
Translate this page into:
Fracture dislocation of scaphoid in association with polytrauma: Diagnostic and management considerations
Address for correspondence: Dr. Venkatraman Bhat, 309, Greenwoods Apartment, Bommasandra, Bengaluru - 560 099, Karnataka, India. E-mail: bvenkatraman@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Chavre S, Bhat V, Chandra Sekar BC, Ram MA. Fracture dislocation of scaphoid in association with polytrauma: Diagnostic and management considerations. J Orthop Allied Sci 2016;4:84-6.
Abstract
Isolated fracture of the scaphoid with the dislocation of the proximal bony component is a rare abnormality, usually encountered in a high-energy injury. Prompt diagnosis is essential for preferentially considering open reduction and fixation. Careful image analysis is necessary to exclude more frequent injuries such as lunate dislocation and establish encroachment of carpal tunnel or injury to median nerve. This presentation presents imaging and management consideration of the patient with the scaphoid fracture with dislocation of proximal component encountered in association with polytrauma.
Keywords
Internal fixation
isolated scaphoid fracture
scaphoid fracture dislocation

Introduction
Scaphoid injury constitutes relatively common form of wrist injury. Often, injury to scaphoid is associated with injury to carpal bones or proximal articular components of wrist joint. However, isolated scaphoid injury, especially the one associated with dislocation of part of scaphoid component, is extremely rare.[1] Prompt identification of scaphoid fracture dislocation and exclusion of other common scaphoid injury is important for prompt management of patient. Conventional radiographic methods as well as magnetic resonance imaging (MRI) have vital role in defining osseous and ligamentous component of injury. Early open reduction with internal fixation and repair of ligament is preferable for optimal outcome.[1,2,3] Hereby, we report a case of scaphoid fracture dislocation in association of polytrauma and discuss diagnostic and management considerations.
Case Report
A 28-year-old male patient was brought to the emergency service, following a fall from the second floor of the building. He was in a state of the altered consciousness due to associated head injury and multiple bony injuries. His hemoglobin was 6 g % due to blood loss at multiple bleeding sites. On computed tomography evaluation of the head, he was found to have intracranial hemorrhage in association with frontoparietal linear fracture. In addition, he had fracture of the left femur, dislocation of left elbow, and injury to the left wrist. Frontal and lateral radiographs of the wrist demonstrated fracture of the scaphoid with the ventral and proximal displacement of the bony fragment. In the frontal view, the alignment of the proximal and distal carpal bones was disrupted at the location of scaphoid with resultant gap in the region of the lunate-scaphoid interface. Lateral radiograph clearly demonstrated rotated, displaced bony fragment of scaphoid anterior to the distal radius [Figure 1]. The patient had no signs of the median nerve injury. The patient was immediately taken to the operating room for evaluation of intracranial hematoma after restoring hemoglobin level by blood transfusion. At the same sitting, he underwent open reduction of wrist and fixation of the scaphoid with the Kirschner wires [Figure 2]. Displaced bony fragment of the scaphoid was visible lateral to the median nerve at surgery [Figure 3]. Fragment was repositioned and injured scapholunate and radio-scapho-triquetral ligaments were repaired. No evidence of median nerve damage was noted. The patient recovered postoperatively and was stable on the 10th postoperative day.

- Frontal and lateral wrist radiograph showing evidence of fracture of scaphoid with a gap between scaphoid and lunate. Dislocated scaphoid fragment is displaced proximally, and on ulnar side (black arrow). Lunate is located in normal position (black circle). Additional chip fractures are noted along lateral and dorsal aspect of radius (white arrows)
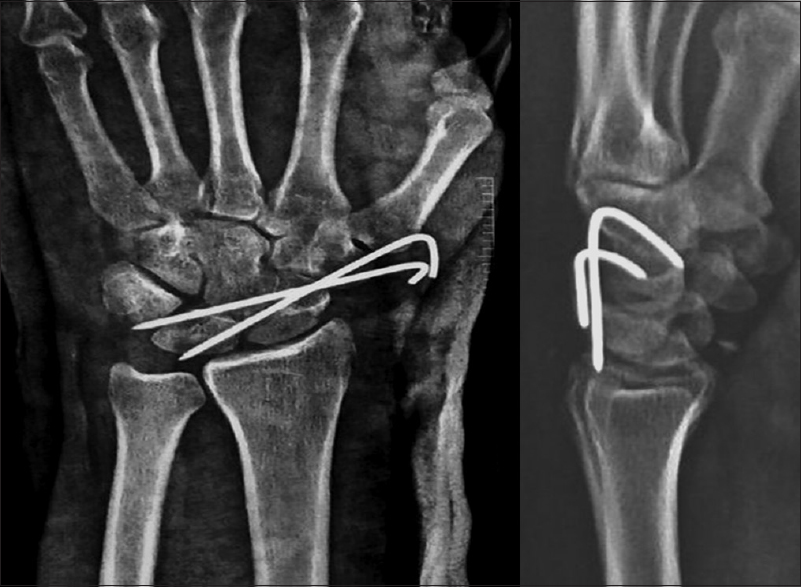
- Frontal and lateral wrist radiograph after open reduction and metal pin fixation showing repositioning of scaphoid
