
Translate this page into:
Extrapulmonary Mycobacterium tuberculosis-induced carpal tunnel syndrome presented with rice body
Address for correspondence: Dr. Ali Tabrizi, Clinical Research Development Unit, Imam Khomeini Hospital, Urmia University of Medical Sciences, Modaress Street, Ershad Boulevard, Urmia 57157 81351, Iran. E-mail: dr.tabrizi.ali@hotmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Alamdari MT, Tabrizi A, Afshar A. Extrapulmonary Mycobacterium tuberculosis-induced carpal tunnel syndrome presented with rice body. J Orthop Allied Sci 2019;7:34-6.
Abstract
Skeletal involvements are less likely in Mycobacterium tuberculosis (TB), and it is even rarer in the hand. Flexor tenosynovitis from M. tuberculosis concomitant with median nerve involvement has been rarely reported, and it usually presents with symptoms of carpal tunnel syndrome (CTS). In this report, we introduced a patient with symptoms of CTS with rice body in the volar wrist synovium membrane and extrapulmonary tuberculosis (TB). Rice bodies were presented in synovium and histological study indicated the inflammatory granulomatous with necrosis caseous. Surgical debridement with excision of the involved synovium and irrigation was performed. Twelve-month treatment with anti-TB medication regimen was successful.
Keywords
Carpal tunnel syndrome
extrapulmonary tuberculosis
tenosynovitis
tuberculosis

Introduction
Tuberculosis (TB) has been considered as a rare disease in Western countries, but in the third world and developing countries, it is a common and endemic disease.[1] Skeletal involvement is unusual and occurs in 10%–15% of TB patients.[1,2] The possibility of upper-extremity involvement, especially in hand, is very rare. Skeletal TB can produce a wide range of soft tissue or bone involvement which can lead to various clinical symptoms.[3] TB can be various manifestations in radiography and clinical examination.[4] Depending on the slow clinical course and progression of the disease, in many cases, it is detected lately or misdiagnosed.[5] Mycobacterium-induced extrapulmonary TB can be manifested by various symptoms including spondylitis, septic arthritis, osteomyelitis, myositis, bursitis, subcutaneous abscess, and tenosynovitis.[6] In this report, we introduced a patient with symptoms of carpal tunnel syndrome (CTS) with rice body in the volar wrist synovium membrane and extrapulmonary TB.
Case Report
A 39-year-old male, rural farmer, referred to the orthopedic clinic with chronic paresthesia in radial side distal phalanx and wrist pain 6 months ago. Physical examination showed positive Tinel and Phalen tests at the wrist with mild swelling in the volar side of the wrist without any stiffness of the hand and fingers. Electromyography and nerve conduction studies confirmed the clinical diagnosis of CTS. A distal motor latency of >4.5 ms and a sensory latency of >3.5 ms were consistent with CTS diagnosis. Chest and hand X-ray conventional radiographs were normal. No history of previous illness was noted. Wrist joint movements were painful. He was a candidate for surgical decompression. Based on our patient's management, there was no laboratory test before operation. Using local anesthesia, carpal tunnel was released by volar approach in wrist. The median nerve was compressed, and the epineurium was thickened. After opening the flexors retinaculum, we encountered multiple large rice bodies along the flexor tendons and the compressed median nerve [Figures 1 and 2]. All rice bodies were removed. Irrigation with normal saline was done. Biopsy samples from rice bodies, synovium, and flexor retinaculum were sent for pathological tests. Laboratory tests after operation revealed that white blood cell count was 9600 mm− 3, erythrocyte sedimentation rate was 65 mm/mm in the 1st h and C-reaction protein was 25 mg/l (normal value < 10 mg/l). The sample culture was negative in terms of bacteriology, and no microorganism grew. Histological studies showed the inflammatory granulomatous with necrosis caseous [Figure 3]. TB skin test (purified protein derivative) was performed, and induration was measured which was higher than 15 mm so that positive skin test was determined. After the operation, the pain and the sensory loss were improved, but active flexion of the index finger was difficult and painful due to chronic synovitis. Chemotherapy included anti-TB drugs and oral nonsteroidal anti-inflammatory drugs. Anti-TB treatment regimen constituted isoniazid, rifampicin, pyrazinamide, and streptomycin prescribed for 2 months, and it was continued with rifampicin and isoniazid for 10 months. After a 12-month follow-up, the patient had no clinical recurrence of the disease and had full active and passive motion of the wrist and fingers.

