
Translate this page into:
Debridement and Stabilization with Transpedicular Screws in Thoraco-Lumbar Spinal Tuberculosis
Address for correspondence: Dr. Lenin Ligu, Tomo Riba Institute of Health and Medical Sciences, Naharlagun, Arunachal Pradesh, India. E-mail: ortholenin@gmail.com
-
Received: ,
Accepted: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Ligu L, Jini M. Debridement and stabilization with transpedicular screws in thoraco-lumbar spinal tuberculosis. J Orthop Spine 2020;8:52-6.
Abstract
BACKGROUND:
The treatment for spinal tuberculosis (TB) remains a difficult and challenging decision-making process, given the lack of evidence and guidelines on the optimal treatment and management strategies. Conservative treatment options for spinal TB include methods such as immobilization using body casts or plaster beds, as well as a healthy diet.
MATERIALS AND METHODS:
The records of 26 patients who underwent posterior stabilization with pedicle screws and decompression with laminectomy for thoraco-lumbar TB with associated neurological deficit between January 2015 and December 2019 from hospitals were reviewed. The patients were followed up for a minimum of 24 months. In this study, we did not include patients with HIV co-infection.
Results:
In the present study, total 26 patients with thoraco-lumbar (T12-L1) TB. The study group consisted of 11 male and 15 female patients. The preoperative and postoperative mean kyphotic Cobb's angle were 23.1± 2.9° in males and 26.4 ± 2.4° in females and 8.9± 1.3° in males and 8.1± 1.4° females in the present study, respectively. At 1-year follow-up, the mean kyphotic angle was 11.2± 2.2° with a mean loss of kyphotic correction by 4.9± 1.1° in male. In our study, the C-reactive protein level decreased when compared preoperatively and postoperatively, 14.26 ± 1.8 in preoperatively, and 8.26 ± 1.2 postoperatively. Similarly, ESR value also decreased from 38.2 ± 2.3 mm to 21.6 ± 2.8. In addition, visual analog scale also decreased from 7.42 ± 1.1 to 2.9 ± 0.9.
Conclusions:
The procedure of one stage posterior debridement, decompression, and transpedicular screw fixation is effective and safe for treating thoracic and lumbar spinal TB.
Keywords
Debridement
spinal tuberculosis
stabilization
transpedicular screws

Introduction
The World Health Organization's Global tuberculosis (TB) Report 2019 ranked (TB) as a leading cause of death worldwide with 1.5 million deaths in 2018. An estimated 10 million people fell ill with TB worldwide: 5.7 million men, 3.2 million women, and 1.1 million children.[1] TB is a common form of osseous TB, accounting for 50%–60% of cases. The first modern description of spinal deformity and paraplegia resulting from spinal TB was described by Percival Pott in 1779.[2] Although uncommon, spinal TB still occurs even in both developed and developing countries.[3]
The treatment for spinal TB remains a difficult and challenging decision-making process, given the lack of evidence and guidelines on the optimal treatment and management strategies.[4] Conservative treatment options for spinal TB include methods such as immobilization using body casts or plaster beds, as well as a healthy diet. Following the introduction of anti-TB drugs, there has been a radical improvement in the prognosis of spinal TB patients. However, anti-TB drug treatments may alone not be suitable in cases where patients are at risk of instability, progression of neurological deficit, as well as patients who are refractory to medical treatment. Furthermore, the lengthy course of recumbency as advocated is both social and economic burden, as well as a personal burden to the quality of life of the patient.[5,6]
Anterior approach is usually indicated in cases where anterior and middle column of the vertebral bodies are affected with invagination of spinal canal with abscess or dead bones with symptoms of cord compression with involvement of less than 3 vertebra.[7,8]
Posterior approach only is mainly indicated in cases where there are more than 3 vertebra involvements with intact pedicles that will give adequate 3 column fixation and debridement will be through transforaminal route.[9]
The purpose of the study was to analyze the efficacy of all posterior approach and transpedicular screw fixation in treating thoracic and lumbar spinal TB and provide guidelines for the selection of appropriate surgical approaches. We retrospectively analyzed 26 cases treated surgically from January 2015 to December 2019.
