
Factors contributing to superior gluteal nerve injury during cephalomedullary nailing of femoral fractures
Address for correspondence: Dr. Ahmed A. Khalifa, Department of Orthopaedic and Traumatology, Qena Faculty of Medicine and Its University Hospital, South Valley University, Kilo 6 Qena-Safaga Highway, Qena 83523, Egypt. E-mail: ahmed_adel0391@med.svu.edu.eg
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Khalifa AA, Ahmed AM, Khaled M, Said EA. Factors contributing to superior gluteal nerve injury during cephalomedullary nailing of femoral fractures. J Orthop Allied Sci 2019;7:4-7.
Abstract
Operative treatment of femoral fractures using intramedullary nailing is considered as the gold standard technique; despite safety and minimal invasiveness, it is prone to some complications, of these is the persistent abductor lurch even after complete fracture healing. In this review, we are discussing the possible factors which may endanger the superior gluteal nerve during cephalomedullary nailing of the femur.
Keywords
Cephalomedullary
femoral
nailing
superior gluteal nerve

Introduction
Cephalomedullary nails have become a gold standard for treating femoral fractures since the 1980s,[1-3] because nailing is a minimally invasive and relatively easy procedure with mechanical advantages.[4,5] However, residual complications may develop such as hip pain, stiffness, limping, decreased walking distance, and difficulty with stairs.[6-11] These symptoms are primarily attributed to postoperative hip abductor weakness described by the patients as a lurch in their gait. Surgeons often neglect this complaint, or the lurch is so mild that it may go unnoticed.[12] It is postulated that the decreased abductor strength is partially related to superior gluteal nerve (SGN) injury during nail insertion.
Anatomical Overview
The anatomy of the SGN and its surgical implications have been discussed in different anatomic studies [Figure 1].[9,13-18] The lumbosacral plexus gives off the SGN which then runs through the greater sciatic foramen above the piriformis muscle. The SGN usually follows a “spray pattern” where it spreads out along the intermuscular plane between the gluteus medius and gluteus minimus muscles. The most inferior branch of the nerve provides innervation to the gluteus minimus muscle and continues anteriorly to pierce the fused anterior edges of the gluteal muscles to supply the tensor fasciae latae muscle. Another distribution is called “transverse neural trunk pattern” where short branches arise to supply the gluteal muscles from a long trunk terminating in the tensor fasciae latae muscle.[19-21] The inferior main branch, the principal neuronal supply of the gluteus medius, is thought to be the most susceptible part of the SGN to injury during reaming.[17,20]
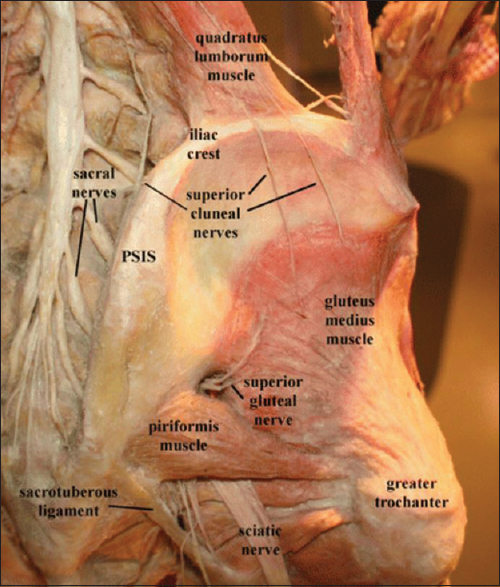
- Course and anatomical relations of the superior gluteal nerve (Image courtesy of Andrea Trescot, MD)
Patient's Position
Nailing can be performed with the patient lying in either the supine or the lateral decubitus position. Although the supine position is more common, it permits only a limited amount of adduction and flexion of the limb, and therefore, it may be challenging to create an entry point.[22] In a study by Ansari Moein et al.,[14] an antegrade femoral nail was introduced in ten cadavers lying in the supine position. In two of them, the inferior branch of the SGN was found to be at high risk of injury, being <5 mm from the surgical incision in the gluteus medius.
In contrast, a higher degree of both flexion and adduction (up to 30°) can be achieved with the lateral decubitus position on the fracture table which provides more accurate access to the correct point of entry.[22] Another reported method is manual traction with the patient in the so-called sloppy lateral position, in which the affected limb was elevated with a bolster placed beneath the buttock allowing an even higher amount of hip adduction (up to 45°).[23] The safety of these positions was tested by Ozsoy et al.[20] who noticed that higher degrees of flexion and adduction, as is possible with the patient in the lateral position on a fracture table or in the sloppy lateral position on a radiolucent table, the SGN is displaced superiorly and anteriorly and thus at less risk of being injured.
