
Translate this page into:
Foraminoplasty
Address for correspondence: Dr. Anand Kavi, B-1001/Kapil Vastu, Karve Nagar, Near Vithal Mandir, Pune - 411 052, Maharashtra, India. E-mail: anandskavi@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Kavi A. Foraminoplasty. J Orthop Allied Sci 2018;6:S13-5.
Abstract
Transforaminal endoscopic lumbar spine surgery has evolved leaps and bounds in the last 10 years, and as such, it is now not limited to simple contained herniation. It can now be successfully done for central, extraforaminal, extruded, and migrated herniations, which were considered bad indications when the procedure was limited to central intradiscal nucleotomy or debulking. With better understanding of the foraminal anatomy, more bold approaches to intervertebral foramen are now being undertaken. Moreover, with further development in instruments, such as motorized burrs and lasers, we can now successfully treat the foraminal and lateral canal stenosis. With the advantages of Transforaminal endoscopic techniques, such as use of local anesthesia, minimal skin incision, no need for neuromuscular retraction, and no excessive bone removal, with minimal approach-related morbidity, allows it to be applied safely in extremes of age, with early return to normal life. The procedure of foraminoplasty is vital to achieve these extended targets in Transforaminal endoscopic surgeries. The term foraminoplasty is used among the spine endoscopists to broadly describe the expansion of the foraminal boundaries and it is reversibly used to describe foraminotomy. However, foraminotomy is performed for widening the foramen to reach far off and difficult targets, whereas foraminoplasty is performed for decompression of neural structures in the treatment of foraminal and lateral stenosis. In this article, we discuss both the procedures. To understand the principles and successfully employ the technique, let us first understand the foraminal anatomy.
Keywords
Foraminoplasty
foraminotomy
foraminal stenosis
lateral recess stenosis

Introduction
Intervertebral foramen is an important portal through all the basics and advanced procedures are being carried out in current scenario.[1,2] The foramen in the lumbar spine is a pear-shaped or inverted teardrop shaped osteofibrous canal bounded by the following:
Superior: Inferior surface of pedicle of superior vertebra.
Ventral: Lower part of the vertebral body, intervertebral disc, and superior endplate and part of the inferior vertebra.
Dorsal: Inferior articular process, superior articular process (SAP), and ligamentum flavum
Inferior: Pedicle of the inferior vertebra
Contents: Exiting root in the superior part of the foramen dorsal root ganglion and the exiting root traverse the laterally.
Foraminal ligaments
Foraminal artery
Foraminal veins
Fat and connective tissue
Traversing root and the dura on the medial side.
Out of the four walls of the foramen, only the ventral wall, i.e., the posterior annulus and the disc, is yielding, whereas the superior, inferior, and dorsal walls are unyielding. Furthermore, the shape and dimensions of the foramen change and constrict in the degenerative spine.[3-6]
Safe Triangle of Kambin
Endoscopic approach to the foramen is through the safe triangle of Kambin formed between the exiting root, traversing root, and superior endplate of inferior vertebra.[2,3]
Foraminotomy
To approach various targets, we need to enlarge the boundaries of the foramen, which is called foraminotomy. It can be achieved by the following methods.
Trephine
This is done with larger diameter 4–6 mm metal trephines under fluoroscopic guidance.
Procedure
Under local anesthesia, spinal needle is inserted posterolaterally via the safe triangle of Kambin, under the facet, in the lower part of the foramen (as upper part has exiting nerve, so to prevent injury), the needle is anchored in the posterior annulus, guide wire is inserted and the needle is removed, and subcentimeter skin incision is taken and the dilator (obturator) is railroaded on the guide wire, followed by the cannula, with its opening directed toward the facet and the tang protecting the exiting nerve.
Now, the trephine is inserted, and with light hammering, the bone of the superior facet is cut under the fluoroscopic guidance. The trephine should not cross the medial pedicular line in anteroposterior view. Usually, the bone cut gets impacted in the trephine and is removed with it [Figure 1]. Now, the endoscope is inserted to carry out the intended procedure under vision.