As the state of Arunachal Pradesh doesn't have any intensive care unit or vascular surgery back up, the surgeon had opted for all posterior only approach as against any anterior approach, alone or combined.
Aims and objectives
Stabilization of unstable diseased spine with pedicle screws
Wide laminectomy whenever decompression required
Debridement through transforaminal route
Intertransverse grafting in cases where laminectomy done
Cobb's angle correction with patient positioning and compression over rods.
Materials and Methods
The records of 26 patients who underwent posterior stabilization with pedicle screws and decompression with laminectomy for thoraco-lumbar TB with associated neurological deficit between January 2015 and December 2019 from hospitals were reviewed. The patients were followed up for a minimum of 24 months. In this study, we did not include patients with HIV co-infection.
The diagnosis of spinal TB was made based on clinical symptoms, physical signs, laboratory findings, and radiological evidence. The American Spinal Injury Association score was used to evaluate the neurological function of patients. Visual analog scale (VAS) was used to evaluate several clinical factors including back pain for all patients. The Cobb's angle was used to assess the local kyphotic angle. The Oswestry disability index (ODI) score was used to evaluate the functional outcome of patients.
Only patients who had thoraco-lumbar TB with a neurological deficit or spinal instability were included in this study. Those patients who received conservative treatment, or who could not undergo vertebral fixation was excluded from the study.
Preoperative management
All cases were administered a chemotherapy regimen (isoniazid 300 mg/day, rifampicin 450 mg/day, ethambutol 750 mg/day, and pyrazinamide 750 mg/day) as soon as diagnosis was established. Preoperative hemoglobin and ESR levels needed to be higher than 100 g/L and higher than 40 mm/L, respectively, before surgery.
Operation technique
All patients underwent general endotracheal anesthesia, after which they were placed in the prone position on the spinal table. A standard dorsal midline was given. After incising skin and thoraco-lumbar fascia, the paraspinal muscles were thoroughly dissected with electrocautery till the bony landmarks were clearly identified. The spinous process in the center and laminas, facet joints, and transverse processes laterally were exposed.
Centering upon the diseased vertebrae, the two vertebrae above and two vertebrae below were inserted with pedicle screws. The debridement was carried out through transforaminal route as thoroughly as possible. In cases requiring decompression, wide laminectomy was done and the excised bone fragments were used as graft for intertranrverse fusion.
The prone positioning for the surgery itself attributes to around 5-10 degrees of spontaneous correction in kyphosis. Rest of the achievable correction was achieved through compression over the prebent rodson the pedicle screws.
The muscles and fascia were closed over a suction drain and skin was closed. Sterile dressing was put over the surgical wound. The amount of blood loss and the time of the surgery was noted.
Postoperative care
The suction drain was removed on 3rd post-operative day. Preventive antibiotic treatment was administered during the first 3 days after the operation. All patients were recommended to wear the bracing apparatus until bony fusion was observed by radiography. Patients resumed oral isoniazid, rifampicin, ethambutol, and pyrazinamide (HREZ) chemotherapy postoperatively, and then pyrazinamide was discontinued at 6 months. Patients continued to receive a regimen of HRE chemotherapy for 9-12 months (6HREZ/9-12HRE).
Results
In the present study, we evaluated the outcome of one-stage posterior debridement, decompression, and transpedicular screw fixation for the treatment of 26 patients with thoraco-lumbar (T12-L1) TB. The study group consisted of 11 male and 15 female patients [Table 1].

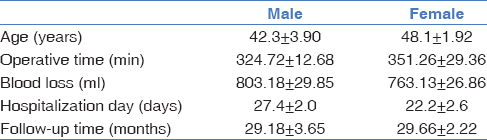
In Table 2, the mean age of the study was 42.3 ± 3.90 years in males and 48.1 ± 1.92 in females. The mean operation time was 324.72 ± 12.68 min in males and 351.26 ± 29.36 min in females. In our study, the mean blood loss of patients during surgery was 803.18 ± 29.85 ml in males and 763.13 ± 26.86 ml in females. The mean duration of hospital stay was 27.4 ± 2.0 days in males and 22.2 ± 2.6 days in females.
