abduction. Seven patients underwent implant removal at the end of 18 months with stable AC joint.
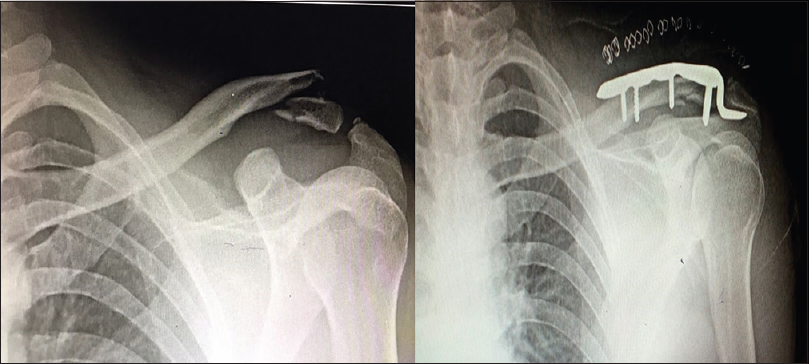
- Left acromioclavicular joint disruption with lateral end clavicle fracture pre- and post-operative X-rays
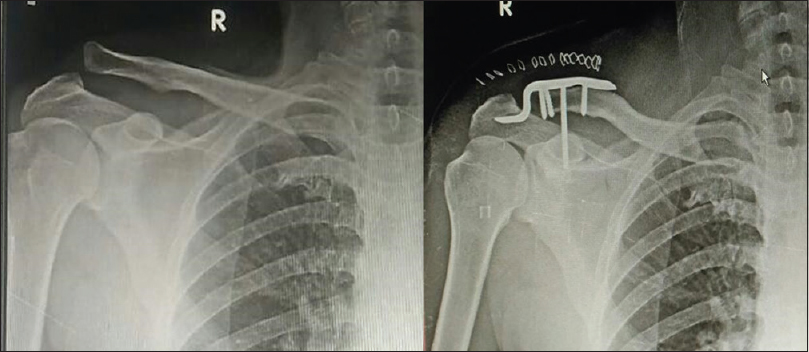
- Right acromioclavicular joint disruption preoperative and postoperative X-rays
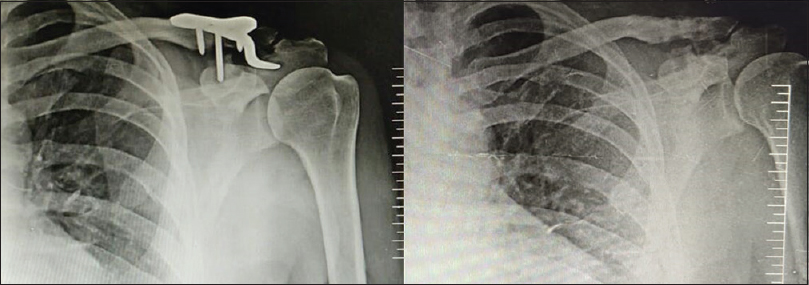
- United 18-month-old left acromioclavicular joint disruption with lateral end clavicle fracture X-rays before and after implant removal
Discussion
The treatment of AC joint disruption with or without lateral end clavicle fractures varies based on their indications. The need for surgery and their choice of implant is based on the type of AC joint disruption and the associated lateral end clavicle fracture. Variety of treatment includes Kirschner wires, Tension band wire around coracoid and clavicle, repair of CC ligament with augmentation by endo buttons, and the hook plate.[7,8,9,10]
In these methods, Kirschner wire had a higher incidence of migration, while the Bosworth screw had more chance of rotations, screw backout, and cut out. Hook plate was widely used because of its stable fixation against horizontal, rotational and vertical forces and early mobilization with much stability. When compared to elderly people, the younger or adult age group people have a maximum need for fixation as nonunion rate was higher and shoulder pain because of ligamentous disruption and the lack of their healing.
In our study, we noted an improvement in constant score at 3rd month with a mean of 77.9 for 33 patients and further improvement in score by 89.7 at 6th month [Table 1 and Graph 2]. These results were similar to the results of the studies by Yoon et al. who noted a constant score of 90.2 at 6 months and Lingaraju et al. who noted a constant score of 82.5.[11,12]
In a study conducted in which reconstruction of CC and AC ligament with allogenic tendon compared with hook plate suggested both are effective in all means including the functional outcome and stability, but hook plate needs hardware removal and has more pain when compared to allogenic tendon reconstruction.[13] One of the previous studies suggests 15° prebent hook plate for AC joint disruptions when compared to normal 0° hook plate for better rehabilitation and more reduction in the postoperative shoulder pain.[14]
The use of hook plate in the treatment of AC joint disruptions and fractures of the lateral end of the clavicle is shown to be a good and acceptable treatment option. AC joint dislocations result in an inferior sag of the scapula[15] and stability at this joint must be achieved either by repair of the ligaments and/or stabilizing with a plate or other fixation devices.