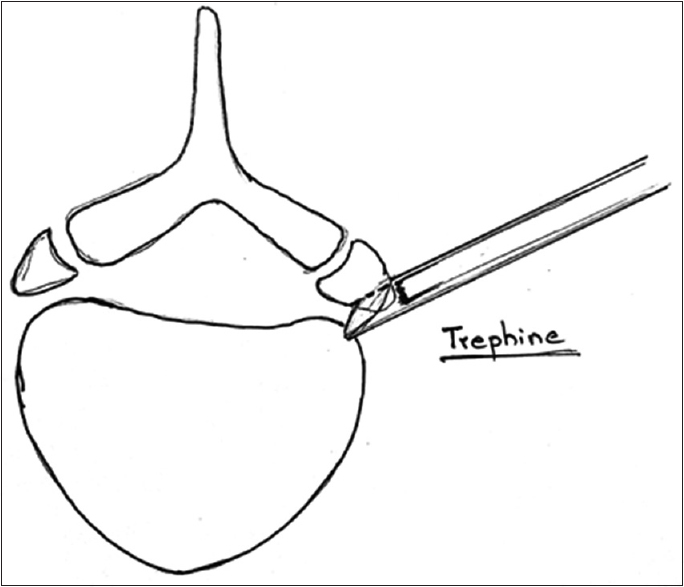
- Foraminoplasty using Trephine
Tomshidi needle and the drills (Thomas Hoogland technique)
In this method, the Tomshidi needle is anchored in the SAP of facet in the lower part of the foramen, the guide wire is inserted, and then the manual drills of gradually increasing sizes are inserted over the guide wire; to enlarge the foraminotomy, this is also done under fluoroscopic guidance.
Although both these techniques are done under fluoroscopic guidance, they are blind endoscopically. Endoscopic foraminotomy can be done by Schubert et al.[7]
Motorized Burr
Once the access is developed via the safe triangle of Kambin, in the foramen, the cannula is placed in the posterior annulus, under the SAP, protecting the exiting nerve. Endoscope is inserted, structures are identified by probing, and radiofrequency (RF) cautery is used to clear the soft connective tissue over the bone. Then, high-speed motorized burr and drills are inserted through the endoscope and are used to cut the bone under vision, until the ligament flavor is reached medially, under continuous irrigation [Figure 2].
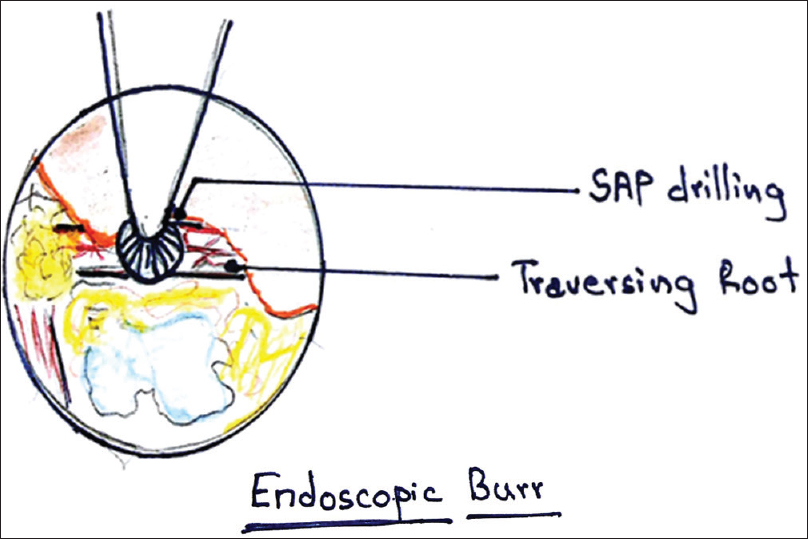
- Foraminoplasty with endoscopic Burr
Laser
Similar to the endoscopic burr technique, once the approach is established and structures identified with probing under endoscopic view. A side-firing laser probe is inserted through the endoscope; pulsed holmium YAG laser beam is used to remove the bone and hard tissues in the foramen [Figure 3].[8,9]
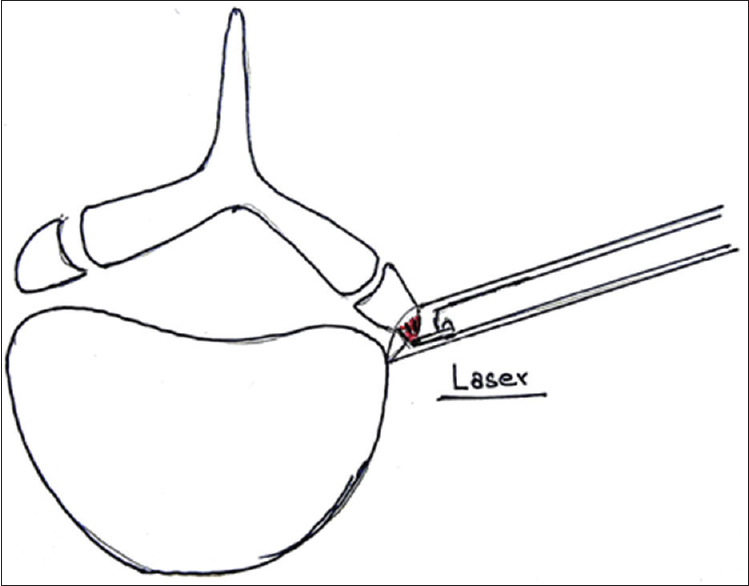
- Endoscopic Laser Foraminoplasty
Foraminotomy for Approach
Outside in approach
As popularized by Thomas Hoogland, wherein manual drills are employed to widen the foramen's posterior walls and to land on the disc to target the herniated fragment, in an attempt to prevent going intradiscally.[7]
Superior migrated fragment
To target the up migrated fragment, the needle approach is also modified accordingly; to target the tip of the SAP in the superior foramen, access is developed and the tip of the SAP is removed under the endoscopic vision to reach the axilla of the existing root and approach the tail of the up migrated fragment.[10,11]
Inferior migrated fragment
The spinal needle is inserted such that the needle tip is positioned in the lower foramen over the pedicle; oblique pediculectomy and lower foraminotomy are done to target the down migrated fragment.