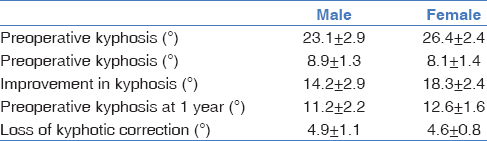
In Table 3, the preoperative and postoperative mean kyphotic Cobb's angle were 23.1 ± 2.9° in males and 26.4 ± 2.4° in females and 8.9 ± 1.3° in males and 8.1 ± 1.4° females in the present study, respectively. At 1-year follow-up, the mean kyphotic angle was 11.2° ± 2.2° with a mean loss of kyphotic correction by 4.9° ± 1.1° in males.
In Table 4, the Frankel scores were significantly higher at the final follow-up visit than those before surgery. No patient showed any deterioration of the neurological symptoms after surgery.

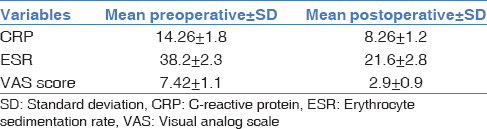
In Table 5, the C-reactive protein (CRP) level decreased when compared preoperatively and postoperatively, 14.26 ± 1.8 in preoperatively, and 8.26 ± 1.2 postoperatively. Similarly, ESR value also decreased from 38.2 ± 2.3 mm to 21.6 ± 2.8. In addition, VAS also decreased from 7.42 ± 1.1-2.9 ± 0.9.
Discussion
In recent years, based on incidence of spinal TB is considered as a medical condition, and surgery is required only in the presence of neurological deficits caused by spinal cord compression, disabling back pain, and spinal deformity in spite of ongoing anti-TB therapy.[10] Surgical approach in spinal TB has evolved from anterior to posterior. The anterior approach, popularized by Hodgson in 1960, was advocated traditionally in view of the predilection of the pathology of TB for the vertebral bodies and disc spaces.[3,11,12,13,14,15,16]
In the present study, we evaluated the outcome of one-stage posterior debridement, decompression and transpedicular screw fixation for the treatment of 26 patients with thoraco-lumbar (T12-L1) TB. The study group consisted of 11 males and 15 female patients. Mean age of the study was 42.3 ± 3.90 years in males and 48.1 ± 1.92 in females. The mean duration of hospital stay was 27.4 ± 2.0 days in males and 22.2 ± 2.6 days in females.
In our study, the mean blood loss of patients during surgery was 803.18 ± 29.85 ml in males and 763.13 ± 26.86 ml in females. This blood loss is lower than that reported by Rawall et al. who reported an average blood loss of 419 ml.[17,3] The mean blood loss was almost similar to our study reported by Pu et al. In Pu et al.'s study, the mean blood loss was 834.1 mL. No perioperative complications appeared in the present study.[18] Many experts believe that patients treated by the anterior approach experience greater blood loss. Many authors report increased surgical complications associated with the anterior approach, such as nerve and vascular injuries.[19]
The mean operation time was 324.72 ± 12.68 min in males and 351.26 ± 29.36 min in females. The operation time is longer than those reported by Pu et al. In his study, the mean duration of surgery was 390.2 min.[18] One patient presented slight perioperative complications in the present study and all recovered within 3 months, which did not affect the bony fusion of the spine. Furthermore, experts believe that patients treated by the anterior approach experience greater duration of the operation itself and the hospitalization period is longer than that of the posterior approach.[19]
The preoperative and postoperative mean kyphotic Cobb's angle were 23.1 ± 2.9° in males and 26.4 ± 2.4° in females and 8.9 ± 1.3° in males and 8.1 ± 1.4° females in the present study, respectively. At 1-year follow-up, the mean kyphotic angle was 11.2 ± 2.2° with a mean loss of kyphotic correction by 4.9 ± 1.1° in males. No significant loss of deformity correction was noted in these patients at the final follow-up. The result was similar to Zhang et al.'s study.[20] It was concluded from our study that the final outcome of one-stage posterior approach was satisfying. No intraoperative complications appeared in any of our cases. Thus, our study showed a satisfactory outcome in regard to the neurological dysfunction suffered by patients with thoraco-lumbar TB who were treated by a single-stage posterior debridement, decompression, and transpedicular screw fixation approach.
