
Translate this page into:
Diabetic muscle infarction
Address for correspondence: Dr. Gautam Rava, GNRC Hospital, Dispur, Guwahati - 781 005, Assam, India. E-mail: gautamrava@outlook.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Rava G, Goswami N, Mahanta P. Diabetic muscle infarction. J Orthop Allied Sci 2018;6:48-50.
Abstract
Diabetic muscle infarction is an underdiagnosed and underreported complication of long-standing diabetes mellitus occurring in a middle-aged person with symptoms simulating infective or inflammatory condition most commonly involving the thigh muscles, legs, and arms, in decreasing order of frequency. Magnetic resonance imaging is the diagnostic modality of choice showing diffuse hyperintense signal involving the muscles and deep fascia on T2 images. It is a self-limiting condition which resolves simply by rest and analgesic; therefore, being aware of this condition is necessary to avoid unnecessary interventions.
Keywords
Diabetes mellitus
muscle infarction
thigh pain

Introduction
Diabetic muscle infarction (DMI) or diabetic myonecrosis (DM) is a rare but known complication of poorly controlled diabetes mellitus mostly affecting the lower extremities. It presents as acute or insidious onset thigh or leg pain in a person with long-standing history of diabetes mellitus, thereby mimicking other inflammatory or infective condition, making clinical and radiological diagnosis difficult. Just over a 100 cases have been reported in the literature so far.[1] Therefore, it is prudent to be aware of this condition in an orthopaedic clinic for proper diagnosis and avoiding any unnecessary intervention.
Case Report
A 35-year-old female, nonsmoker and nonalcoholic, presented to us with a history of insidious onset right thigh pain of a few months duration. There was no history of fever or any discharge from the affected area nor there any kind of joint pain. She gave a history of needle aspiration from the affected area in a local facility elsewhere, which did not yield any significant diagnostic result. She was a known case of diabetes mellitus dependent on insulin, and hypothyroidism on regular medication and hemoglobin-E disease.
On presentation, she was afebrile and rest of the general and systemic examinations were within normal limits. Local examination of the affected area showed tenderness and induration over anterior and posterior aspect of midthigh. Skin appeared normal without any signs of inflammation or sinus scar. Joint examination proximally and distally was unremarkable. Neurovascular examination of the affected extremity was normal.
We considered the differential diagnosis as – cellulitis, thigh abscess, necrotizing fasciitis and deep vein thrombosis – ruled out due to – duration of symptoms, absence of fever, and other signs of inflammation.
Roentgenograms and ultrasound Doppler were also performed which did not show any abnormality. A magnetic resonance imaging (MRI) of the right thigh was obtained [Figures 1 and 2].

- Axial T2-weighted image showing hypersignal changes involving vastus medialis and semitendinosus muscle
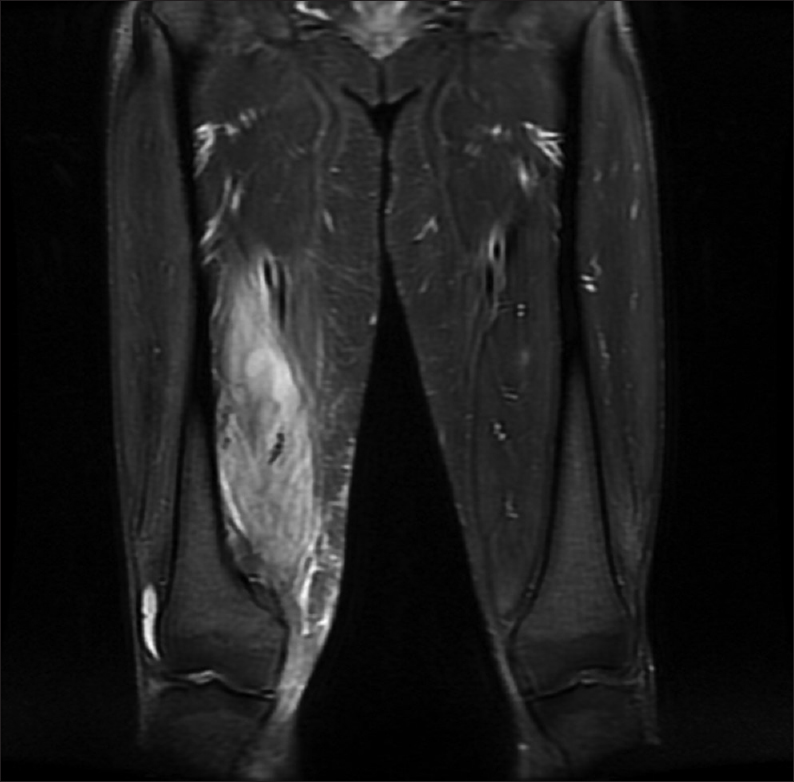
- Coronal T2-weighted image showing hyperintense signal changes in the vastus medialis muscle with strong peripheral enhancement and the dimension of the lesion is 2.4 cm × 2 cm × 3.5 cm
MRI was reported as possibility of pyomyositis or intramuscular abscess, involving the vastus medialis muscle and semitendinosus muscle along with the subcutaneous tissue edema.
Laboratory investigations were performed, the significant findings being poorly controlled blood sugar in spite of regular insulin therapy (fasting blood sugar – 240 mg/dl, postprandial blood sugar – 213 mg/dl), raised erythrocyte sedimentation rate (82), and increased glycosylated hemoglobin (8.8%). Other routine tests-complete blood count, serum creatinine, and thyroid-stimulating hormone were within normal limits.