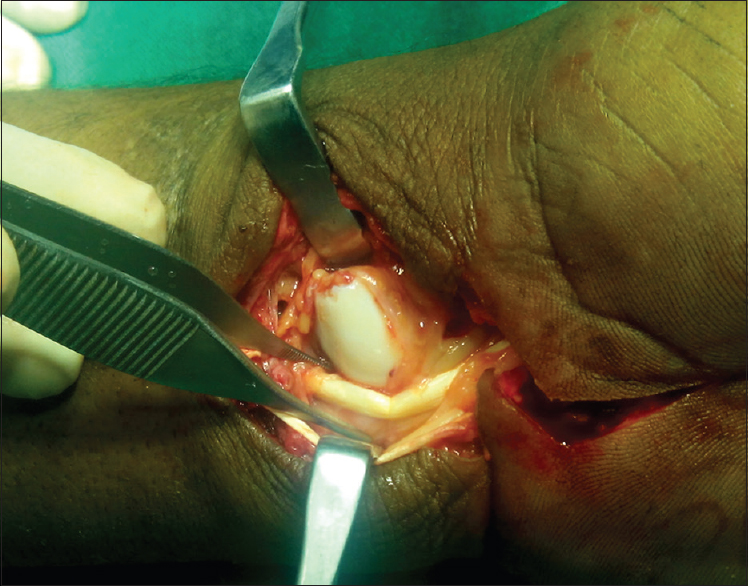
- Operative photograph demonstrates displaced scaphoid fragment lateral to median nerve
Discussion
Isolated scaphoid dislocation or fracture dislocation is a relatively rare injury often seen in patients with high-velocity trauma while patients trying to hold on to an object while falling. The resultant injury could be isolated dislocation/fracture dislocation of the scaphoid (Type 1) or result in injury to capito-hamate joint with the dislocated scaphoid (Type 2).[1,2] Our patient was observed to catch on to a rope while falling. Scaphoid injury, in our patient, is seen with minor radial avulsion injuries and with other major injuries as described. Dislocation of ipsilateral elbow joint in our patient appears to share the same mechanism of injury. Scaphoid has a stabilizing role in wrist movement. Proximal pole is anchored to lunate and distal pole attached to trapezium and trapezoid by strong ligaments. The mechanism of injury often either a hyperextension and ulnar deviation leading to disruption of the scaphoradial, scapholunate ligament, radio-scaphocapitate ligament, and the long radiolunate ligament.[3] Typically, scaphoid shows ventral and radial displacement.[4] Both closed and open reductions have been attempted in the limited number of reported cases. Optimal anatomic reduction is difficult with the close reduction, and hence the open reduction is recommended for the better outcome.[1] More recent, the studies recommend open reduction and ligament reconstruction as a preferred modality of treatment. Review of literature (published in English) reports few cases of the scaphoid fractures with anterior dislocation of the proximal fragment. One such review documents only nine reported cases.[5] Some patients present with the carpal tunnel syndrome.[6] Avascular necrosis is another likely complication in the dislocated fragment of scaphoid.
Radiological assessment of the scaphoid dislocation is performed with plain radiography, typically with frontal, lateral views. Major differential consideration in the frontal projection is to exclude more common injury such as lunate dislocation. There are similarities between the two entities; however, demonstration of the normal location of the lunate in the lateral view will clinch the diagnosis of scaphoid injury. Review of few reported fracture dislocation of the scaphoid revealed that displaced fragment located proximally and on radial side. Our case showed grater displacement of fracture fragment and displacement toward the ulnar side. Furthermore, on surgery, displaced fragment was located lateral to the median nerve. Nerve injury and disruption of carpel tunnel appear to be important sequel of this injury. There is a recommendation to perform magnetic resonance examination in case of the scaphoid dislocations to delineate the extent of ligament injury and also evaluate the changes of avascular necrosis.[5] MRI should be performed if reconstruction of ligament is planned. We were not able to consider these options because of the acute clinical situation demanding prompt management. Our patient, after 6-month follow-up, showed no significant movement disability of wrist joint. Furthermore, there was radiographic restoration of scaphoid alignment. This report is intended to increase the awareness of this rare wrist injury and to highlight the need for proper preoperative assessment and management.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- An unusual variation of luxation of the wrist: External vertical luxation. Apropos of a case. Review of the literature. Ann Chir Main Memb Super. 1995;14:159-66.
- [CrossRef] [PubMed] [Google Scholar]
- Isolated carpal scaphoid dislocation. Acta Orthop Traumatol Turc. 2012;46:68-71.
- [CrossRef] [PubMed] [Google Scholar]
- Isolated scaphoid fracture with anterosuperior dislocation of the proximal fragment. Chir Main. 2011;30:298-301.
- [CrossRef] [PubMed] [Google Scholar]
- Isolated scaphoid fracture with palmar dislocation of the proximal fragment. BMJ Case Rep 2015, July 6, 2015 10.1136/bcr-2015-n210333
- [CrossRef] [PubMed] [Google Scholar]
- Isolated volar fracture-dislocation of the scaphoid with acute carpal tunnel syndrome: A case report. Acta Orthop Belg. 2010;76:552-4.
- [Google Scholar]