In the present study, the Frankel scores were significantly higher at the final follow-up visit than those before surgery. No patient showed any deterioration of the neurological symptoms after surgery. Improved at the final follow-up visit than those before surgery, there was no significant loss of kyphosis at final follow-up, and majority of the patients had achieved significant improvement in their daily activities (functional strength).
In our study, the CRP level decreased when compared preoperatively and postoperatively, 14.26 ± 1.8 in preoperatively, and 8.26 ± 1.2 postoperatively. Similarly, ESR value also decreased from 38.2 ± 2.3 mm to 21.6 ± 2.8. In addition, VAS also decreased from 7.42 ± 1.1-2.9 ± 0.9. The results were consistent with Zhang et al.' s study. The VAS scores of the patients were decreased from 5.5 before surgery to 0.9 at the final follow-up visit.[21]
However, surgery by a posterior approach is relatively simple, causes less trauma, and allows thorough debridement, fusion, and internal fixation to be achieved. There is no need to change the position of the patient during the operation, and fewer complications occur during the perioperative period. Furthermore, this approach can be used to effectively correct kyphosis and reduce internal fixation loosening and breakage.
The advantages of the posterior approach include reduced bleeding and shorter hospitalization and operation durations, in addition to relief of spinal nerve compression, corrected spinal kyphosis, regained spinal stability, and improved quality of life. Moreover, the posterior approach may be a better surgical method in patients with less involved spinal TB for the anterior column that is mainly affected by TB achieving spontaneous fusion.[22] In addition, posterior pedicle screw fixation may improve neurological recovery, as rigid stabilization enhances neurological improvement in patients with traumatic spinal cord injury.[23,24,25,26]
In this study, there was no significant difference in blood loss between the posterior approaches; we consider that this result may be related to the obvious learning curve of the posterior approach. However, a posterior-only approach also has some disadvantages, such as a narrow visual field, high technical requirements, dural injury, and surrounding tissue adhesion. Furthermore, a posterior approach destroys the posterior column, which has an influence on stability.[27]
Our research had some limitations. First, it was a retrospective study rather than a prospective study. Second, the sample size was small. In addition, posterior debridement bears the potential risk of TB spreading to the posterior healthy regions, resulting in infection diffusion and fistulas. Fortunately, these complications have not been observed in the present study. Second, the normal posterior column of spine was destroyed to achieve complete debridement and decompression in this procedure, which would affect the stability of the spine in theory. Long-term follow-up is needed to closely monitor the development of these potential complications.
Conclusions
Our study demonstrated that single-stage posterior debridement, decompression, and transpedicular screw fixation can be an effective treatment method for most patients with thoraco-lumbar (T12-L1) TB and associated neurological deficits, with good neurologic recovery, avoidance of kyphosis progression, and few complications.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 2019. Geneva: World Health Organization; Available from: https://apps.who.int/iris/bitstream/handle/10665/191102/ 9789241565059 _eng. pdf; jsessionid=257E179B7641F5CE7FD14BEF18488436? sequence=1. (accessed )
- Surgery for spinal tuberculosis: A multi-center experience of 582 cases. J Spine Surg. 2015;1:65-71.
- [CrossRef] [Google Scholar]
- Posterior approach in thoracolumbar tuberculosis: a clinical and radiological review of 67 operated cases. Musculoskelet Surg. 2013;97:67-75.
- [CrossRef] [PubMed] [Google Scholar]
- Spinal tuberculosis - Current management approach. Niger J Orthop Trauma. 2019;18:35-43.
- [CrossRef] [Google Scholar]
- One-stage posterior approach in the treatment of consecutive multi-segment thoracic tuberculosis with kyphosis. Turk Neurosurg. 2018;28:439-46.
