
Translate this page into:
Does Matrilin-3 Gene Polymorphism and Primary Knee Osteoarthritis Have a Association in Indian Population?
Address for correspondence: Dr. Vipin Kumar, Department of Orthopaedics, ERA's Lucknow Medical College and Hospital, Sarfarazganj, Lucknow - 226 003, Uttar Pradesh, India. E-mail: drvipingupta17@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Kumar V, Shah R, Khan AA, Pandey A, Khambhati US, Mishra NK. Does matrilin-3 gene polymorphism and primary knee osteoarthritis have a association in Indian population? J Orthop Spine 2020;8:22-6.
Abstract
INTRODUCTION:
Osteoarthritis (OA) is estimated to be the fourth-leading cause of disability. Results from several studies have shown that OA is inherited and may vary by joint site. Twin family and studies have estimated the heritable component of OA to be between 50% and 65% with larger genetic influences for hand and hip OA than for knee OA. In view of the possible role of matrilin-3 (MATN-3) gene in primary OA, a number of studies during the past few years have evaluated the role of MATN-3 polymorphism in OA in various countries.
SUBJECTS AND METHODS:
The study was conducted in the Department of Orthopedics and Department of Bio-Technology in ERA's Lucknow Medical College and Hospital, Lucknow. Necessary blood (complete blood count, erythrocyte sedimentation rate, C reactive protein, rheumatoid arthritis factor, serum uric acid) and X-ray of the bilateral knee in investigations anteroposterior and lateral view on standing for confirmation of the diagnosis. Cases will be diagnosed with OA based on the Kellgren-LawrenceKL) Grading System. Five millimeters of venous blood will be drawn and poured in ethylenediaminetetraacetic acid-containing tubes. The DNA samples will be isolated from peripheral blood lymphocytes by the standard phenol extraction method. MATN-3 genotyping done from the blood.
RESULTS:
Statistically, the difference between the two groups was not significant (P = 0.603). No significant difference in genotype was observed among different KL-grades (P = 0.945).
CONCLUSION:
The findings of the present study showed that MATN-3 polymorphism does not seem to be associated with primary knee OA in the Indian population.
Keywords
Cartilage
Indian population
knee
matrilin-3 gene
primary osteoarthritis

Introduction
Osteoarthritis (OA) is estimated to be the fourth leading cause of disability.[1] It probably is the most common disease of joints in adults throughout the world.[2] Knee OA accounts for >80% of the disease's total burden[3] and as per an estimate in the US population, it affects at least 19% of adults aged 45 years and older.[4]
The risk of developing OA is determined by both systemic and local factors. Several systemic factors have been identified; these may act by increasing the susceptibility of joints to injury, by direct damage to joint tissues, or by impairing the process of repair in damaged joint tissue. Local factors are most commonly biomechanical in nature and adversely affect the forces applied to the joint. Some of the important risk factors associated with OA are obesity and metabolic disease, age, sex, ethnicity and race, genetics, nutrition, smoking, bone density, and muscle function.[5]
Results from several studies have shown that OA is inherited and may vary by joint site. Twin and family studies have estimated the heritable component of OA to be between 50% and 65% with larger genetic influences for hand and hip OA than for knee OA.[6,7]
Kerkhof et al.[8] reported that the C allele of rs3815148 on chromosome 7q22 was associated with a 1.14-fold increased prevalence of knee and/or hand OA and also with a 30% increased risk of knee OA progression. Keeping in view the significance of genetic factors in the development of primary OA, a number of genome-wide association studies have attempted to seek the relationship between genetic changes and OA. It has been demonstrated in these studies that single-nucleotide polymorphisms (SNPs) in various genes are related to an increased risk of knee OA, including collagen genes (COL1A1, COL2A1, COL9A1, and COL11A2) as well as genes encoding interleukin-1 receptor, transforming growth factor-β1, cartilage matrix protein 1, tissue inhibitor of metalloproteinase 3, insulin-like growth factor-1, bone morphogenetic protein, Vitamin D receptor, aggrecan-1, secreted frizzled-related protein 3, growth differentiation factor 5, and cyclooxygenase-2.[9,10,11] In recent years, matrilin-3 (MATN-3) gene, has been recognized to play a role in the synthesis of cartilage. It is expressed in chondroblasts and osteoblasts but not in hypertrophic chondrocytes.[12,13] Distribution of MATN-3 protein, an extracellular matrix protein, has also been seen in cartilaginous tissues, including the articular and epiphyseal cartilages.[12] In view of the possible role of MATN-3 gene in primary OA, a number of studies during the past few years have evaluated the role of MATN-3 polymorphism in OA. It has been shown that a single-nucleotide polymorphism of the MATN-3 gene is associated with primary OA in patients with different ethnicities.[14,15] However, there are no such studies from India so far. Hence, the present study was carried out to assess the association between MATN-3 gene polymorphism and primary knee OA in Indian patients at a center in North India.