- Clinical image in operation time shows tenosynovitis and rice bodies along the flexor tendons
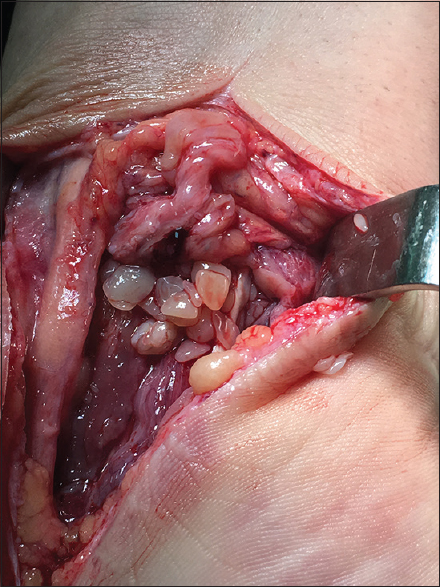
- Multiple large rice bodies near to the median nerve
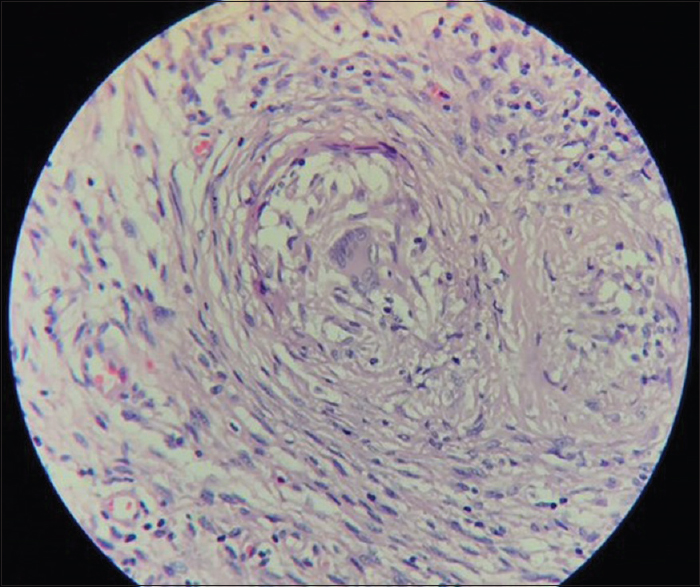
- Histological findings based on synovial-tissue biopsy showing long-term inflammation with a caseating granuloma
Discussion
Infection caused by Mycobacterium tuberculosis in developing countries and the third world is a major health problem, and it can affect any part of the body with various manifestations.[1,2] In musculoskeletal system, spinal vertebra involvement usually occurs in 30%–50%. Soft-tissue involvement is rare. Tendon sheath or nerve sheath involvement is generally due to hematogenous spread. Other conditions to infection include lymphogeneous or direct contamination, which may induce infection in soft tissues.[7] Tenosynovitis due to M. tuberculosis is reported to be <1% of the cases.[3,4] Following the involvement of soft tissue with TB, the inflammatory reaction is triggered; therefore, tissue exudation and granulation occur.[7] Such an inflammatory reaction occurs in the tissue bursa. Rice bodies can be presented in <50% of cases with M. tuberculosis soft-tissue infection. However, it was not specific for M. tuberculosis infection. In other inflammatory diseases, the rice body can be observed. Usually, it can be formed in rheumatoid arthritis, seronegative arthritis, systemic lupus erythematosus, and osteoarthritis.[3,4,7] Early diagnosis and appropriate treatment for M. tuberculosis infection is important to restore the performance. Usually, skeletal infection caused by M. tuberculosis slowly progresses, which makes its early diagnosis difficult.[3,7] In cases of soft-tissue infection, especially the tendon sheath, there are nonspecific manifestations including pain, swelling, and nerve impairment due to compression effect (paresthesia and numbness) and due to different symptoms that cause misdiagnosis.[3,4] Based on case series studies of flexor tenosynovitis from M. tuberculosis, usually concomitant with median nerve involvement is induced symptoms of CTS. In patients with late diagnosis, poor functional outcome can occur.[3] In 1982, Janier et al. reported chronic tenosynovitis with CTS for thefirst time in a female patient a few weeks after she wounded herself with a pasteur pipette containing bacillus Calmette–Guerin cultures.[5] The diagnosis of TB tenosynovitis is complicated and a long delay is frequently observed between the onset of the patient's symptoms and the correct diagnosis.[3,4] Usually, the patients are misdiagnosed with nonspecific synovitis or rheumatoid synovitis before the correct diagnosis of TB. Biopsy and pathological study can be helpful in correct diagnosis. A history of respiratory symptoms is possible; moreover, skeletal TB involvements, pulmonary symptoms, and respiratory system involvement may not be observed.[3,4] Treatment by isoniazid, rifampicin, pyrazinamide, and streptomycin for 2 months should be completely performed; and the treatment should be also continued by rifampicin and isoniazid for 10–14 months.[5,6] According to the studies, skeletal involvement of TB needs long-term treatment.[5-7] The mentioned therapy was very successful in our patient. A study of Kotwal and Khan on hand involvement of TB showed that 75% of cases exhibited favorable clinical outcomes by employing the mentioned medications.[6] Surgical debridement with excision of involved synovium and irrigation continued with anti-TB medication regimen for 12 months was successful. In endemic areas of M. tuberculosis, careful examination and attention to any swelling in the wrist are of great importance. Precautionary laboratory examinations and imaging study must be performed before carpal tunnel releases.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Acknowledgments
This study was financially supported by Urmia University of Medical sciences.
Conflicts of interest
There are no conflicts of interest.
References
- Skeletal tuberculosis presenting as a small cystic lesion in the medial femoral condyle. Arch Bone Jt Surg. 2013;1:112-5.
- [Google Scholar]
- C. botulinum neurotoxin types A and E: Isolated light chain breaks down into two fragments. Comparison of their amino acid sequences with tetanus neurotoxin. Biochimie. 1989;71:1193-200.
- [CrossRef] [PubMed] [Google Scholar]
- Tenosynovitis and carpal tunnel syndrome from Mycobacterium tuberculosis – A rare manifestation of extrapulmonary tuberculosis. Acta Reumatol Port. 2010;35:82-4.
- [Google Scholar]
- Tuberculous synovitis with “rice bodies” presenting as carpal tunnel syndrome. J Hand Surg Am. 1988;13:574-6.
- [CrossRef] [PubMed] [Google Scholar]
- Carpal tunnel syndrome due to Mycobacterium bovis BCG (author's transl) Sem Hop. 1982;58:977-9.
- [Google Scholar]
- Tuberculosis of the hand: Clinical presentation and functional outcome in 32 patients. J Bone Joint Surg Br. 2009;91:1054-7.
- [Google Scholar]
- Tuberculosis tenosynovitis with multiple rice bodies of the flexor tendons in the wrist: A case report. Int J Surg Case Rep. 2016;27:129-32.
- [CrossRef] [PubMed] [Google Scholar]