Surgical Incision
An optimal skin incision (location and length) should provide both safety (for soft tissues including the SGN) and accessibility for the nail instruments. Jacobs and Buxton[21] were thefirst to describe a “safe area” as much as 5 cm proximal to the tip of the greater trochanter [Figure 2]. Despite the technical difficulty to obtain an instrumentation trajectory that is “in line” with the femoral canal, particularly in muscular and obese patients,[24] it was determined that a more distal skin incision, 2–5 cm proximal to the tip of the greater trochanter, should be used. However, the exact location of this safe area remained controversial, because the distance between the branches of the SGN and the greater trochanter may alter in relation to many variables including body height and pelvic anatomy.[25] This controversy (regarding incision location and length) was further proved by Ozsoy et al.[20] who found that the SGN is located in an average distance of only 7 mm (range, 0–17 mm) away from the instrumentation and the nail path when a piriformis entry intramedullary nail is inserted through the traditional distal incision.
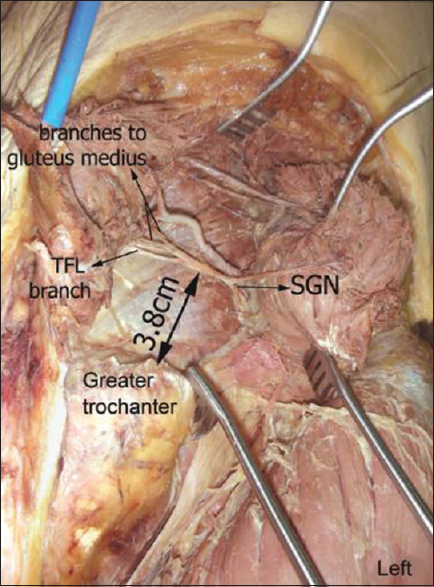
- Relation of the tip of the greater trochanter (Image courtesy of Dr. Nihal Apaydin)
On the other hand, a more proximal skin incision is considered advantageous as it makes it easier to obtain an “on-axis” trajectory to the femoral canal. The safety of this approach was questioned till evaluated by Lowe et al.[26] They positioned the leg in 15° of adduction and 10° of flexion to make an incision 1–2 cm distal to the most proximal subcutaneous border of the iliac crest aligned with the femoral shaft. No injuries to the main trunk or any of its branches were reported. As demonstrated by the authors, the gluteus medius muscle acted as a natural “barrier” or “buffer” to protect the SGN as well as its branches which lie on its “undersurface.” In addition, the prominence of the iliac crest and gluteal tubercle prevents excessive medialization of the instrument and nail trajectory providing an extra protective effect. However, these protective effects can be achieved only when the procedure is performed by experienced hands.
Nailing Entry Point
There has been a conflict regarding the optimal portal of nail insertion to minimize soft-tissue injury [Figure 3]. The safety of piriformis and greater trochanter tip entry was examined by both cadaveric and clinical studies.
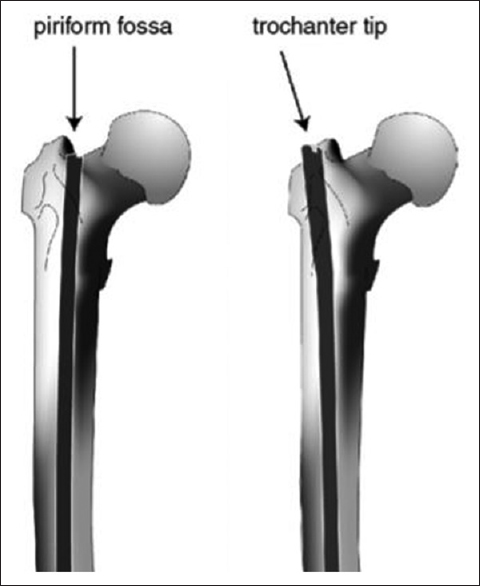
- Entry points of a cephalomedullary femoral nail (Image courtesy of Dr. Ansari Moein)
Studies by Ansari Moeinet al.[14,19,27] concluded that there is no difference regarding the risk of SGN injury when it comes to the entry point. The nerve was either preserved in both groups or at similar risk of injury. On the other hand, Khan and Knowles[28] found the average distance from the greater trochanter tip to the lowest branch of the SGN is ≥5 cm farther than the nerve's distance from the piriformis fossa entry portal. Therefore, using the greater trochanter tip as an entry point may reduce the risk of damage to these nerve branches. These results were supported by another clinical study where five of the patients in the piriformis fossa group had an abnormal electromyography with evidence of acute injury of the SGN directly after operation followed by reinnervation.[29]
Conclusion
After reviewing the possible factors, which can endanger the SGN during cephalomedullary femoral nailing, we believe that greater trochanter entry point represents a safer approach than the piriformis entry, and the lateral decubitus position, although less commonly utilized, seems to offer more protection for the SGN and its branches. The proximity of the skin incision does not affect the risk of SGN injury, but rather makes the procedure technically easier.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- The gamma nail – A significant advance or a passing fashion? J Bone Joint Surg Br. 1992;74:329-31.
- [CrossRef] [PubMed] [Google Scholar]
- Unstable trochanteric fractures: The role of lateral wall reconstruction. Int Orthop. 2010;34:125-9.
- [Google Scholar]
- Treatment of unstable trochanteric fractures. Randomised comparison of the gamma nail and the proximal femoral nail. J Bone Joint Surg Br. 2004;86:86-94.