Subjects and Methods
The study was conducted in the Department of Orthopedics and the Department of Bio-Technology in ERA's Lucknow Medical College and Hospital, Lucknow. It was a case-controlled study conducted between November 2015 and October 2019. After ethical approval from the institutional ethics committee, 100 patients were recruited into the study.
Inclusion criteria
Inclusion criteria are as follows:
Cases age group 40–75 years (of either sex) who were isolated diagnosed cases of knee OA
Controls, age group 40–75 years (of either sex) with age- and sex-matched with cases (±5 years)
Control group patients were those patients who never had any signs or symptoms of knee OA or any other arthritis.
Exclusion criteria
Isolated patella-femoral OA
Secondary OA due to trauma or deformity
Inflammatory arthritis such as rheumatoid arthritis (RA), SLE and seronegative arthritis
Malignancy
Bilateral knee replacements.
After enrolment, the recruited cases and controls were explained the purpose and relevance of the study. Necessary blood investigations (complete blood count, ESR, C-reactive protein [CRP], RA factor, serum Uric acid), and X-ray of bilateral knee In anteroposterior and lateral view on standing for confirmation of the diagnosis. Cases will be diagnosed with OA based on the Kellgren-Lawrence (KL) Grading System.
Matrilin-3 Genotyping
Procedure for DNA extraction
Five millimeters of venous blood will be drawn and poured in ethylenediaminetetraacetic acid containing tubes. The DNA samples will be isolated from peripheral blood lymphocytes by the standard phenol extraction method. The DNA concentration will be determined by the spectrometer and stored at −20°C till the time of DNA extraction. PCR was performed in a reaction volume of 50 μL using Dream Taq Green PCR Master Mix (Thermo Fisher Scientific Inc.,) with 25 μL dream taq green PCR master mix, 3 μL (5 pmol) forward primer, 3 μL (5 pmol) reverse primer, 5 μL (10 ng) template DNA, 14 μL nuclease-free water.
The PCR primers used were: 5′d GGACAGGATCCCACAAAAAG 3′ as a forward primer and 5′d GAAAGAGGGGCTACAACAGG 3′ as a reverse primer.
The amplification protocol followed was: Initial denaturation at 95°C for 10 min, followed by 35 cycles of denaturation at 95°C for 1 min, annealing at 60°C for 1 min, extending at 72°C for 1 min, and a final extension at 72°C for 10 min in a thermocycler. The resultant PCR products showed a single fragment at 501 bp by gel electrophoresis. In total, 10 μL of 501-bp product was digested with ten units of BSEYI restriction enzyme at 37°C for 10 h. Digestion products were visualized on a 3% agarose gel containing 2% ethidium bromide. RFLPs were coded as Bb, where the uppercase letter signified the absence of the restriction site, and the lowercase letter signified the presence of the site. The wild-type genotype (CC), was coded as bb, which produced a double band at 149 and 352 bp; heterozygotes (CN), will be coded as Bb, which will produce three bands at 501, 149, and 352 bp; and homozygote polymorphic genotype (NN), was coded as BB, which produced only one band at 501 bp.
Results
Knee OA were comprised the case group of study, while the remaining 50 (50%) were control of the study. Demographically, matched healthy individuals who comprised the control were taken out of the 100 subjects enrolled.
In cases, genotype bb and Bb had a frequency of 20% and 80%, respectively. There was no BB genotype.
In controls, genotypes bb, Bb and BB had a frequency of 20%, 78%, and 2%, respectively.