Following the reports from the MRI examination, a drainage procedure was planned after obtaining informed consent from the patient. As per the patient's request for general anesthesia (GA), and sterile preparation and draping, posterior part of the thigh was explored, by giving direct incision around 5 cm long, over the indurated part over semitendinosus muscle. After incising the deep fascia and muscle sheath, muscle fibers were exposed. We did not find any collection in the operated site. However, the muscle fibers were found to be pale. There were no signs of inflammation. Hence, we decided to take samples both from the deep fascia of thigh (1.6 cm × 0.6 cm × 0.3 cm) and semitendinosus muscle fibers (2.3 cm × 0.5 cm × 0.4 cm) for histopathological examination (HPE). We also explored anteriorly over the vastus medialis muscle in a similar way with same intraoperative findings. Wounds were closed in layers. Antiseptic dressing was applied and prophylactic antibiotics started. The patient was discharged home the next day with the advice of bed rest, prophylactic antibiotics, nonsteroidal anti-inflammatory drugs (NSAIDs), and proper glycemic control with diet and insulin.
HPE report was obtained, which was as follows:
Semitendinosus muscle – degenerating necrotic myofibers with patchy acute neutrophil infiltrate and red blood cells – features are consistent with myonecrosis.
Deep fascia – fibrofatty tissue and focal tendon with patchy mild perivascular chronic infiltrate. No evidence of granuloma or vasculitis was seen.
Discussion
Angervall and Stener[2] in 1965 suspected tumor mass in the thigh, in two diabetes patients and after HPE of the tissue concluded muscular degeneration following ischemia.
More than 100 cases have been described in the literature since then.[1] The initial episode of DMI occurred in thigh muscles in 80% of the time, followed by lower leg muscles in 17%, concurrently in both the thigh and leg muscles in 2%, and rarely in upper extremity in 1%. The mean age of presentation was 42 years with a predilection towards female diabetic patients.[3]
The pathogenesis of DMI has not been clearly defined.[3] Many theories have been put forward, one possibility being diabetic microangiopathy and arteriosclerosis[4] which results in an intense inflammatory response, edema, hyperemia, and reperfusion leading to the generation of reactive oxygen radicals and form pressure within the fascial compartment, ultimately leading to muscle ischemia and infarction.[1]
Although described in person with advanced diabetes and with advanced microvascular complications in the form of nephropathy, retinopathy, or neuropathy in almost 97% of the patients,[1] our patient did not have yet developed any such complications.
The key clinical features related to DMI were[5] – DMI presents as acute muscular pain and swelling most commonly in the lower extremities in a person with poorly controlled DM, without history of trauma and afebrile on presentation. Routine laboratory investigations are nonspecific. MRI is the investigation of choice, which typically shows a hyperintense signal on T2-weighted images and an isointense to hypointense signal on T1-weighted images from the affected muscle, with associated perifascial, perimuscular, and/or subcutaneous edema. The most characteristic finding in MRI is multifocal areas of involvement in a “patchwork pattern,” which is a key to differentiate from pyomyositis.[1]
A combination of bed rest, glycemic control, and NSAID therapy are the preferred treatment, with avoidance of surgery and physiotherapy in acute stage, as it may prolong the recovery time.[1,3,5] Symptoms usually resolve spontaneously within a few weeks to months.[6] However, a biopsy may be recommended if the presentation is atypical or when recovery is delayed, as in our case, that also in the form of needle or incisional biopsy since open biopsy has been associated with an increased risk of postoperative complications.[7]
The gross appearance in DMI is pale, whitish, and nonhemorrhagic muscles. Light microscopy shows large areas of muscle necrosis and edema, phagocytosis of necrotic muscle fibers, and appearance of granular tissue and collagen.[3] Later, stages may show mononuclear cell infiltration, fibrosis, and muscle fiber regeneration.
The short-term prognosis of DMI is generally good; however, recurrence rate has been found to be high (47.82%) with 8.69% involving the same muscle group and 39.13% occurring in a different group of muscles.[3] However, the long-term prognosis may be poor as the patients continue to have end-organ microvascular damage with death occurring within 5 years in majority of the patients.[8]
Therefore, awareness is the key to prevent unnecessary intervention in this self-limiting condition. Muscle biopsy can give a definitive diagnosis, but presently, not recommended at the moment due to procedure-associated complication and increase time to recovery. However, in our case, as the MRI report suggested to rule out pyomyositis or abscess formation, an operation was planned and carried out in the form of incisional biopsy. Therefore, we recommend this entity should be well known in the orthopaedic literature so that it can be appropriately managed.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Tumoriform focal muscular degeneration in two diabetic patients. Diabetologia. 1965;1:39-42.
- [CrossRef] [Google Scholar]
- Diabetic muscle infarction: An underdiagnosed complication of long-standing diabetes. Diabetes Care. 2003;26:211-5.
- [CrossRef] [PubMed] [Google Scholar]
- Case 29 1997: Case records of the Massachusetts general hospital. N Engl J Med. 1997;337:839-45.
- [CrossRef] [Google Scholar]
- Diabetic muscle infarction: A systematic review. BMJ Open Diabetes Res Care. 2015;3:e000082..
- [CrossRef] [PubMed] [Google Scholar]
- Diabetic myonecrosis: An atypical presentation. Case Rep Endocrinol. 2013;2013:190962..
- [CrossRef] [PubMed] [Google Scholar]