- [CrossRef] [Google Scholar]
- Nail or plate fixation of intertrochanteric hip fractures: Changing pattern of practice. A review of the American Board of Orthopaedic Surgery Database. J Bone Joint Surg Am. 2008;90:700-7.
- [CrossRef] [PubMed] [Google Scholar]
- Gamma nails revisited: Gamma nails versus compression hip screws in the management of intertrochanteric fractures of the hip: A meta-analysis. J Orthop Trauma. 2009;23:460-4.
- [CrossRef] [PubMed] [Google Scholar]
- Intramedullary nailing of femoral fractures in adolescents. Clin Orthop Relat Res. 1998;350:85-9.
- [CrossRef] [Google Scholar]
- Femoral neck fracture: A complication of femoral nailing. Injury. 1995;26:319-21.
- [CrossRef] [PubMed] [Google Scholar]
- Iatrogenic fractures of the femoral neck during closed nailing of the femoral shaft. J Bone Joint Surg Br. 1994;76:293-6.
- [CrossRef] [Google Scholar]
- Abduction strength following intramedullary nailing of the femur. J Orthop Trauma. 1997;11:93-7.
- [CrossRef] [PubMed] [Google Scholar]
- Proximal thigh pain after femoral nailing. Causes and treatment. J Bone Joint Surg Br. 1997;79:738-41.
- [CrossRef] [Google Scholar]
- Early rehabilitation following surgical fixation of a femoral shaft fracture. Phys Ther. 2006;86:558-72.
- [CrossRef] [PubMed] [Google Scholar]
- Abductor weakness in intertrochantric fractures operated with PFN and its management. Indian J Orthop Surg Radiol Anat. 2018;4:230-3.
- [CrossRef] [Google Scholar]
- Is there a gluteus medius tendon injury during reaming through a modified medial trochanteric portal? A cadaver study. J Orthop Trauma. 2007;21:617-20.
- [CrossRef] [PubMed] [Google Scholar]
- Soft tissue injury related to choice of entry point in antegrade femoral nailing: Piriform fossa or greater trochanter tip. Injury. 2005;36:1337-42.
- [CrossRef] [PubMed] [Google Scholar]
- Entry point soft tissue damage in antegrade femoral nailing: A cadaver study. J Orthop Trauma. 2001;15:488-93.
- [CrossRef] [PubMed] [Google Scholar]
- Damage to the superior gluteal nerve after the hardinge approach to the hip. J Bone Joint Surg Br. 1996;78:903-6.
- [CrossRef] [PubMed] [Google Scholar]
- The surgical anatomy of the superior gluteal nerve and anatomical radiologic bases of the direct lateral approach to the hip. Surg Radiol Anat. 1994;16:253-8.
- [CrossRef] [PubMed] [Google Scholar]
- Does the direct lateral approach to the hip joint jeopardize the superior gluteal nerve? Clin Anat. 1991;4:123-8.
- [CrossRef] [Google Scholar]
- Soft tissue anatomy around the hip and its implications for choice of entry point in antegrade femoral nailing. Clin Anat. 2008;21:568-74.
- [CrossRef] [PubMed] [Google Scholar]
- Risk of superior gluteal nerve and gluteus medius muscle injury during femoral nail insertion. J Bone Joint Surg Am. 2007;89:829-34.
- [CrossRef] [PubMed] [Google Scholar]
- The course of the superior gluteal nerve in the lateral approach to the hip. J Bone Joint Surg Am. 1989;71:1239-43.
- [CrossRef] [Google Scholar]
- Fractures of lower extremity. In: Canale ST, ed. Campbell's Operative Orthopaedics. Philadelphia: Mosby; 2003.
- [Google Scholar]
- Femoral nailing without a fracture table. Clin Orthop Relat Res. 1996;332:119-25.
- [CrossRef] [PubMed] [Google Scholar]
- Intramedullary nailing of femoral fractures in morbidly obese patients. J Trauma. 1994;36:208-10.
- [CrossRef] [PubMed] [Google Scholar]
- Reliability of the safe area for the superior gluteal nerve. Clin Orthop Relat Res. 2003;412:111-6.
- [CrossRef] [PubMed] [Google Scholar]
- Risk of injury to the superior gluteal nerve when using a proximal incision for insertion of a piriformis-entry reamed femoral intramedullary nail: A cadaveric study. J Bone Joint Surg Am. 2012;94:1416-9.
- [CrossRef] [PubMed] [Google Scholar]
- Intramedullary femoral nailing through the trochanteric fossa versus greater trochanter tip: A randomized controlled study with in-depth functional outcome results. Eur J Trauma Emerg Surg. 2011;37:615-22.
- [CrossRef] [PubMed] [Google Scholar]
- Damage to the superior gluteal nerve during the direct lateral approach to the hip: A cadaveric study. J Arthroplasty. 2007;22:1198-200.
- [CrossRef] [PubMed] [Google Scholar]
- Functional outcome after antegrade femoral nailing: A comparison of trochanteric fossa versus tip of greater trochanter entry point. J Orthop Trauma. 2011;25:196-201.
- [CrossRef] [PubMed] [Google Scholar]