Thus, genotype BB was seen in only 1 (2%) of controls as compared to none of the cases. Statistically, the difference between the two groups was not significant (P = 0.603).
Allele b and B frequency was 60% and 40%, respectively, in cases as compared to 59% and 41% in controls. On evaluating the data statistically, the difference was not found to be statistically significant (P = 0.885).
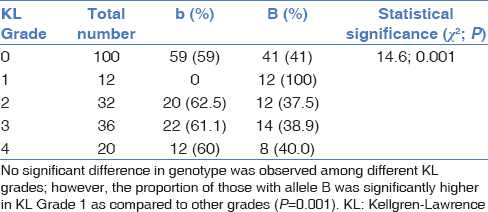
Proportion of those with allele B was significantly higher in KL Grade 1 as compared to other grades (P = 0.001).
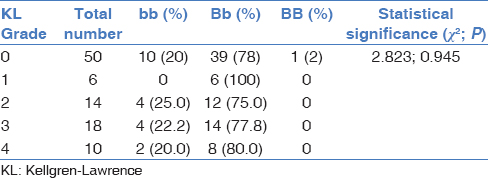
No significant difference in genotype was observed among different KL grades; however, the proportion of those with allele B was significantly higher in KL Grade 1 as compared to other grades (P = 0.001).
Discussion
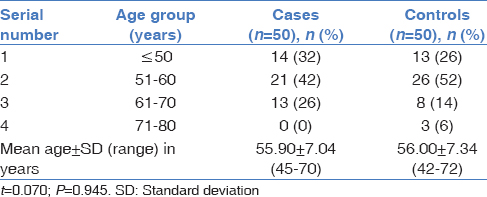
In the present study, the age of knee OA patients ranged from 45 to 70 years. Among different studies reviewed by us for Martilin-3 gene polymorphism, the mean age has been shown to vary from 57.34 years to 69.8 years.[14,15] The mean age of patients in the present study was slightly younger. In the present study, the majority of patients were males. However, according to epidemiological studies, reported a higher risk of all types of OA among females is higher as compared to males.[5]
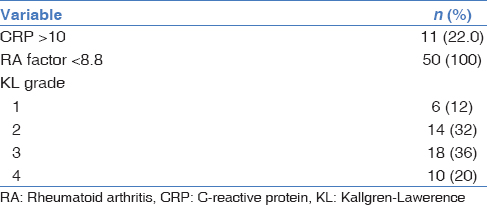
In the present study, body mass index (BMI) of cases ranged from 19.10 to 27.30 kg/m2 with a mean of 23.72 ± 2.35 kg/m2. In their study, Diab et al.[14] reported the mean BMI of their cases as 22 ± 2.14 kg/m2, which is lesser than the present study. As far as the clinical profile of the patients was concerned, a total of 11 (22%) had CRP >10, RA factor was positive in all the cases, and there was a dominance of KL Grade 2 and 3 patients (68%). As far as the grade is concerned, the profile of patients in the present study was similar to that reported by Diab et al.,[14] who also had 60% of their patients with KL Grade 2 and 3. Gu et al.[15] also showed a dominance of Grades 2 and 3 in their study sample (85.7%).
In the present study, MATN3, rs8156070 (SNP6) polymorphism studies in cases and controls showed, Genotype bb, Bb and BB in 20%, 80%, and 0% of cases as compared to 20%, 78%, and 2% of controls, thus showing no significant difference between two groups. At allele level, alleles b and B were present in 60% and 40% of cases and 59% and 41% of controls, thus showing no significant difference between the two groups. In comparison with the present study, Diab et al.[14] in an Egyptian population observed expression of bb, Bb and BB genotypes in 24%, 60% and 14% of cases and 12%, 40% and 48% of controls and allele frequency b and B in 54% and 46% of cases as compared to 32% and 42% of controls and reported a significant difference between two groups both for genotypes and alleles. However, in our study, we found expression of genotype BB to be relatively less prevalent in both cases as well as controls and did not find a significant difference between the two groups. Gu et al.[15] in another study conducted in Chinese population reported the expression of genotypes bb, bB and BB in 47.8%, 40.4%, and 11.9% of cases as compared to 44.5%, 39.3%, and 14.2% of controls and found that the difference between two groups was significant only for frequency of genotype BB.