Foraminoplasty for Stenosis
It is the procedure to free the exiting and the traversing nerve from the epidural space to beyond the external boundaries of foramen, and as such, it is not just limited to undercutting of the facet or just decompression be discectomy alone.
It can be divided into three steps.
Needle placement
Skin marking is done such that the skin entry point is between 8 cm and 12 cm lateral to the midline, under fluoroscopic guidance. Needle is landed either on the SAP or on the posterior annulus, on the disc surface (coinciding with the medial pedicular line and posterior vertebral line in biplane endoscopy). The needle is replaced by the guide wire and followed by the dilator in the intraforaminal space, over which the beveled working cannula is introduced, such that the bevel opening is toward SAP and the tang protects the exiting root; this position is confirmed under fluoroscopy.
Facet undercutting
After successfully landing over the facet, endoscope is introduced and under vision gentle probing is done to identify the structures, RF cautery is used to clear the surface of the bone. The hypertrophic SAP is then undercut using motorized burr under endoscopic vision; drilling is done until the lateral edge of ligamentum flavum is reached. After undercutting is completed, the endoscope can be advanced further to visualize the anatomical structures in more detail.
Final decompression
Complete decompression is done using punches, graspers, RF, and laser, by removal of the hypertrophied ligamentum flavum, foraminal ligaments, extruded disc fragments, and bony osteophytes., After which we can observe the free and pulsating exiting nerve, traversing nerve, and lateral edge of the dura.
Thus, we free the neural structures of anything that is compressing, distorting, or irritating the nerve in the foramen.[12,8]
Technical Tips
This procedure should be undertaken with sufficient experience in transforaminal endoscopy.
Precise landing in the foramen is the key to successful procedure
Exiting root should always be protected with the operating cannula
Soft tissue decompression should be done strictly under vision.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Full Endoscopic Spinal Surgery Techniques: Advancements, Indications, and Outcomes. Int J Spine Surg. 2015;20(9):17.
- [Google Scholar]
- Arthroscopic microdiscectomy: An alternative to open disc surgery. Mt Sinai J Med. 2000;67:283-7.
- [Google Scholar]
- Arthroscopic and endoscopic spine surgery via a posterolateral approach. Minimally Invasive Spine Surgery: A Surgical Manual 2006:331-45.
- [Google Scholar]
- Anatomy of the lumbar spinal nerves in the intervertebral foramen. Clin Anat. 1991;4:366-72.
- [Google Scholar]
- Clinical anatomy and significance of the lumbar intervertebral foramen: A review. J Anat Soc India. 2015;64:166-73.
- [Google Scholar]
- Endoscopic transforaminal nucleotomy with foraminoplasty for lumbar disk herniation. Oper Orthop Traumatol. 2005;17:641-61.
- [Google Scholar]
- Transforaminal endoscopic lumbar decompression & foraminoplasty: A 10 Year prospective survivability outcome study of the treatment of foraminal stenosis and failed back surgery. Int J Spine Surg 2014:8.
- [Google Scholar]
- Percutaneous endoscopic decompression for lumbar spinal stenosis. Expert Rev Med Devices. 2014;11:605-16.
- [Google Scholar]
- Percutaneous endoscopic approach for highly migrated intracanal disc herniations by foraminoplastic technique using rigid working channel endoscope. Spine (Phila Pa 1976). 2008;33:E508-15.
- [Google Scholar]
- Transforaminal percutaneous endoscopic lumbar discectomy for very high-grade migrated disc herniation. Clin Neurol Neurosurg 2016:147.
- [Google Scholar]
- Endoscopic foraminal decompression for failed back surgery syndrome under local anesthesia. Int J Spine Surg 2014:8.
- [Google Scholar]