- [Google Scholar]
- Surgical treatment of thoracolumbar spinal tuberculosis-a multicentre, retrospective, case-control study. J Orthop Surg Res. 2019;14:233.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior versus posterior approach in surgical treatment of tuberculous spondylodiscitis of thoracic and lumbar spine. Eur Spine J. 2016;25:1056-63.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy and safety of posterior versus combined posterior and anterior approach for the treatment of spinal tuberculosis: A meta-analysis. World Neurosurg. 2015;83:1157-65.
- [CrossRef] [PubMed] [Google Scholar]
- Debridement, interbody graft using titanium mesh cages, posterior instrumentation and fusion in the surgical treatment of multilevel noncontiguous spinal tuberculosis in elderly patients via a posterior-only. Injury. 2017;48:378-83.
- [CrossRef] [PubMed] [Google Scholar]
- Thoracic and lumbar tuberculous spondylitis treated by posterior debridement, graft placement, and instrumentation: a retrospective analysis in 19 cases. J Neurosurg Spine. 2005;3:450-8.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical results in patients with tuberculosis of the spine and severe lower-extremity motor deficits: a retrospective study of 48 patients. J Neurosurg Spine. 2007;6:320-6.
- [CrossRef] [PubMed] [Google Scholar]
- Tuberculosis of the spine: a fresh look at an old disease. J Bone Joint Surg Br. 2010;92:905-13.
- [CrossRef] [PubMed] [Google Scholar]
- Atypical spinal tuberculosis. Clin Orthop Relat Res. 2002;398:67-74.
- [CrossRef] [PubMed] [Google Scholar]
- Spinal tuberculosis: Current concepts. Global Spine J. 2018;8:96S-108S.
- [CrossRef] [PubMed] [Google Scholar]
- Isolated tuberculosis of posterior elements of spine: magnetic resonance imaging findings in 33 patients. Spine (Phila Pa 1976). 2002;27:275-81.
- [CrossRef] [PubMed] [Google Scholar]
- Instrumented circumferential fusion for tuberculosis of the dorso-lumbar spine. A single or double stage procedure? Int Orthop. 2012;36:315-24.
- [CrossRef] [PubMed] [Google Scholar]
- A posterior versus anterior surgical approach in combination with debridement, interbody autografting and instrumentation for thoracic and lumbar tuberculosis. Int Orthop. 2012;36:307-13.
- [CrossRef] [PubMed] [Google Scholar]
- Tuberculosis of the thoracic spine. A classification based on the selection of surgical strategies. J Bone Joint Surg Br. 2001;83:859-63.
- [CrossRef] [Google Scholar]
- Tuberculosis of the spine: a historical review. Clin Orthop Relat Res. 2007;460:29-38.
- [CrossRef] [PubMed] [Google Scholar]
- The outcomes of chemotherapy only treatment on mild spinal tuberculosis. J Orthop Surg Res. 2016;11:49.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of tuberculosis of the spine with neurologic complications. Clin Orthop Relat Res. 2002;398:75-84.
- [CrossRef] [PubMed] [Google Scholar]
- Tuberculosis of the craniovertebral junction: Is surgery necessary? Neurosurgery. 2006;58:1144-50.
- [CrossRef] [PubMed] [Google Scholar]
- Neurosurgical management of thoracic and lumbar vertebral osteomyelitis and discitis in adults: a review of 43 consecutive surgically treated patients. Neurosurgery. 1996;38:926-33.
- [CrossRef] [PubMed] [Google Scholar]
- Systematic review and meta-analysis: techniques and a guide for the academic surgeon. Ann Cardiothorac Surg. 2015;4:112-22.
- [Google Scholar]
- Comment on the new classification of surgical treatment of spinal tuberculosis. Int Orthop. 2009;33:291-2.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical management and outcome of tuberculous atlantoaxial dislocation: A 15-year experience. Neurosurgery. 2003;52:331-8.
- [CrossRef] [PubMed] [Google Scholar]
- et al. Surgical treatment of thoracolumbar spinal tuberculosis-a multicentre, retrospective, case-control study. J Orthop Surg Res.. 2019;14:233.
- [CrossRef] [PubMed] [Google Scholar]