In another study, Pullig et al.[16] found expression of bb, bB, and BB genotypes in 97.7%, 2.3%, and 0% of cases as compared to 97.5% and 2.5% of controls in a German population and failed to find out any significant difference association of MATN3, SNP6 polymorphism with knee OA. In the present study, we also carried out a comparison of MATN3, SNP6 polymorphism with relation to KL grade in cases and found no significant association at genotype level but found expression of allele B to be significantly higher in lower grades as compared to higher KL grades.
Limitations within the of study, we failed to derive a significant association between MATN3, SNP6 polymorphism, and knee OA risk in the Indian population. As far as the correlation of our results with contemporary work from other parts is concerned, it shows that this association seems to be effective in only select ethnicities [Tables 1-7].



Conclusion
Statistically, there was no significant difference between cases and controls with respect to age, gender, marital status, BMI and occupational profile.
No significant difference in genotype and allele frequency was observed between cases and controls. In cases, none of the patients showed BB genotype, whereas 1 (2%) control showed BB genotype.
Financial support and sponsorship
The author acknowledge the support of the Department of biochemistry and Department of biotechnology Ear's Lucknow Medical College in conducting the study.
Acknowledgment
The authors acknowledge the support of the Department of Biochemistry and Department of Biotechnology Era's Lucknow Medical College in conducting the study.
Conflicts of interest
There are no conflicts of interest.
References
- The epidemiology of osteoarthritis in Asia. Int J Rheum Dis. 2011;14:113-21.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of hip and knee osteoarthritis. Epidemiol Rev. 1988;10:1-28.
- [CrossRef] [PubMed] [Google Scholar]
- Years lived with disability (YLDs) for 1140 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2143-96.
- [Google Scholar]
- Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum. 2008;58:26-35.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology and burden of osteoarthritis. Br Med Bull. 2013;105:185-99.
- [CrossRef] [PubMed] [Google Scholar]
- Genetic influences on osteoarthritis in women: A twin study. BMJ. 1996;312:940-3.
- [CrossRef] [PubMed] [Google Scholar]
- Predisposition to familial osteoarthrosis linked to type II collagen gene. Lancet. 1989;1:924-7.
- [CrossRef] [PubMed] [Google Scholar]
- A Genome-Wide Association Study identifies a locus on chromosome 7q22 to influence susceptibility for osteoarthritis. Arthritis Rheum. 2010;62:499-510.
- [Google Scholar]
- A meta-analysis of genome-wide association studies identifies novel variants associated with osteoarthritis of the hip. Ann Rheum Dis. 2014;73:2130-6.
- [Google Scholar]
- Genomics of osteoarthritis. Curr Opin Rheumatol. 2003;15:634-40.
- [CrossRef] [PubMed] [Google Scholar]
- Prostaglandins and bone: Physiology and pathophysiology. Osteoarthritis Cartilage. 1999;7:419-21.
- [CrossRef] [PubMed] [Google Scholar]
- Molecular structure and tissue distribution of matrilin-3, a filament-forming extracellular matrix protein expressed during skeletal development. J Biol Chem. 2000;275:3999-4006.
- [CrossRef] [PubMed] [Google Scholar]
- Changes of matrilin forms during endochondral ossification. Molecular basis of oligomeric assembly. J Biol Chem. 2000;275:32628-34.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical significance of Matrilin-3 gene polymorphism in Egyptian patients with primary knee osteoarthritis. Eur J Rheumatol. 2017;4:200-4.
- [CrossRef] [PubMed] [Google Scholar]
- MATN3 gene polymorphism is associated with osteoarthritis in Chinese Han population: A community-based case-control study. ScientificWorldJournal. 2012;2012:656084.
- [CrossRef] [PubMed] [Google Scholar]
- MATN3 (matrilin-3) sequence variation (pT303M) is a risk factor for osteoarthritis of the CMC1 joint of the hand, but not for knee osteoarthritis. Ann Rheum Dis. 2007;66:279-80.
- [CrossRef] [PubMed] [Google Scholar]