With regards to the use of a hook plate, there are debatable statements regarding retaining the implant for a more longer duration as against removal when the patient is symptomatic. The ideal time for implant removal is still controversial. In a study by Lin et al.,[16] the hook plate removal was done as early as possible, i.e., 6 months in view of subacromial shoulder impingement and rotator cuff lesion. Whereas in our study, implant removal was done after 1-year once the patients had returned to their daily activities without any difficulty. The need for either simultaneous reconstruction or repair of the ligaments along with hook plate method of fixation, further suggesting implant removal after radiological or clinical indication and/or reconstruction after plate removal depending on the instability.[15] Implants like endobuttons does not require removal, so it avoids additional surgery to the patient.[17]
In our series, three patients had prominence of the hardware, as they were thin and four patients had discomfort while attempting movement, and three patients had painful terminal ROM while doing abduction. Seven patients underwent implant removal at the end of 18 months with a stable AC joint. These results are comparable with other studies though the exact reason of shoulder stiffness is unknown; it appears to be a posttraumatic frozen shoulder.[18,19]
No osteolysis of the acromion was noted at the end of the hook. The presence of osteolysis between the plate and the acromion has been attributed to the rotational movement (micromotion), which occurs with abduction resulting in rotation of the clavicle and the hook plate in respect to the acromion.
Limitation in study
The primary limitation of our study was that it was a retrospective study, including a small number of patients and done at a single center. There was no control group in the present study. Larger randomized controlled trials are needed to further evaluate the outcomes and complications of precontoured hook plates.
Conclusions
In the current study, we conclude that the surgical and functional outcomes after AC joint stabilization with or without lateral end clavicle fractures using hook plate fixation yield satisfactory results. The hook plate also provides good horizontal, rotational, and vertical stability. Furthermore, the maintenance of reduction by the hook plate was significantly superior compared to the other modes of treatment. The hook plate also facilitates early mobilization and prevents stiffness of the shoulder joint.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Clavicular hook plate for Grade-III acromioclavicular dislocation. J Orthop Surg (Hong Kong). 2014;22:329-32.
- [CrossRef] [PubMed] [Google Scholar]
- Management of acute acromioclavicular joint dislocation with a double-button fixation system. Injury. 2013;44:288-92.
- [CrossRef] [PubMed] [Google Scholar]
- Hook plate fixation for acute acromioclavicular dislocations without coracoclavicular ligament reconstruction: A functional outcome study in military personnel. Strategies Trauma Limb Reconstr. 2015;10:79-85.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical outcome following treatment with clavicular hook plate. J Trauma Treat. 2012;1:1-3.
- [CrossRef] [Google Scholar]
- Effects of hook plate on shoulder function after treatment of acromioclavicular joint dislocation. Int J Clin Exp Med. 2014;7:2564-70.
- [Google Scholar]
- Semitendinosus tendon graft versus a modified Weaver-Dunn procedure for acromioclavicular joint reconstruction in chronic cases: A prospective comparative study. Am J Sports Med. 2009;37:181-90.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanical comparison of a modified Weaver-Dunn and a free-tissue graft reconstruction of the acromioclavicular joint complex. Am J Sports Med. 2010;38:1196-203.
- [CrossRef] [PubMed] [Google Scholar]
- Acromioclavicular joint reconstruction using peroneus brevis tendon allograft. Arthroscopy. 2007;23:788.e1-4.
- [CrossRef] [PubMed] [Google Scholar]
- Arthroscopic-assisted locking compression plate clavicular hook fixation for unstable fractures of the lateral end of the clavicle: A prospective study. Int Orthop. 2010;34:839-45.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of results between hook plate fixation and ligament reconstruction for acute unstable acromioclavicular joint dislocation. Clin Orthop Surg. 2015;7:97-103.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical fixation of Rookwood Type III-V acromioclavicular joint dislocation with acromioclavicular: Hook plate. J Orthop Traumatol Rehabil. 2018;10:44-8.
- [CrossRef] [Google Scholar]
- Treatment of AC dislocation by reconstructing CC and AC ligaments with allogenic tendons compared with hook plates. J Orthop Surg Res. 2018;13:1-7.
- [CrossRef] [PubMed] [Google Scholar]
- Fifteen-degree clavicular hook plate achieves better clinical outcomes in the treatment of acromioclavicular joint dislocation. J Int Med Res. 2018;46:4547-59.
- [CrossRef] [PubMed] [Google Scholar]
- Acromioclavicular joint injuries. Orthop Clin North Am. 2000;31:177-87.
- [CrossRef] [PubMed] [Google Scholar]
- Clavicular hook plate may induce subacromial shoulder impingement and rotator cuff lesion - Dynamic sonographic evaluation. J Orthop Surg Res. 2014;9:1-9.
- [CrossRef] [PubMed] [Google Scholar]
- The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: Longitudinal construct validity and measuring self rated health change after surgery. BMC Musculoskelet Disord. 2003;4:11.
- [CrossRef] [PubMed] [Google Scholar]
- Clavicular hook plate for lateral end fractures: A prospective study. Injury. 2006;37:277-83.
- [CrossRef] [PubMed] [Google Scholar]
- Constant score assessment of shoulder function is strength measurement useful? J Bone Joint Surg Br. 2002;84:197-9.
- [Google Scholar]




